Article Text

Abstract
Objective To evaluate the feasibility and diagnostic performance of acoustic radiation force impulse (ARFI) elastography in different omental masses (OM).
Design This was a retrospective analysis of 106 patients with OM defined as omental thickness ≥1 cm, who underwent abdominal B-mode ultrasound (US) and standardised ARFI examinations of the OM between September 2018 and June 2021 at our university hospital. A cytohistological confirmation was available in 91/106 (85.8%) of all OM, including all 65/65 (100%) malignant OM (mOM) and 26/41 (63.4%) of benign OM (bOM). In 15/41 (36.6%) of bOM; cross-sectional imaging and or US follow-up with a mean duration of 19.8±3.1 months was performed. To examine the mean ARFI velocities (MAV) for potential cut-off values between bOM and mOM a receiver operating characteristic analysis was implemented.
Results The MAV in the mOM group (2.71±1.04 m/s) was significantly higher than that of bOM group (1.27±0.87 m/s) (p<0.001). Using 1.97 m/s as a cut-off yielded a sensitivity and specificity of 76.9% and 85.4%, respectively, in diagnosing mOM (area under the curve=0.851, 95% CI=0.774 to 0.928).
Conclusion ARFI elastography is feasible in the omentum and may represent a good non-invasive additional tool in differentiating bOM from mOM.
- GASTROINTESTINAL ULTRASOUND
- IMAGING
- RADIOLOGY
- SURGICAL ONCOLOGY
- TUMOUR MARKERS
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known on the topic?
Differentiation between benign and malignant omental masses using current imaging modalities is often difficult. In many instances an invasive diagnostic approach (tissue biopsy or even surgical exploration) may be necessary for a definite diagnosis.
Acoustic radiation force impulse (ARFI) elastography is a good non-invasive method in characterising tissue stiffness with established guidelines for application in multiple organs.
There is only one study on the use of strain elastography in the omentum, this former study reported differences in stiffness values between benign and malignant omental lesions, however, no studies regarding feasibility and diagnostic potential of ARFI elastography in the omentum exist.
What this study adds?
ARFI elastography is feasible in quantifying tissue stiffness in different omental masses with significant differences in mean ARFI velocities between benign and malignant aetiologies.
How might this study affect research, practice or policy?
ARFI elastography may represent a non-invasive and radiation-free adjunctive tool in characterising omental masses.
Introduction
The greater omentum is formed by a double layer of the peritoneum extending from the greater curvature of the stomach and passing anterior to the small intestine before folding back on itself to insert upwards into the transverse colon, it consists of 4 layers and is also known as the gastrocolic ligament.1–3 Galen (128–199 AD) already knew the omentum and believed that it served to keep the bowel warm.4
This apron-like or shield-like structure serves as a boundary to contain intra-abdominal disease processes but also can be a potential conduit for the spread of different pathologies.2 The omentum can store a large amount of fat3 and is also rich in lymphatic tissue and white blood cells enabling this structure which is also known as the ‘ policeman of the abdomen’ to function as an immunological organ.3 In fact, the omental volume can increase dramatically in the presence of inflammation or foreign bodies due to the large number of cells having immunomodulatory and stem cell features, a process known as omental activation.3
The differential diagnosis of omental masses (OM) includes several benign and malignant pathologies like infectious or tuberculous peritonitis, peritoneal carcinomatosis, mesothelioma, lymphomatosis, pseudomyxoma peritonei, omental infarction, haematoma, foreign body granuloma and hernia.1 2 The diagnosis is often difficult due to nonspecific clinical and radiologic features.1
Usually the ultrasound (US) visualisation of a normal thin omentum is difficult,5 however it represents a cost-effective and radiation-free method in the evaluation of ascites and omental pathologies.6–9 It can also be used to guide biopsy of OM.10 11
US elastography is a non-invasive imaging technique for the assessment of tissue stiffness with current established guidelines for hepatic and non-hepatic applications.12–15 Acoustic radiation force impulse (ARFI) is a type of point shear wave elastography (pSWE) which depends on the differences of acoustic wave propagation velocity in different tissues determined by measuring the degree of displacement within a 0.5–1.0 cm box on the US screen, known as ‘region of interest’ (ROI).16
In 2019, the European Federation for Ultrasound in Medicine and Biology published guidelines on the use of elastography in non-hepatic organs.13 However, due to insufficient scientific evidence, guidance on elastography in omental pathologies is currently unavailable. To the best of our knowledge, only one study evaluated the use of strain elastography in omental thickening, and our study is the first to evaluate the use of ARFI elastography as a potential quantitative non-invasive tool in characterising OM based on differences in tissue elasticity.
