Article Text

Abstract
Introduction Barrett’s oesophagus (BO) is common and is a precursor to oesophageal adenocarcinoma with a 0.33% per annum risk of progression. Surveillance and follow-up services for BO have been shown to be lacking, with studies showing inadequate adherence to guidelines and patients reporting a need for greater disease-specific knowledge. This review explores the emerging role of dedicated services for patients with BO.
Methods A literature search of PubMed, MEDLINE, Embase, Emcare, HMIC, BNI, CiNAHL, AMED and PsycINFO in regard to dedicated BO care pathways was undertaken.
Results Prospective multicentre and randomised trials were lacking. Published cohort data are encouraging with improvements in guideline adherence with dedicated services, with one published study showing significant improvements in dysplasia detection rates. Accuracy of allocation to surveillance endoscopy has been shown to hold cost savings, and a study of a dedicated clinic showed increased discharges from unnecessary surveillance. Training modalities for BO surveillance and dysplasia detection exist, which could be used to educate a BO workforce. Qualitative and quantitative studies have shown patients report high levels of cancer worry and poor disease-specific knowledge, but few studies have explored follow-up care models despite being a patient and clinician priority for research.
Conclusions Cost–benefit analysis for dedicated services, considering both financial and environmental impacts, and more robust clinical data must be obtained to support this model of care in the wider health service. Greater understanding is needed of the root causes for poor guideline adherence, and disease-specific models of care should be designed around clinical and patient-reported outcomes to address the unmet needs of patients with BO.
- cancer
- endoscopy
- Barrett's oesophagus
Data availability statement
Data sharing is not applicable as no datasets have been generated and/or analysed for this study. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is known
Dedicated services are a key research priority for patients and clinicians.
Current practice shows poor adherence to biopsy protocols with significant levels of missed dysplasia.
What this literature review shows
There are few studies published; one study to date has shown significantly improved dysplasia detection rates.
One systematic review showed improvement with dedicated services but was based on only a few studies.
Data presented at conferences from units in the UK have shown improved adherence to biopsy protocols and documentation without clarity on transformation impact.
What needs to be done
Large multicentre studies to determine the benefit of dedicated services and look for improved outcomes for patients in real terms: dysplasia detection, oesophageal adenocarcinoma detection and survival.
