Article Text

Abstract
Introduction Biologic and small-molecule therapies have revolutionised the treatment of moderate-to-severe inflammatory bowel disease (IBD). A significant proportion of patients experience early or delayed treatment failure. Patients with IBD with greater visceral obesity are less likely to respond to biologics. Sarcopenia has been identified as a predictor of disease severity and need for rescue therapy in acute severe ulcerative colitis. The aim of this study is to assess the feasibility of a physician-derived exercise programme in patients with IBD commencing biologic or small-molecule therapy in addition to the effect on physical fitness, body composition and objective measures of quality of life, fatigue scores and disease activity.
Methods and analysis This is a randomised controlled feasibility study comparing the effects of a physician-derived exercise programme and standard medical care (biologic/small-molecule therapy) with standard care alone in patients with moderate to severe IBD. Patients with IBD in the intervention group will undergo a structured exercise programme for 20 weeks. Both IBD groups will carry out body composition, disease activity and quality-of-life assessments at baseline, week 12 and week 26. The primary objective is to assess the feasibility of the physician-derived exercise programme in patients with IBD commencing disease-modifying therapies. Secondary endpoints include a change in cardiorespiratory fitness, disease activity/inflammation, fatigue, health-related quality of life outcomes and body composition between the two IBD groups. Exploratory endpoints include validation of anterior thigh ultrasound for sarcopenia screening, assessment of proinflammatory cytokines and markers of immunometabolism.
Ethics and dissemination This study has received ethical approval from the Beaumont Hospital Ethics committee on 22 October 2021 (reference number 21/21). Data generated or analysed during this study will be published as an article and supplementary appendix in relevant medical journals. The data will also be presented at national and international conferences.
Trial registration number NCT05174754.
- inflammatory bowel disease
- ulcerative colitis
- crohn's disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Exercise is safe in patients with mild to moderate inflammatory bowel disease (IBD). Sarcopenia is common in patients with IBD and present in over 40% of patients. Anterior thigh ultrasound (US) has been validated for sarcopenia screening in rheumatoid arthritis to detect low muscle mass.
WHAT THIS STUDY ADDS
This study is the first of its kind to enrol patients with IBD with severely active disease commencing disease-modifying therapies to a supervised exercise programme. It aims to examine the immunometabolic response to exercise in patients with IBD and to validate thigh US as an early predictor of low muscle mass in patients with IBD.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study will provide evidence for the wider introduction of a prescribed exercise programme in the management of patients with IBD with moderate–severe disease activity. It will validate anterior thigh US as a readily available screening tool for early sarcopenia detection in IBD and provide insight into modulation of immunometabolic pathways by supervised exercise.
Introduction
Biologic (monoclonal antibodies) and small-molecule therapies have revolutionised the treatment of moderate-to-severe inflammatory bowel disease (IBD) and are frequently used as first-line therapy in moderate-to-severe IBD.1–3 Despite significant advances in IBD therapeutics, a significant proportion of patients experiences a primary or secondary loss of response to treatment.4 5
In keeping with temporal trends, 20–30% of patients with IBD are obese and previous data have shown that patients with IBD with greater visceral obesity are less likely to respond to biologics, have worse outcomes including postoperative complications and are at greater risk of other chronic diseases.6–8 Adipocytes exposed to intestinal microbiota that permeate a compromised intestinal epithelial barrier produce proinflammatory and anti-inflammatory cytokines, some of which attract macrophages, which in turn produce proinflammatory cytokines, including interleukin (IL)−6 and tumour necrosis factor (TNF)-α.9–11
Lean muscle mass is also compromised in chronic inflammatory states. Rates of sarcopenia are high in patients with IBD despite improvements in pharmacological treatments.12 Sarcopenia is classically associated with older persons and is characterised by both a loss of skeletal muscle mass and function.13 Low muscle mass and strength (sarcopenia) have been identified as a predictor of disease severity and need for rescue therapy in acute severe ulcerative colitis (UC).14 Myopenia (muscle wasting) has been shown to be associated with primary loss of response to anti-TNF therapy in patients with Crohn’s disease (CD).15 Anterior thigh US for the detection of the early loss of muscle mass as part of sarcopenia screening has been recently validated in rheumatoid arthritis.16 Regional loss of muscle mass may occur earlier than total muscle loss; therefore, the use of anterior thigh US may detect low muscle mass earlier than conventional imaging (CT, MRI, bioelectrical impedance analysis (BIA) or dual energy X-ray absorptiometry (DEXA)).17