Patients and methods
This was a retrospective study of 123 consecutive patients with OM between October 2018 and June 2021 who underwent an abdominal US of the omentum with elastographic evaluation using ARFI technology at our tertiary healthcare facility (university hospital). Informed consent was obtained from each patient for the US examination. The inclusion criteria were 1. OM defined as thickness of ≥1 cm in diameter on B-mode US; 2. Valid ARFI measurements; and 3. Confirmation of the diagnosis by cytological/histological examination or clinical follow-up. In total, 17/123 (13.8%) of the patients were excluded due to the absence of diagnostic confirmation, so finally 106 patients were included in the study (figure 1).
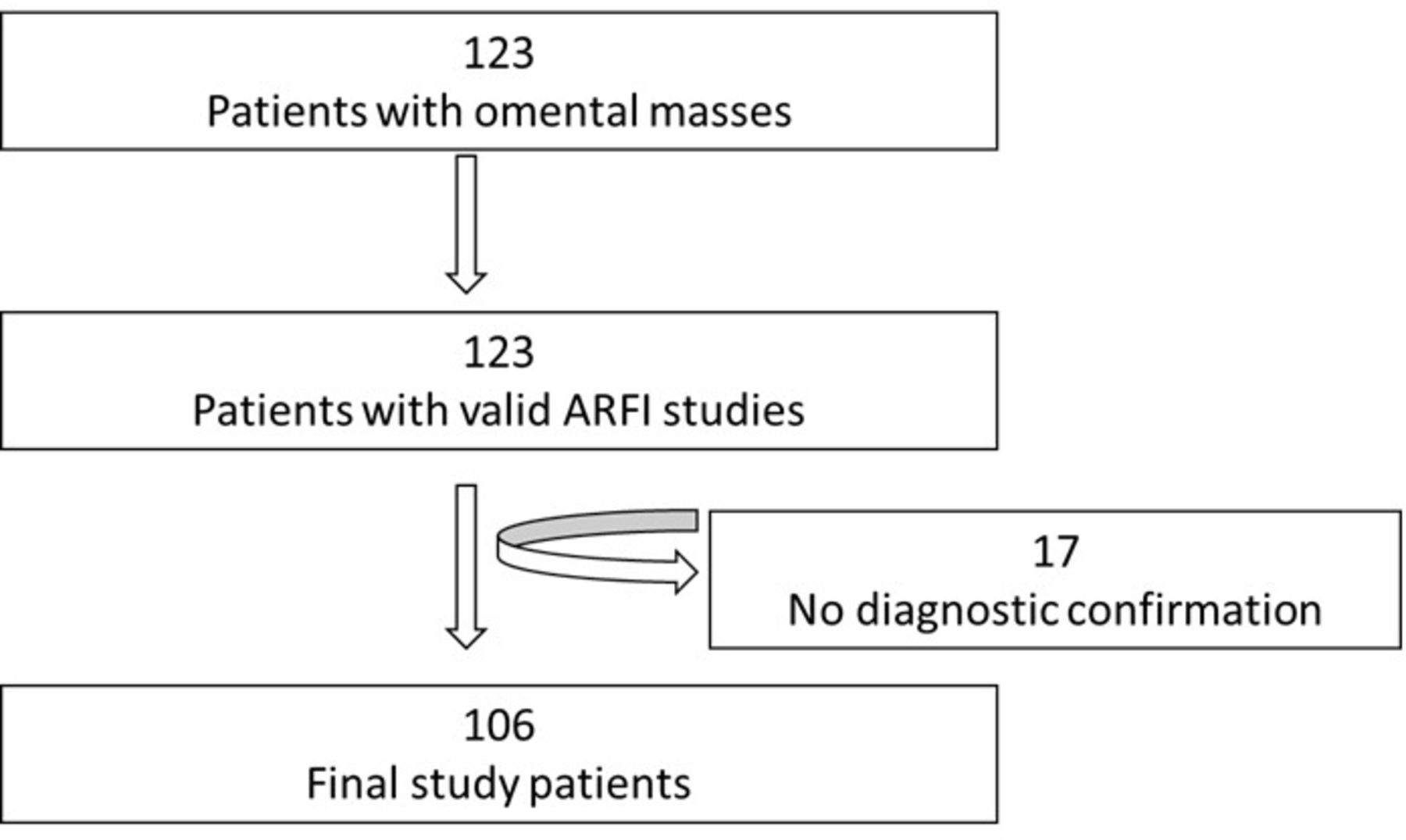
Flow diagram of the study patients. ARFI, acoustic radiation force impulse.
The indications for sonographic evaluation of the omentum were: omental abnormality initially detected on CT/MRI in 31.1% (33/106) or ascites of unknown cause in 31.1% (33/106), and in 37.8% (40/106) of the patients the OM was an incidental finding on sonographic examination performed for other indications.
US examinations
All US and ARFI elastographic examinations were performed using Siemens Acuson S2000, Acuson S3000 and Acuson Sequoia (Siemens Medical Solutions, Erlangen, Germany) by two independent, qualified investigators (ESZ, AA) under the supervision and active participation of a German Society for Ultrasound in Medicine (DEGUM) Level III qualified examiner (CG, internal medicine) with more than 35 years of US experience.17 With the patient laying supine, the curvilinear transducer (6C1) was placed gently on an area of the abdomen where the OM was optimally visualised. Focus and gain were adjusted as needed. The echogenicity of the lesion was classified as hypoechoic or isoechoic/hyperechoic compared with that of the spleen as an in vivo reference. Both echogenicity, and thickness of the of the OM (largest diameter in cm), as well as the presence of ascites were evaluated on B-mode US.