Cost–benefit analysis should also be performed to show value (eg, quality-adjusted life years).
More should be done to improve training and quality of Barrett’s oesophagus (BO) surveillance.
More must be done to look at BO follow-up care pathways and patient education from the patient perspective and to use patient-reported outcomes to shape practice.
Surveillance has a potentially high environmental impact; work is needed to model the sustainability and carbon impact of different pathways, and whether dedicated services and non-endoscopic sampling methods may help streamline care to those who most need it.
Introduction
Barrett’s oesophagus (BO) is a precursor to oesophageal adenocarcinoma (OAC) with a rate of progression from non-dysplastic Barrett’s oesophagus (NDBO) to cancer of around 0.33% per annum.1 2 Rates of BO are rising in more socioeconomically high-income countries even accounting for advances in endoscopy practice.3 Cancer Research UK states that 59% of all cases of oesophageal cancer are preventable and that it carries a dismal 12% 10-year survival.4
Once BO is diagnosed, patients are offered surveillance endoscopy every 2–5 years, depending on the length of their BO, which is predominantly performed on routine upper gastrointestinal (UGI) endoscopy lists (figure 1).5 Standard reporting of results is expected as per the British Society of Gastroenterology (BSG) guidelines5 and Seattle protocol biopsies (quadrantic samples at every 2 cm of the BO segment) are taken along with targeted samples of lesions.6 All patients newly diagnosed with BO should be seen in an outpatient clinic to discuss their diagnosis according to the BSG guidelines.5 Studies have shown that patients lack disease-specific knowledge and overestimate their cancer risk with corresponding cancer worry.7–9 Retrospective studies suggest endoscopic surveillance of patients with BO improves outcomes,10 11 and adherence to Seattle protocol biopsies has been shown to be important for the detection of dysplasia.12 However, BO surveillance endoscopy has often been shown to be performed inadequately,13 with longer segments routinely underbiopsied.14 Missed dysplasia is common; a meta-analysis showed 25% of OAC is missed at an index BO endoscopy,15 and a UK-based study suggested 12.7% was missed >3 months after diagnosis of BO.16
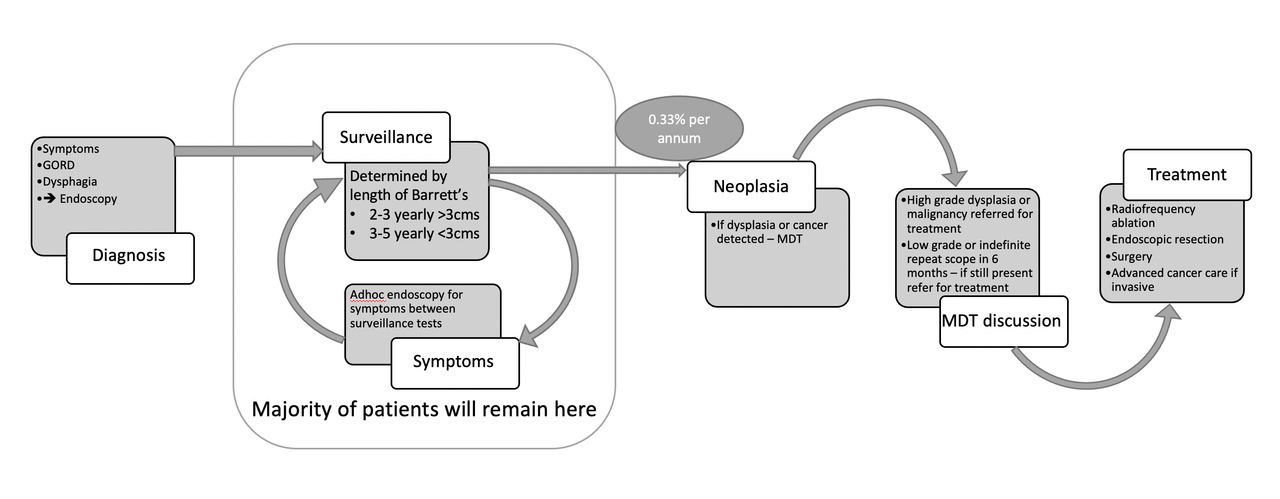
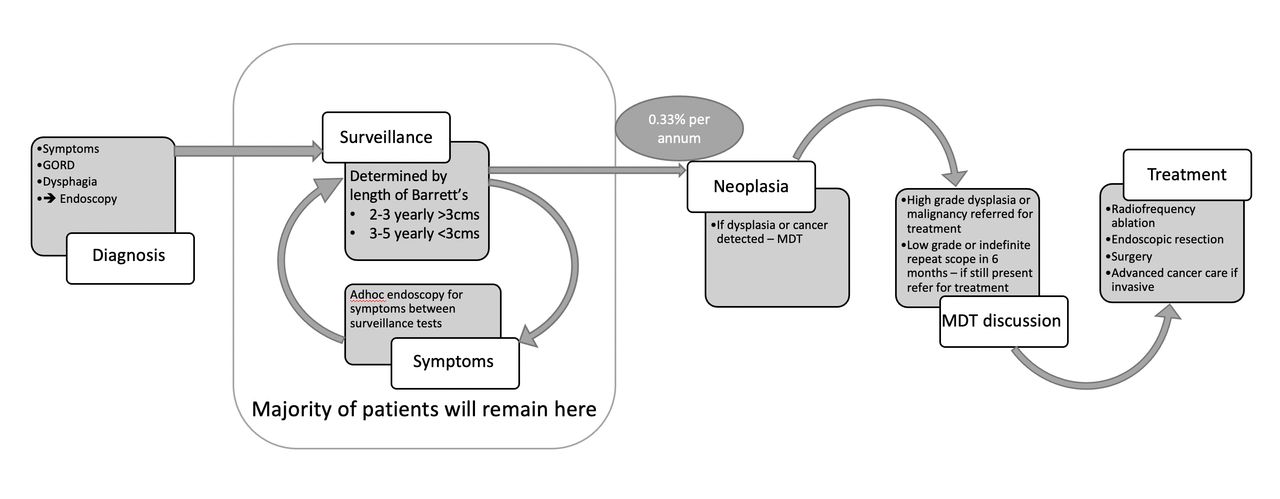{kind=link}
Schematic of a patient journey with Barrett’s oesophagus. The majority of patients will remain in the surveillance programme, presenting with symptoms ad hoc as required. Of these patients, 0.33% per annum may progress to malignancy and dysplasia (Hvid-Jenson et al 1). GORD, gastro-oesophageal reflux disease; MDT, multidisciplinary meeting.