Current evidence suggests that exercise exhibits an anti-inflammatory effect through the induction of anti-inflammatory cytokines, predominantly mediated by IL-6 released from skeletal muscle during exercise, which, has inhibitory effects on TNF-alpha production.18 19 Alteration in metabolism is also a key component to the pathogenesis of IBD and an increasing volume of studies have shown the effect of metabolism on regulating immune cells. Exercise is recognised to regulate metabolism and is a promising adjunctive therapy for management of autoimmune disorders through modulation of immunometabolic pathways, achieving an anti-inflammatory state while also enhancing well-being among subjects.20 Few studies examining exercise in IBD have assessed effects on validated IBD activity markers or inflammatory biomarkers. Those studies have shown an increase in fitness, bone mineral density and a decrease in IBD-related induced stress and anxiety.21 One randomised study measured proinflammatory cytokines before and after prescribed exercise did not see a significant difference in cytokine levels, likely as a result of patients recruited being in clinical remission.22
The type of exercise interventions previously studied in IBD varies from moderate-intensity aerobic and resistance training (the majority of studies) to walking, running, yoga and high intensity interval training.22–24 Limited studies have previously shown that moderate-intensity combined aerobic and resistance training is safe in unfit patients with IBD with quiescent disease and can quickly achieve favourable body changes without adverse effects.22 A previous pilot study examining in adults with CD during a 17-month period found no serious exercise-related adverse events and had a high completion rate of 89–97%.23
ExWell Medical is a novel community-based exercise programme for individuals with chronic disease in Ireland. It offers group exercise classes with medical oversight for people with a range of chronic diseases, including cardiovascular disease, pulmonary disease, diabetes and cancer. The programme is a significant resource for healthcare professionals and individuals living with chronic disease and hosts approximately 700 participant visits per week.25 26
The design of this study aims to investigate the feasibility and impact of an adjuvant intervention in the form of a community-based physician-delivered and supervised exercise programme in combination with best medical therapy in patients with active IBD. We hypothesise that the physician-derived exercise programme may be associated with synergistic induction of an anti-inflammatory response with alteration of immunometabolic pathways and cytokine response. To our knowledge, there are no published studies investigating the effect of a physician-derived exercise programme on patients with active moderate–severe IBD commencing biologic or small-molecule therapy.
Methods and analysis
Study objectives
The primary objective is to assess the feasibility of the physician-derived exercise programme in patients with IBD commencing disease-modifying therapies including:
The recruitment, retention and adherence rates in both IBD arms.
The frequency and nature of adverse events.
Potential barriers to exercise in patients with moderate–severe disease.
Secondary objectives
To demonstrate that the exercise programme will result in a clinically significant increase in cardiorespiratory fitness (15% improvement in 6 min walk test (6-MWT)) when compared with standard medical care alone.
To assess disease-related outcomes attributed to the exercise programme:
Improved response to induction with biologic or small molecule therapy.
Improved overall disease control/inflammation.
Changes in body composition.
Changes in hand-grip strength.
Changes in health-related quality of life (HRQoL).
Changes in fatigue score.
Exploratory endpoints
To estimate the response of proinflammatory cytokines to the prescribed exercise programme and the effect of prescribed exercise on markers of immunometabolic pathways.
To validate the use of anterior thigh ultrasound (US) as an imaging modality to detect the presence of early loss of muscle mass and subsequent response to exercise.
To carryout subgroup analysis looking at the difference in inflammatory response and body composition in patients with CD versus UC.
Study design
The study is a single-centre three-arm prospective randomised non-blinded controlled feasibility study of the impact and feasibility of a physician-accredited 20-week exercise programme in patients attending a tertiary IBD referral centre in Ireland with active IBD undergoing induction therapy. Eligible patients with IBD will be recruited 1:1 to exercise intervention plus standard medical care or standard care with medical therapy alone. The investigators will recruit a third group of healthy controls for comparison of baseline body composition and inflammatory markers. The flow of the study is seen in figure 1. The study has been registered with Clinicaltrials.gov. The Standard Protocol Items: Recommendations for Interventional Trials checklist was followed when developing the study protocol.