ARFI examinations
The transducer was placed gently on the abdomen, and the depth was adjusted, bringing the OM to the centre of the screen. The ROI (dimensions=10×5 mm) was placed within the mass. For each measurement, the patient was asked to hold their breath in mid-expiration for at least 6 seconds. The measurement was displayed as velocity (m/s) on the upper corner of the screen. If the lesion moved while being measured, this single reading “shot” was considered invalid and was repeated. A total of 11 valid measurements were obtained for each ARFI study.14 15 18 ARFI study was considered valid only if the success rate to obtain 11 measurements was >60%. The mean ARFI velocities (MAV) were registered.
Final diagnosis of OM
Of all OM 65/106 (61.3%) were malignant OM (mOM) and 41/106 (38.7%) were benign OM (bOM). An overview of all disease entities of OM is shown in table 1.
Baseline characteristics and final diagnoses in 106 study patients
Cytohistological confirmation was available in 91/106 (85.8%) of all OM, this included all the 65/65 (100%) patients with the final diagnosis of mOM, in whom cytohistological specimens were obtained using transabdominal US-guided biopsy (48/65; 73.8%), surgery (12/65;18.4%) or paracentesis with positive cytology of the ascitic fluid regarding evidence of tumour cells (5/65; 7.7%).
In 26/41 (63.4%) patients with the final diagnosis of bOM US-guided biopsies were performed. In 15/41 (36.6%), the diagnosis of bOM was based on cross-sectional imaging and or US follow-up. The mean duration of follow-up was 19.8±3.1 months. All the 91 specimens were examined by 2 pathologists with experience in gastrointestinal pathologies at a university hospital. There were no recorded complications related to tissue sampling procedures.