Patients can also be left on routine surveillance inappropriately or surveyed too frequently17; overdiagnosis of BO at the gastro-oesophageal junction is frequent; and the majority of cases with BO will die of another disease than OAC.18 Information and decision making around multicomorbid patients has been neglected in studies, but guidelines advise clinicians to consider this in decisions around initiating and stopping surveillance.5 19 Individual risk stratification methods to aid surveillance decisions are being investigated,20–22 and non-endoscopic oesophageal sampling methods have been devised, which may support streamlining of endoscopy use.
Dedicated BO services as a model of care are recognised in the tertiary setting, with advanced endoscopy for BO lesions centralised in referral centres. However, most initial diagnosis of BO, surveillance and follow-up of NDBO occur in the general setting. A research priority setting exercise published in 2017 was undertaken to determine the top 10 research priorities for BO23; the fourth priority was ‘Should surveillance and new patient clinics for BO be done by a dedicated service? How would this compare with existing standards of practice in the UK, and what effect would this have on patients (eg, precancer diagnosis rates, patient education, quality of life and satisfaction)?’
This review explores how well this priority is covered in the literature at present and the areas of unmet need in BO that a dedicated service could address.
Methods
Using National Institute of Healthcare Excellence Healthcare Databases Advance Search, we performed a literature search of PubMed, MEDLINE, Embase, Emcare, HMIC, BNI, CiNAHL, AMED and PsycINFO to September 2020 was performed. A separate search was performed of the Cochrane database and review articles, and key papers’ reference lists were reviewed for further relevant papers. Search strategy was undertaken as follows: (“dedicated” AND “Barrett’s Oesophagus”), ((“dedicated” AND “Barretts oesophagus”) AND (“clinic” OR “endoscopy”)), (“Barretts oesophagus” AND (“clinic” OR “endoscopy”)), ((“dedicated service” AND “gastroenterology”) AND (Endoscopy OR clinic)), (dedicated endoscopy for Barrett’s oesophagus), (dedicated clinic for Barrett’s oesophagus).
Reinforcing the novel nature of dedicated services for NDBO, we found that there were few fully published studies with no randomised controlled trials and only a few that were multicentre.
Dedicated BO surveillance services
Studies comparing types of Barrett’s services are summarised in table 1. Only one study published in the UK was identified which showed a significant difference in dysplasia detection rate. Ooi et al compared prospective data from two sites on a dedicated service, where four endoscopists who had prior training in the BSG guidelines and lesion detection performed surveillance at the two sites.24 This was then compared with retrospective data from a group of 47 different endoscopists from the same site over the prior 5 years. A total of 729 patients were reviewed; there was a significant difference in dysplasia detection rate (defined to include indefinite for dysplasia, low-grade dysplasia, high-grade dysplasia (HGD) and OAC) of 18 % (26 /142) in group A vs 8% (45/587) in group B (p< 0.001). This study was extremely encouraging, showing markedly improved outcomes; however, there are some limitations; the BSG guideline bisected the retrospective data which could account for the lower figures, and there is a potential the prospective group benefited from this. No data were collected on inspection time, and it is possible the tertiary centre had selection bias with a saturated population with some cases referred in with known dysplasia.