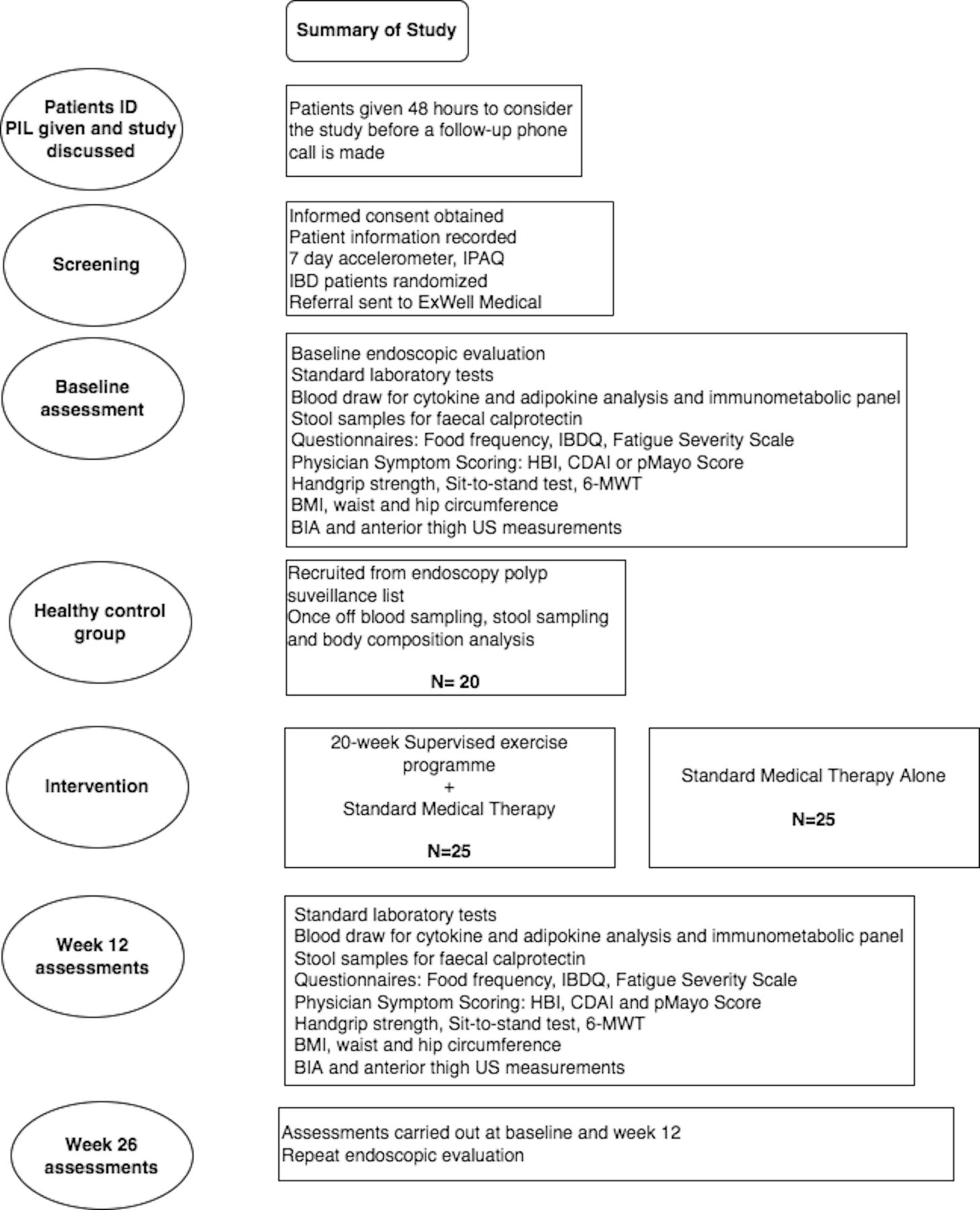
Study flow diagram. BIA, bioelectrical impedance analysis; BMI, body mass index; CDAI, Crohn’s Disease Activity Index; HBI, Harvey-Bradshaw Index; IBDQ, Inflammatory Bowel Disease Questionnaire; 6-MWT, 6-minute walk test; US, ultrasound, PIL- patient information leaflet.