Cross-sectional reference imaging was available in 92/106 (86.8%) of all OM.
Statistical analysis
All statistical analyses were performed using Excel (Microsoft 365 MSO; Microsoft, Redmond, WA, USA) and SPSS V.26.0 statistical software (IBM). Demographic and biometric data were expressed as mean values±SD. Statistical evaluation was performed using a Fisher’s exact test for categorical variables and a Mann-Whitney test for continuous variables. The diagnostic performance was assessed using receiver operating characteristics (ROC) curves. Cut-offs between groups were examined for accuracy using the area under the ROC curve (AUROC) and the 95% CI. A p<0.05 was defined as significant.
Results
Demographics
Of the 106 study patients 43 (40.6%) were males and 63 (59.4%) females. The mean age was 62.1±15.0 years (range 18–87 years). The mean body mass index (BMI) was 26.0±4.5 kg/m2 (range: 16.9–44.8 kg/m2). No significant associations were found between gender, age or BMI and malignancy risk (p>0.05).
US data
Ascites was present in 82/106 (77.4%) patients; in 54/65 (83.1%) patients with mOM and in 28/41 (68.3%) patients with bOM (p=0.1). The mean size of the mOM (2.93±1.25 cm) and that of the bOM (2.48±0.77 cm) did not differ significantly (p=0.07). Regarding echogenicity, 57/106 (53.8%) OM were isoechoic and 49/106 (46.2%) hypoechoic. MOM were more likely to be hypoechoic (44/65; 67.7%) than bOM (5/41;12.2%) (p<0.001).
ARFI data
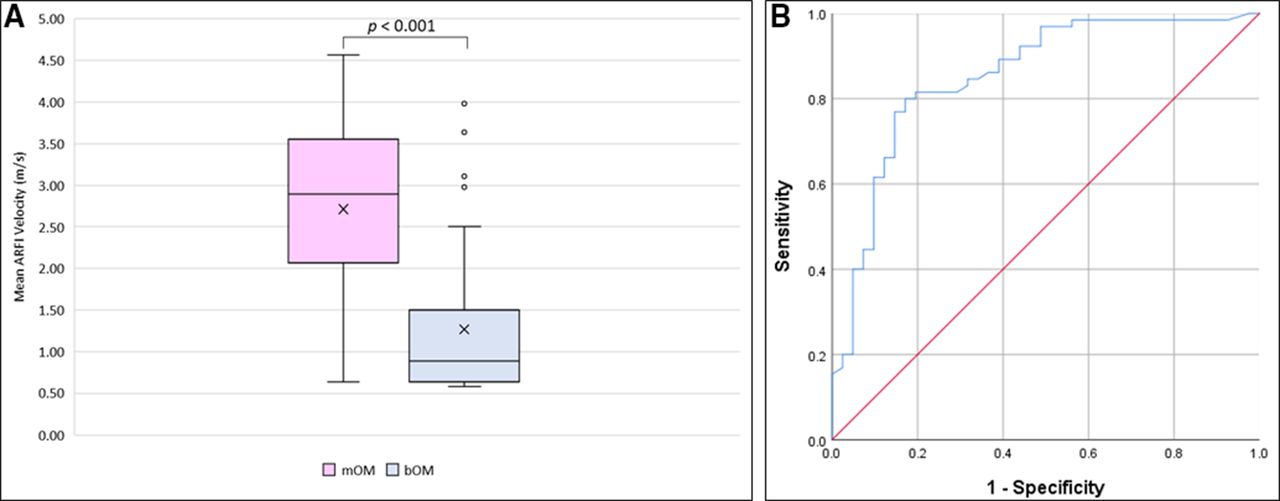
MOM demonstrated significantly higher MAV than bOM (2.71±1.04 vs 1.27±0.87 m/s) (p<0.001) (figures 2 and 3). Using 1.97 m/s as a cut-off would have a sensitivity and specificity of 76.9% and 85.4%, respectively in diagnosing mOM (AUC 0.851, 95% CI 0.774 to 0.928). There were no significant differences in MAV between 19 inflammatory bOM (1.46±0.90 m/s) and 22 non-inflammatory bOM (1.11±0.84 m/s) (p=0.23). There were also no significant differences in the MAV of 24 OM without ascites (2.18±1.20 m/s) and that of 82 OM with ascites (2.15±1.21 m/s) (p=0.82). A boxplot comparing ARFI values among bOM and mOM is shown in figure 4. The MAV of different benign and malignant subgroups are shown in table 2.