Summary of the comparison studies of dedicated endoscopy versus non-dedicated endoscopy for Barrett’s surveillance including expert centres versusnon-expert centres
Another cohort study by Britton et al compared a single-centre prospective cohort of patients undergoing Barrett’s surveillance, either on a dedicated service (n=217) or a non-dedicated list (n=78).25 The dedicated service was defined as conducted by an endoscopist with a special interest in BO. This service was compared with those who attended lists performed by other operators, and with their retrospective data. Adherence to documentation guidelines was significantly better in the dedicated list with Prague classification reported (100% vs 87.3% vs 82.5%, p<0.0001) and location and number of biopsies (99.5% vs 5.6% vs 6.9%, p<0.0001). Adherence to the Seattle protocol was significantly greater in the dedicated list (72% vs 42% vs 50%, p<0.0001), though this did not translate to significant differences in histology with intestinal metaplasia (IM) (79.8% vs 73.1%, p=0.12) and dysplasia/OAC (4.3% vs 2.6%, p=0.41). More patients were discharged from surveillance from the dedicated list due to comorbidity or performance status (13.4%). This study was a single-centre cohort looking at a small number of patients, with a partly retrospective design, and no inspection time data were reported.
Studies comparing expert centres with non-expert centres
Rather than comparing a specific dedicated service within one trust to prior standard care, some studies have compared the outcomes for specialist or expert centres with community or non-expert endoscopy units. Schölvinck et al 26 reviewed 198 patients who were referred from 37 community hospitals to a Dutch tertiary referral centre. Visible lesion detection was 87% in expert centres vs 60% in community cases. When HGD or OAC was found on a random sample, 76% had a lesion detected by the expert unit vs 50% when repeated in the community.
Cameron et al 27 reviewed 69 cases who had been referred to a specialist BO centre for treatment of dysplasia. Adherence rates were poor in the community setting with 4/25 endoscopists adhering to Seattle protocol; 42% only noted any visible pathology on the referral endoscopy, which compared with 94% in the expert unit (p≤0.001). The expert unit confirmed all the prior known cancers and found an additional 10 cases at mapping. high-definition white-light endoscopy(HD-WLE) was used only in 57% of the community units and 14% used narrow band imaging (NBI), which might account for some of the missed lesions.
Limitations of these studies are that referrals to a specialist centre are a saturated population with known dysplasia, which introduces significant bias. Inspection time during endoscopy is an important factor influencing dysplasia detection,28 similar to colonoscopy adenoma detection; however, it is poorly reported in the aforementioned studies.
Conference abstract data
Given the paucity of published studies, conference abstract data are outlined in table 2.
Summary table of conference abstract data relating to dedicated Barrett’s services
What are the unmet needs of patients with BO which could be addressed by a dedicated service?
Unmet need: clinical factors
Current surveillance practices: what improves outcomes?
A systematic review and meta-analysis published in 2020 reviewed studies pertaining to adherence to BO guidelines.29 Fifty-six studies were included in qualitative analysis and 45 studies were used for quantitative synthesis/meta-analysis. In this collection of international studies, they reviewed adherence to local guidance in a number of domains including total adherence, surveillance intervals, biopsy protocol and use of advanced imaging; landmark identification including length assessment using the Prague classification30; and histopathological results and correlated them with patient, endoscopist and endoscopy unit variables. Adherence ranged from 18% to 89% with the Seattle protocol. Factors associated with better adherence included university hospital endoscopy units, use of a dedicated list or service, shorter segment of BO and endoscopists who were employed as salaried clinicians opposed to those who were dependent on productivity. There was a wide variance in study designs; the studies were influenced by self-reporting of outcomes and country-based factors including different guidelines.