Patient and public involvement
Patients with IBD at two sites (Beaumont Hospital and Connolly Hospital) were surveyed to identify the need for an exercise programme based on physical activity levels, barriers to exercise and willingness to participate in the programme once available. Patients attending outpatient clinics, infusion suites and admitted with disease flares were asked to participate. The survey included specific binary questions asking (1) whether patients would avail of personalised exercise advice and (2) whether they would be interested in participating in a physician-supervised exercise programme. Patients responded favourably, with 75% indicating their interest in participating in a supervised exercise programme.
Study setting and population
The study is being carried out in the Department of Gastroenterology, Beaumont Hospital and is sponsored by the Royal College of Surgeons in Ireland, Dublin (RCSI). Eligible participants will be identified from the IBD clinic and inpatient ward (table 1). A diagnosis of moderate–severe IBD will be confirmed (by endoscopic evaluation and/or faecal calprotectin). Blinding of patients, data collectors and physiological assessors is not possible due to the nature of the study. The intention-to-treat principle will be followed.
Participant inclusion and exclusion criteria.
Trial subjects
Intervention arm: IBD participants enrolled in the study who are randomised to the intervention arm will be referred to ExWell Medical to part take in a 20-week community-based exercise programme (described below). IBD participants in the intervention arm will receive best medical therapy in addition to the exercise programme. Measurements of physical fitness, anthropometrics, body composition, thigh US, blood sampling and questionnaires will be carried out at baseline, 12 and 26 weeks (table 2).
Outline of outcome measurement assessment time points for patients with IBD
IBD control arm: IBD participants who are randomised to the standard of care group will receive best medical therapy and will be advised to continue their usual level of physical activity. Measurements of physical fitness, anthropometrics, body composition, thigh US, blood sampling and questionnaires will be carried out at baseline, 12 and 26 weeks (table 2).
Healthy control arm: a third group of healthy controls attending for elective endoscopic colonic polyp surveillance will be recruited for comparison of baseline body composition and inflammatory measurements. Patients will undergo once-off anthropometrics, body composition, thigh US, blood sampling and questionnaires.
Exercise protocol
The ExWell Medical programme will offer both an in-person and virtual format (via the Zoom platform) for recruited patients. Patients randomised to the exercise plus standard medical therapy arm will be asked to participate for 20 weeks and will be invited to continue to participate beyond this period if they wish. This programme caters to each patient’s physical fitness and ability with a focus on developing sustainable exercise habits to positively impact long-term health. Participants will complete an induction to the programme, which involves (1) information on the programme purpose, structure and logistics, (2) baseline assessments and (3) a brief demonstration of an exercise class.