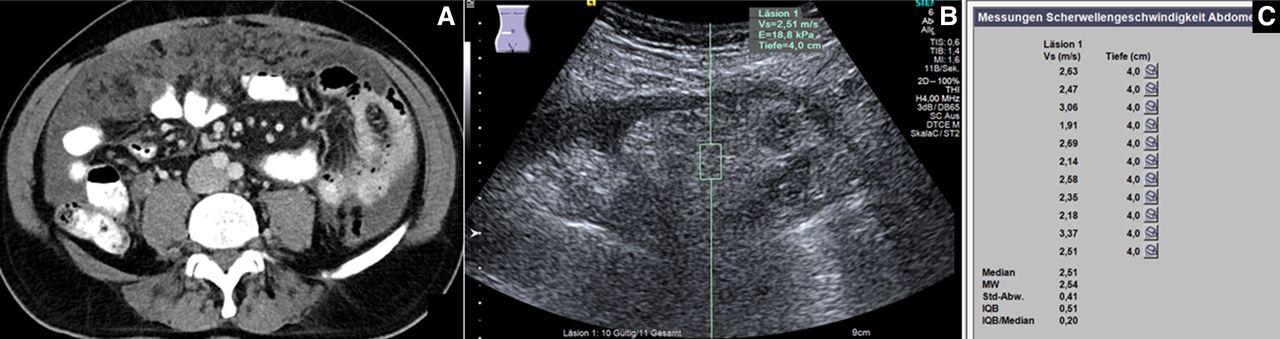
Benign omental mass. A 41-year-old male patient with unexplained ascites; (A) CT scan showing ascites and thickened omentum (courtesy of Professor Dr Mahnken, Department of Radiology, University Hospital Marburg), (B) US elastography image showing a mass-like echogenic omentum in the epigastric area with one ARFI measurement of 0.55 m/s, (C) the final ARFI report of the same mass sowing a mean ARFI velocity (MW) of 0.58 m/s. After surgical exploration, the diagnosis of bacterial peritonitis as a delayed presentation of a perforated subacute appendicitis was established and histologically confirmed.ARFI, acoustic radiation force impulse; US, ultrasound.