Adjuncts to support dysplasia detection and training the dedicated workforce
Currently, there is no specific assessment for competence in BO endoscopic surveillance beyond Joint Advisory Group accreditation in diagnostic UGI endoscopy. Though the quality Barrett’s endotherapy guidelines and other guidelines for BO exist,31 32 improving adherence to protocols as well as better recognition of visible lesions by a dedicated workforce could improve dysplasia detection.
Training modules for BO dysplasia detection
The International Committee for Oesophagitis created a training module aimed at using videos to train endoscopists to delineate Barrett’s oesophagus-related neoplasm (BORN).33 Named the BORN training module, phase I involved collecting a series of endoscopy videos of NDBO, and dysplastic BO which were annotated by three experts. They delineated any lesions and a ‘sweet spot’ for targeted biopsy. This formed a training series, comprising a test module and four training modules on which participants attempt to match the expert annotations, with mandated feedback between each module. Phase II evaluated BORN on an international cohort of 121 general endoscopists of varying experience. They showed marked sequential improvements between module 1 and module 4 with 46% in detection, 129% delineation and 106% relative delineation. The learning effect was independent of endoscopic expertise or country of origin.
Advanced imaging techniques and acetic acid dye spray
Advanced imaging techniques are a vital part of lesion recognition (eg, NBI, I-scan and volumetric laser endomicroscopy), enhancing abnormal vasculature and mucosal surface patterns, with many hoping targeted biopsies could replace Seattle protocol biopsies.34–36 Dilute acetic acid dye spray which causes a reversible reaction to the BO epithelium with early reversal in dysplastic tissues can be used to help detect dysplasia. It has been found to be cost effective if resulting in targeted samples alone in the surveillance population – particularly in higher risk groups.37 It is cheap and online learning has been shown that non-experts can learn how to use it with training programmes.38 Tholoor et al, using a per biopsy analysis, found a 14.7 -fold increase in neoplasia detection when endoscopists used ascetic acid-guided biopsies.39 An audit in Nottingham showed Seattle protocol still was important even with experts,40 but potentially a dedicated workforce, with adequate training in the use of adjuncts, could improve dysplasia detection.
Artificial intelligence (AI)
AI systems are being used (eg, I-scan and CADDIE) in BO to find dysplasia current methods miss.41–43 Lesion detection in BO is notoriously challenging for the uninitiated, and AI may provide some guidance; however, it requires a skilled workforce to use and interpret the signals from AI devices and to counsel patients about the potential limitations as responsibility remains with the operator.44 Machine learning tools could help to teach a dedicated workforce how to detect dysplasia. Seghal et al used I-scan, an endoscopy machine learning technology from Pentax on high-definition video of endoscopy procedures taken from patients undergoing surveillance.45 The experts reviewed the videos and scored them according to vascular pattern, visible lesions and whether they were non-dysplastic or dysplastic. Non-experts (GI trainees) and non-endoscopists (medical students) were then allowed to score and diagnose the videos, after which they watched a training video on how to detect dysplasia. Following this, they repeated their scoring of the videos. There was significantly improved sensitivity in the trainees’ group (from 71% to 83%) and specificity in the medical student group (from 31% to 49%).
Non-endoscopic dysplasia detection: Cytosponge
The Cytosponge is a mesh sphere on a string which is swallowed in a gelatine capsule, and on withdrawal samples oesophageal mucosa from the length of the oesophagus, is safe and well tolerated by patients.46 Devised initially as a screening tool for primary care to detect the undiagnosed patients with BO in the community, the Cytosponge also provides an opportunity to support BO surveillance and reduce the patient burden, including after endotherapy.47 The Cytosponge-trefoil factor 3 versus usual care to identify BO in a primary care setting: a multicentre, pragmatic, randomised controlled trial (BEST3)48 comparing standard care to Cytosponge in the gastro-oesophageal reflux disease (GORD) population, found a 10-fold increase in BO diagnosis, which raises the concern this may increase the burden of confirmatory endoscopy and endoscopic surveillance. However, work is under way to devise a biomarker panel to risk stratify patients, with the hope that low-risk groups could continue on Cytosponge surveillance alone or be appropriately discharged.49 Cytosponge is also now in use in the known BO surveillance population, which may allow streamlining of endoscopic assessment towards those at highest risk of dysplasia.50 A dedicated workforce is needed not only to assess endoscopically those found to have high-risk features but also to counsel patients about the different modalities and their limitations.