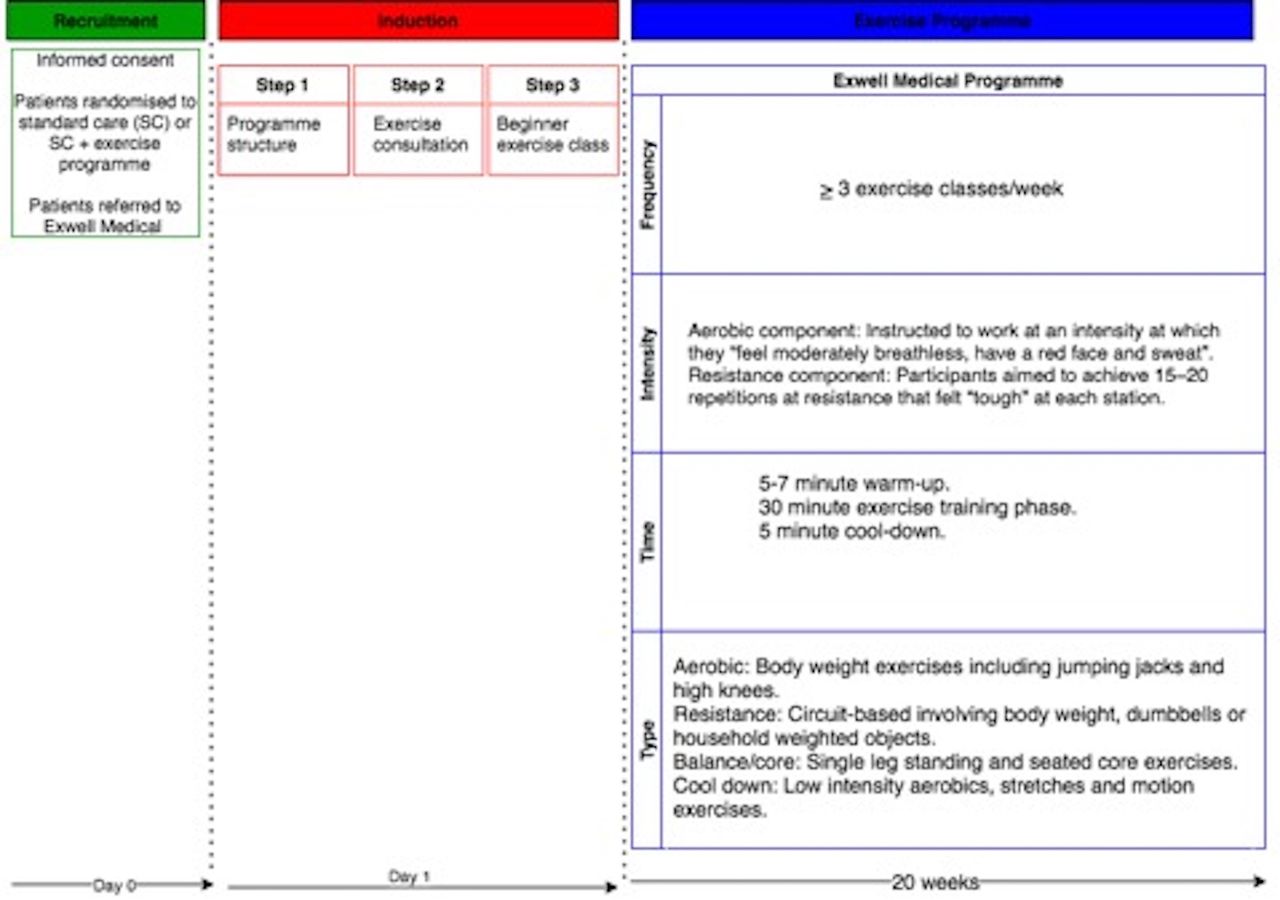
The ExWell Medical exercise intervention is described subsequently using the frequency, intensity, time, type principle (figure 2).25 26
{kind=link}
{kind=link}
Exercise protocol by fitness, intensity, time, type (FITT principle).
1.Frequency
Participants will be advised to attend ≥3 supervised group exercise classes per week and encouraged to attend the same classes every week to foster social support and habit formation.
2.Intensity
For the aerobic component of the exercise classes, participants will be instructed to work at an intensity at which they ‘feel moderately breathless, have a red face and sweat’. For the resistance component of the exercise classes, participants aim to achieve 15–20 repetitions at resistance that feel ‘tough’ at each station.
3.Time
The class includes a 5–7 min warm-up followed by a 30 min exercise training phase and a 5 min cool down. The 5 min warm-up will be followed by 10 min of aerobic exercises followed by 10 min of circuit-based resistance exercises, 10 min of balance/core exercise and a 5 min cool down.
4.Type
The aerobic component of the exercise classes will involve body weight exercises including jumping jacks and high knees. Resistance training will involve circuit-based exercises that include upper and lower body exercises using body weight resistance, dumbbells or household weighted objects. Balance/core exercises will include single leg standing exercises and seated core exercising using a chair. The cool down will consist of low-intensity aerobics and range of motion exercises and stretching (table 1). Adherence to the programme will be monitored as the number of sessions attended.