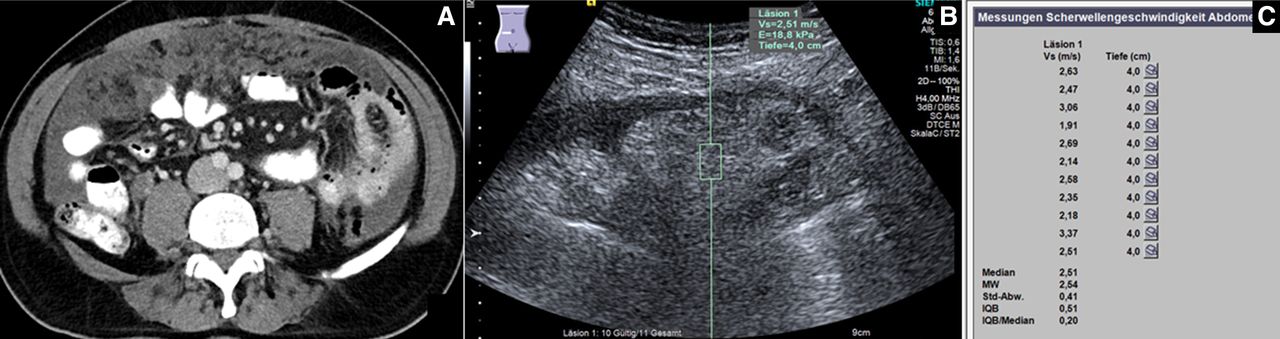
Malignant omental mass. A 51-year-old male patient with unexplained ascites; (A) CT scan showing ascites and inhomogeneous omental mass with multiple nodules (omental caking) (courtesy of Professor Dr Mahnken, Department of Radiology, University Hospital Marburg), (B) US elastography image showing an inhomogeneous multinodular OM in the left lower quadrant with one ARFI measurement of 2.51 m/s, (C) the final ARFI report of the same mass sowing a mean ARFI velocity (MW) of 2.54 m/s. The final histology of the US-guided omental biopsy as well as that of the surgical specimens was diffuse omental and peritoneal metastases from an appendiceal carcinoma. ARFI, acoustic radiation force impulse; OM, omental masses; US, ultrasound.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Differences of mean ARFI velocities between benign and malignant omental masses (mOM) in the study. The mean ARFI velocity (MAV) in m/s is represented with an ‘X’ in each box, and the median ARFI velocity of each group is shown as a horizontal line within each box. (B) Receiver operator characteristic curve for the differences in mean ARFI velocities between benign and malignant omental masses. ARFI, acoustic radiation force impulse; bOM, benign OM.
Comparison of acoustic radiation force impulse (ARFI) data in different bOM and mOM in 106 study patients
Discussion
The omentum is a complex peritoneal fold which functions as an organ. Despite the classical notion of the omentum being merely a ‘fat reservoir’, our understanding of its various immunological and regenerative roles and their clinical applications is evolving.3 There are many benign and malignant diseases which can affect the omentum and the differentiation between such diseases is often difficult.1 7 19 20 In terms of omental imaging, CT scan represents the classical diagnostic modality in omental diseases, however differentiating benign from malignant omental involvement is challenging and the CT signs of fat stranding, nodularity, large masses and omental caking lack specificity.1 Apart from the cost (CT and MRI), radiation exposure (CT) and motion artefacts (MRI) the ability of both imaging modalities in distinguishing postoperative scar tissue from nodular tumour involvement is limited.21
As a cost effective and radiation free method US is a good tool in evaluating ascites and peritoneal carcinomatosis.22 Moreover, US-guided omental biopsy is a safe and effective method in evaluating OM and the cause of ascites.8 10 Salman et al performed US examinations on 100 patients with ascites of unknown aetiology and suggested an omental thickness of ≥19.5 mm to be a predictor of malignancy.6 The size alone was not shown to be specific for malignancy in other studies.7 8 Similarly, in our study there were no significant differences in the mean sizes of mOM und bOM (p=0.07). In one study Trenker et al concluded that the grey scale and contrast enhanced US were not able to differentiate benign from malignant omental lesions.8 In our study, the presence of ascites did not vary significantly among mOM and bOM (p=0.1). However, mOM were more likely to appear hypoechoic (44/65; 67.7%) in comparison to bOM (5/41; 12.2%) (p<0.001).