Barriers to quality surveillance: clinician factors
BO publications have often focused on clinical aspects, the performance of surveillance and technologies involved, yet clinician aspects have not been extensively explored. A survey13 of attitudes and practice of BO surveillance in UK gastroenterology clinicians was performed by the research group for the Aspirin and Esomeprazole in Barrett’s Oesophagus (AspECT) trial.51 The research team sent surveys to 401 clinicians with 228 responses, of which 57 were from centres engaged in the AspECT study. They found 90% of responders would perform inadequate biopsy numbers; most would refer HGD to surgery; and 92% stated their lack of adherence to guidelines was due to the poor quality of evidence. In a follow-up survey, there was a significant increase in adherence to guidelines particularly in those engaged with the AspECT trial. Though this survey predated the most recent BSG guidelines, the authors suggest engagement with BO research improves practice, suggesting the important role of education for clinicians.
Barriers to quality surveillance: departmental factors
Inspection time when assessing BO segments improves dysplasia detection.28 There is a strong emphasis on withdrawal times in colonoscopy improving polyp detection, particularly in the bowel cancer screening scenario.52 The quality standards in UGI endoscopy suggest an inspection time of 1 min/cm of BO, yet BO surveillance can often be on varying endoscopy lists without adequate time allocation.32 Streamlining surveillance to those at greatest risk then scheduling them on dedicated lists with adequate time and a trained workforce (both the endoscopist and their team) may provide an environment more conducive to dysplasia detection. Streamlining is key, given the increasing demand on all aspects of endoscopy, which influences scheduling.53
Cost implications of BO surveillance
Accurate use of the BSG guidelines implemented in 2014 has been shown to reduce the number of unnecessary surveillance procedures. At St Georges NHS trust, Hewett et al reviewed the BO population on their surveillance waiting lists, stratified them according to BO length according to the BSG guideline, and reviewed histology to check the presence of IM.54 They estimated accurately allocating surveillance would provide a saving over the subsequent 10 years of £72 033 per annum, projecting across the NHS an approximate £100 million saved. An abstract from 2015 estimated the accurate scheduling of patients in York hospital would free 98 endoscopy slots with an annual cost saving of £53 503.55 Accurate BO scheduling has potentially dramatic cost–benefits, and benefits for patients by avoiding unnecessary invasive procedures; dedicated BO teams could oversee BO surveillance scheduling to facilitate these cost savings.
Beyond financial cost, endoscopy carries a huge environmental impact, from solid waste production, to water required for the processing of scopes, to processing costs of endoscopy samples.56 57 BO contributes significantly to this with 2–5 yearly endoscopic surveillance, Seattle protocol biopsies, with the associated travel and departmental costs. No specific papers were found showing a link between dedicated services, streamlining surveillance and the environment, but it follows that avoiding unnecessary endoscopy and improving the quality of that which is performed may have benefits. Formal life-cycle analysis could be undertaken, exploring all aspects of the BO pathway to understand the full impact.
Unmet need: patient factors
Dedicated BO clinics
Only one study by Anagnostopoulos et al reviewed the outcomes of a BO clinic run by clinicians with an interest in BO.58 Prospective data over 12 months were collected and questionnaires regarding patients understanding of BO were used. In the clinic, 17% had a treatment change, and 11% were discharged from surveillance. Their survey showed 22% of patients had had no information and 10% did not know they had BO with a similar figure believing they already had cancer. A key limitation was that it was an audit of a new intervention without a comparator. Likewise, the questionnaire was a single intervention and did not test for sustained improvements. However, they highlighted important deficits in patient knowledge and showed high discharge rates from inappropriate surveillance.