Outcome measurements
Baseline physical activity assessments
The validated WHO International Physical Activity Questionnaire short form will be used to determine participants’ most recent physical activity patterns prior to randomisation. It is a self-reported or telephone-administered questionnaire that details the participants physical activity in the previous 7 days.27 28
Accelerometers will be worn at baseline for 7 days prior to randomisation of participants. Axivity AX3 monitors will be assigned to patients to wear on their non-dominant hand and the AX3 OMGUI Configuration and Analysis Tool will be used to analyse the recorded data.29
Continuous physical assessment
3. 6-MWT: participants will be instructed to cover as much distance as possible in 6 min while walking, running or a combination, back and forth on a flat indoor 30 m course. Participants will receive a standard set of instructions adapted from the American Thoracic Society guidelines for the 6-MWT . No warm-up will be permitted. The position on the 30 m course at which the participant stops at the end of the 6th minute will be marked with a cone and the distance covered in the final partial lap will be measured to the nearest metre using a measuring tape. The total distance covered will be recorded.30
Disease activity
Physicians will complete validated disease-specific symptom scores including the Harvey-Bradshaw index and the Crohn’s Disease Activity Index for patients with CD and a partial Mayo score for patients with UC.31–34
Blood markers of inflammation-c-reactive protein (CRP), serum albumin and platelets in addition to full blood count, renal, bone and liver profiles.
Stool markers of inflammation-faecal calprotectin.35 36
Endoscopic evaluation will be performed at baseline and at 26 weeks to determine endoscopic response as per current standard of care including intestinal mucosal biopsies.
Body composition analysis and assessment of sarcopenia
Muscle strength and function
Hand-grip strength: measured using both arms with a hand-held dynamometer (Jamar 5030J1 Hydraulic Hand Dynamometer). Patients are sitting on a chair with a back support with their shoulder abducted and neutrally rotated. The angle of the elbow is at 90° and the feet are flat on the floor. The average of three attempts will be recorded for both arms.
Sit-to-stand test: participants sit on a chair with arms crossed, feet flat on the floor parallel to each other, approximately one shoulder width apart. They then stand up and sit down for five repetitions as quickly as possible and are asked to extend their legs on each stand. The time taken to perform five repetitions is timed.37
Other: 25–0 hour vitamin D: low levels of vitamin D have been shown to be associated with the presence of sarcopenia and a reduction in muscle strength.38 39 We aim to measure vitamin D levels at baseline (for all three groups) and at 12 and 26 weeks for patients with IBD.
Muscle mass measurements and body composition analysis
Anthropometrics: height and body mass measurements will be carried out using a stadiometer and electronic scale (model 707 balance scales: Seca GmbH, Hamburg, Germany). Body mass index calculated as body mass in kilograms divided by squared height in metres. Waist and hip circumferences will be taken using a tape measure.
BIA: will be carried out on all patients with IBD (at baseline, 12 weeks and 26 weeks) to determine skeletal muscle mass (kg), body fat % and visceral adiposity (kg). It will also be carried out on healthy controls. The Seca 525 mBCA medical body composition analyser with Seca analytics 115 will be used by the investigators.40 BIA readings will be used to calculate cut-off values using receiver operating characteristic (ROC) curve analysis for anterior thigh muscle measurements from anterior thigh ultrasound imaging and to validate the findings of anterior thigh muscle US.16 41
Anterior thigh muscle ultrasound: will be carried out to measure thigh muscle thickness (MT) as a surrogate for muscle mass. Participants will be in the supine position on the examination table, with the legs extended in a relaxed position. B-mode ultrasound will be used (US LOGIQ emachine 12 L, MSK probe setting and a frequency range of 7-12MHz). The anterior superior iliac spine (ASIS) will be palpated as a landmark. Using a measuring tape, the midpoint from the superior border of the patella to the ASIS will be identified and marked with a surgical pen as the main reference point. Measurements will be taken from the right leg, the most common dominant side. The ultrasound probe will be gently set in transverse plane on the anterior thigh, over the region of the quadriceps muscle group with appropriate amount of ultrasound gel to create a good acoustic window. The probe will be carefully set on the thigh so that it will not directly touch the skin to push the soft tissue. MT is defined as the distance between the anterior fascia of the rectus femoris muscle and the posterior fascia of the vastus intermedius muscle. US measurements will be carried out by a senior physician specifically trained in anterior thigh ultrasound or by a senior radiology trainee, for the purpose of this study.16 41 42