Previous studies on colour Doppler US could not demonstrate significant differences in the flow patterns between bOM and mOM.9 19
US elastography represents a good non-invasive method in characterising tissue stiffness with various applications in multiple organs,13 however, little is known about its feasibility and diagnostic performance in omental pathologies with only one study evaluating the use of strain elastography in omental diseases.5 In this study, an elasticity strain ratio of 2.6 (using abdominal wall fat as a reference) was proposed as a cut-off between benign and malignant omental lesions with a sensitivity and specificity of 80.3% und 76.6%, respectively.5 Among the limitations of the above-mentioned study were the subjective nature of strain elastography with unavoidable intra- and interobserver variability and semiquantitative assessments of stiffness.23 24 In comparison, ARFI elastography is a quantitative method of tissue elasticity and various studies demonstrated its excellent intraobserver und interobserver reproducibility in different body organs25 26 as well as its feasibility and validity in patients with ascites.27 Indeed, in this study we did not find significant differences in the MAV of 24 OM without ascites (2.18±1.20 m/s) and that of 82 OM with ascites (2.15±1.21 m/s) (p=0.82) suggesting that the presence of ascites did not influence the ARFI measurements in this study, this was also seen in the liver where several studies reported no significant differences of ARFI measurements in the presence of ascites.28–30
In this study, the MAV in mOM was 2.71 m/s with an SD of 1.04 m/s and in the bOM 1.27 m/s with an SD of 0.87 m/s. This difference between bOM and mOM was statistically significant (p<0.001). Using the AUROC and aiming at maximising sensitivity and specificity we suggest a value of 1.97 m/s as a cut-off for mOM (AUC 0.851, 95% CI 0.774 to 0.928), the calculated sensitivity, specificity, positive predictive value and negative predictive value were 76.9%, 85.4%, 89.3% and 70.0%, respectively. This could be a good non-invasive test with moderate sensitivity and specificity in supporting the final diagnosis of OM. Table 3 summarises the reported diagnostic performances of different diagnostic imaging techniques in differentiating bOM and mOM.
Comparison of various imaging modalities regarding their diagnostic performance in differentiating benign and malignant omental masses
The differences of the MAV between 19 inflammatory bOM (1.46±0.90 m/s) and 22 non-inflammatory bOM (1.11±0.84 m/s) were not statistically significant (p=0.23). Some inflammatory bOM in the study demonstrated higher stiffness measurements (MAV >1.97 m/s), this may be due to enzymatic-related fat necrosis (eg, pancreatitis with peritoneal inflammation) with tissue hardening in the form of saponification which can mimic the appearance of malignancy on imaging,31 32 or due to the presence of variable degree of omental scaring and fibrosis, such findings are similar to those encountered during liver elastography in patients with liver fibrosis/cirrhosis16 and those of certain necro-inflammatory lung consolidations.14
On the other hand, low stiffness values (MAV <1.97 m/s) were encountered in some mOM and we think this may reflect the heterogeneous geometrical construction of such tumours.
There are some limitations to this study: First: there are still no validated reference ARFI values for normal omentum. Second: there was no analysis of the intraobserver or interobserver variability, however, various studies demonstrated the reproducibility of ARFI in different body organs.25 26 Third: histological confirmation was not available in 1/3 of bOM and in around 8% of the mOM the diagnosis was based on positive ascitic fluid which indicates but does not certainly prove the malignity of an OM. Fourth: despite being used as a measure of reliability in other organs, the use of the IQR and IQR/median ratio as measures of reliability is not validated in the omentum. Moreover, obtaining an IQR value <60% und IQR/median ratio <30% was not possible in all patients with OM. To ensure validity of ARFI studies 11 measurements with a success rate of >60% were obtained for each examination.33 Fifth: due the retrospective nature of this study, the examiners were not blinded to clinical and radiological data. Thus, further large prospective studies are needed to validate our results.
In conclusion, our understanding of the omental role in health and disease states is continuously evolving. In this study, we demonstrated the feasibility of pSWE using ARFI in quantifying tissue stiffness in different bOM and mOM. We found significant differences in stiffness values between bOM and mOM. ARFI elastography may represent an additional non-invasive diagnostic tool for characterising omental pathologies.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethikkommission desFachbereichs Humanmedizin der Philipps-Universität MarburgProtocol code: EK_MR_09_04_20_görg_1.
References
Footnotes
Contributors AA, ESZ, CG, CT, CFD and LS performed the research; AA, ESZ and CG designed the research study. AA and ESZ analysed the data. AA, ESZ, CG, CFD and CT wrote the paper. All authors approved the final version of the manuscript. AA is responsible for the overall content as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.