Britton et al 59 carried out a quantitative study comparing the health-related quality of life of patients with BO, both in non-dysplastic and dysplastic cases post-treatment, with healthy patients, those with GORD and patients with colonic polyps. Eligible cases totalled 687. Key findings were that those with NDBOs reported comparable levels of significant cancer worry (53%) as those who had been treated for dysplastic BO and were clinically at greater risk (50% p=0.933). Patients who accurately perceived their cancer risk as low correlated with low levels of cancer worry, whereas anxiety, depression and cancer worry were significantly associated with worse control of GORD symptoms in patients with NDBO. This suggests that patients require greater support and education to reduce their cancer worry and empower them with knowledge of their actual cancer risk, and that good control of symptoms could help reduce worry and anxiety in this cohort.
A qualitative study in a single centre by the same group using semistructured interviews explored the experience of BO care for patients with NDBO.7 The interviews (n=20) concentrated on follow-up needs, symptom burden both physical and psychological, and impact of the disease and surveillance. The results showed four themes:
Burden of disease, including worry of cancer and endoscopy surveillance
Follow-up care experiences.
Follow-up needs.
Disease-specific knowledge.
Most of the patients reported good symptom control; patients with a more central locus of control were able to manage their cancer worry better. Worry was relieved by good communication from their medical team, particularly early verbal reassurance about their surveillance and prompt biopsy results. When asked about follow-up, initial education and information were deemed inadequate and rushed. Disease-specific information overall was lacking, with most patients looking to other sources to self-educate; written information when provided was welcomed.
When asked about future considerations for follow-up care, patients valued seeing a specialist; most were open-minded to nurse specialist care. They viewed a service run by a BO specialised team encompassing endoscopy and follow-up as more robust .
Other studies echo these findings: Murphy et al showed less than 50% of patients with BO-associated OAC knew about the diagnosis of BO despite multiple prior endoscopies.60 Stier et al 61 found patients with BO overestimated their risk of OAC with their lifetime risk perceived as 19%. These studies suggest there is a burden of inadequate knowledge and cancer worry, dedicated BO follow-up services could provide education, risk counselling and offer a place for patient queries to be addressed beyond their initial diagnosis.
Summary
OAC remains a significant cause of morbidity and mortality with high rates of preventable cases. Early diagnosis and treatment of BO-associated dysplasia and OAC offer an opportunity for improvement. Studies concentrate on interventions and dysplasia detection in the tertiary or specialist environment when more needs to be done to detect dysplasia in all units performing UGI endoscopy and BO surveillance. Early data from many published abstracts show encouraging improvements in adherence to surveillance guidelines with dedicated endoscopy services. However, more peer reviewed, multicentre prospective data looking at dysplasia and OAC detection are required, and there are currently no randomised controlled data. As well as technical factors, there are clinician-related factors which have not been well explored outside of surveys, and clinical endoscopists, trainees and surgeons have been missed from much of the data. Follow-up and education for patients with BO is lacking, and this results in a significant burden of cancer worry. Dedicated, patient-orientated services for BO are needed to address these issues (table 3). Tools to measure the effectiveness of interventions that are specific to this patient group should be developed to make sure advances in technological interventions are not to the detriment of the patient experience. An overhaul of current BO services is required to meet the needs of patients and improve clinical outcomes, with costs savings and reduced environmental burden possible if services are more efficient, and the correct patients are enrolled to surveillance with adequate education and support.
Outline of the unmet need in BO and the role dedicated services could take in addressing these issues
Data availability statement
Data sharing is not applicable as no datasets have been generated and/or analysed for this study. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
Acknowledgments
The authors thank the members of the library team at Salford Royal Hospital, Northern Care Alliance Library Services for support with literature searching.
References
Footnotes
Twitter @lil_ratcliffe
Contributors ER and YA devised the concept of the literature review. ER undertook the literature review and wrote the initial draft of the manuscript. All authors contributed to the review and revision of the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests YA received research funding from Medtronic and Cancer Research UK; ER received research funding from Medtronic.
Provenance and peer review Not commissioned; externally peer reviewed.