Health-related outcomes (QOL, fatigue scores)
The Short Inflammatory Bowel Disease Questionnaire is a HRQoL tool measuring physical, social and emotional status (score 10–70, poor to good HRQoL). Ten items are included in the questionnaire, all scores are reported with a 7-point scale (1=poor HRQOL, 7=optimum HRQOL) and scores from each item are summed to produce a total score.43
The fatigue severity scale (FSS): FSS is a unidimensional instrument, which includes nine items, with a score of 1–7 for each item. The FSS total score is the mean score of the nine items and a higher FSS score indicates greater fatigue. Significant fatigue has previously been defined using a cut-off FSS score of 3 or 4.44–46
Exploratory outcomes
Markers of immunometabolism
Whole blood will be collected and stored at −80°C for subsequent flow cytometry using cryogenic vials and cytodelics whole blood stabiliser (1:1 dilution of stabiliser with blood per vial). Flow cytometry will be performed to analyse peripheral blood mononuclear cells including macrophages and lymphocyte subsets, which include T helper cells (CD4+, CD8+). Prototypic markers of cellular activation and metabolism, nitric oxide, arginase-1 and arginase-2 will also be assessed by flow cytometry.
Circulating proinflammatory cytokines and adipokines
Blood samples will be prepared prior to running an ELISA: venous blood will be drawn using Sarstedt serum clot activator tubes and centrifuged as per manufacturer’s instructions. Isolated serum will be aliquoted into coded centrifuge tubes in volumes of 500 µL per tube and immediately frozen at −80°C. Serum cytokine analysis will be carried out, which will include the measurement of serum IL1-Beta, IL-6, IL-8, IL-10, IL-17, IL-23, sTNFRII and adiponectin using a custom AssayGenie Multiplex ELISA assay as per the manufacturer’s instructions by flow cytometry. Serum leptin, ghrelin and TNFα will each be measured using separate single ELISA kit assays as per the manufacturer’s instructions.
Sample size calculation and randomisation process
Sample size
As this is a feasibility study, no formal sample size calculation was performed. This study follows sample size recommendations for feasibility/pilot randomised controlled trials. We aim to recruit 25 participants to each IBD group and 20 healthy controls (ie, total sample size of 70), which follows the Sim and Lewis rule of thumb for pilot study sample size calculation of>50 patients.47
This number of participants is deemed adequate to provide sufficient information on important feasibility issues such as recruitment, retention and acceptability of the exercise programmes.
Randomisation process
Randomisation is to be carried out using computer-generated sequencing. Sealed envelopes will be used until interventions are allocated. Participants will be randomised in a 1:1 fashion to the exercise programme plus standard of care or standard of care alone. It will not be possible to blind patients to their intervention allocation given the nature of the intervention.
Data collection, management and analysis
Data collection methods and retention
Informed consent and data at the three time points will be organised and collected by a physician carrying out a full-time research degree. Agreed appointment times for completion of all measures will be agreed with participants. Data will be retained for 5 years post-publication.
Data management
Data will be collected on paper case report forms and de-identified. All patients screened for the trial will be assigned a unique participant ID number. A Data Monitoring Committee consisting of two clinicians and an assigned data manager to ensure the validity of the data during the study has been established. Data will be regularly examined for missing and impossible values. The principal investigators will have access to the final data set along with the full-time research clinician. Anonymous patient data may be shared on request. Site visits will be carried out by the sponsor (RCSI) and annual updates will be provided to the Beaumont Ethics Committee.
Statistical analysis
Statistical analysis will be performed using Stata and Minitab. Feasibility will be evaluated by calculating the percentage of people approached who participate in the intervention (recruitment) and the percentage who complete the intervention (retention and adherence). Given the small number of participants, interim analysis for efficacy will not be carried out.
Descriptive statistics will be used to describe the study population and parameters at baseline. Changes in biomarkers will be assessed using Student t tests or the Mann-Whitney U test depending on the distribution of the data. Clinical outcomes will be analysed as between-group differences using analysis of variance (ANOVA) adjusted for baseline and stratification factors and multivariate analysis with Lasso regression used to study associations with improvement in symptoms, muscle mass or outcomes. Mixed linear regression models will be used to examine QoL outcomes. ROC curves and areas under the curve will be used to determine the cut-off values for sarcopenia using anterior thigh muscle ultrasound measurements and BIA muscle mass measurements.
Ethics and dissemination
Ethical approval
This study has received ethical approval from the Beaumont Hospital Ethics committee on the 22 October 2021 (reference number 21/21). Informed written consent will be obtained from all participants.
Data dissemination and data sharing
Data dissemination and data sharing will be prioritised at the end of the study period, all data generated or analysed during this study will be published as an article and supplementary appendix in relevant medical journals. Any changes to the protocol will be updated on clinicaltrials.gov and ethics amendments will be sought where necessary.
Safety reporting
All adverse events will be recorded from the beginning of the study up until the final time point at the 26-week assessment. A designated co-investigator has been identified as the responsible party for reviewing adverse events reported and subsequent determination of the significance, relationship to the intervention and seriousness of the adverse events. Reporting of adverse events will be carried out in accordance with the Royal College of Physicians reporting procedures (sponsoring body). Patients will continue to be monitored in the IBD clinic postcessation of the study and in the rare event that the patient is harmed in any way during the study they are covered by clinical trial insurance and medical indemnity.
Discussion
This study is designed to address the feasibility of an exercise programme in patients with IBD with moderate-to-severe disease undergoing induction with disease-modifying therapies. The potential benefits of exercise as an adjunctive therapy along with the safety of an exercise programme in patients with IBD with severe disease will be explored. In addition to the impact on patient-related outcomes such as fatigue, luminal symptoms and quality of life, we intend to analyse objective metrics, including the impact on serum proinflammatory cytokine profiles and immunometabolic panels to add to current knowledge, while providing evidence-based advice to patients.
Exercise has been shown to be a promising therapeutic intervention to influence metabolism in autoimmune disorders including multiple sclerosis through regulation of immune cells. This is mediated through cytokine secretion, and modulation of metabolic regulators including tryptophan.20 Alteration in metabolism is also a key component to the pathogenesis of IBD and there may be a role of prescribed exercise in modulating metabolic pathways in patients with IBD.
The use of anterior thigh US to measure MT as a surrogate marker of early loss of muscle mass is a novel concept in patients with IBD but has been used effectively in other inflammatory conditions such as rheumatoid arthritis.16 42 US is a convenient, non-ionising and cost-effective imaging modality compared with CT and MRI and can be performed at the bedside.
In conclusion, this study will examine if a physician-derived exercise programme is feasible, safe, improves physical fitness, disease control, response to medical therapy, body composition and quality of life in patients with moderate-severe IBD. Novel aspects of this study are the inclusion of patients with active moderate-to-severe IBD, examining the response to disease-modifying therapies as a secondary endpoint and the use of anterior thigh US to detect early loss of muscle mass. This study will provide evidence for the wider introduction of a prescribed exercise programme in the management of patients with IBD with moderate–severe disease activity.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to thank the inflammatory bowel disease nurses in Beaumont Hospital and the infusion unit in St Joseph’s Raheny for their support with the project. The authors would also like to thank the Physiotherapy department in the RCSI for their input and support.
References
Footnotes
Twitter @karenjboland
Contributors NMG: wrote the paper, project conception, final approval. MH: critical revisions, ultrasound technique conception, final approval. FS: critical revisions, exercise programme conception, final approval. RD: radiology advisor, final approval. MM: radiology advisor, ultrasound technique conception, final approval. JD: scientific advisor, critical revisions, final approval. NM: designed the exercise programme, final approval. AO'T: project conception, critical revisions, final approval. KB: project conception, critical revisions, final approval.
Funding The project has received seed funding from Royal College of Surgeons Ireland (RCSI) 2021 (grant number N/A), Dublin and from the Strategic Academic Recruitment programme (StAR) MD RCSI/Beacon Hospital grant (21218A01). Additional funding was received from Janssen for IBD patient-related research 2020 (grant number-N/A).
Competing interests KB received funding from Janssen for the support of this study.
Provenance and peer review Not commissioned; externally peer reviewed.