Article Text

Abstract
Objective In non-alcoholic fatty liver disease (NAFLD), fibrosis determines the risk of liver complications. Non-invasive tests (NITs) such as FIB-4, NAFLD Fibrosis Score (NFS) and Hepamet, have been proposed as a tool to triage NAFLD patients in primary care (PC). These NITs include AST±ALT in their calculations. Many patients with NAFLD take statins, which can affect AST/ALT, but it is unknown if statin affects NITs fibrosis prediction.
Methods We included 856 patients referred through a standardised pathway from PC with a final diagnosis of NAFLD. 832 had reliable vibration controlled transient elastography (VCTE) measurements. We assessed the effects of statins on the association between NITs and VCTE at different fibrosis thresholds.
Results 129 out of 832 patients were taking a statin and 138 additional patients had indication for a statin. For any given FIB-4 value, patients on a statin had higher probabilities of high VCTE than patients not on a statin. Adjusting for body mass index, diabetes and age almost completely abrogated these differences, suggesting that these were related to patient’s profile rather to a specific effect of statins. Negative predictive values (NPVs) of FIB-4 <1.3 for VCTE >8, 10, 12 and 16 were, respectively, 89, 94, 96% and 100% in patients on a statin and 92, 95, 98% and 99% in patients not on a statin. Statins had similar impact on Hepamet predictions but did not modify NFS predictions.
Conclusion In patients with NAFLD referred from PC, those on statins had higher chances of a high VCTE for a given FIB-4 value, but this had a negligible impact on the NPV of the commonly used FIB-4 threshold (<1.3).
- fibrosis
- fatty liver
- nonalcoholic steatohepatitis
- lipids
Data availability statement
Data may be obtained from a third party and are not publicly available. These data are gathered from Alberta Health services (AHS) sources and our current agreement with Alberta Health services does not allow us to share them without an agreement approved by AHS.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known about this subject?
In non-alcoholic fatty liver disease (NAFLD), the degree of fibrosis determines the risk of adverse liver outcomes.
Serum-based non-invasive test for liver fibrosis are recommended to risk-stratify patients with NAFLD.
NAFLD patients frequently have indication for a statin.
What are the new findings?
We show a low impact of statin treatment on the reliability of three two-step risk stratification strategies used in patients with NAFLD.
How might it impact on clinical practice in the foreseeable future?
Patients on statins can be triaged through the same referral pathways as patients not on statins.
Introduction
Non-alcoholic fatty liver disease (NAFLD) has become the most common aetiology of chronic liver disease worldwide with a pooled estimated prevalence of 25%.1 The main determinant of liver morbidity in NAFLD is the presence of advanced fibrosis.2 3 Indeed, there is an exponential increase in liver related mortality with increased fibrosis stage whereas in patients with no or early fibrosis, the rate of liver related mortality is minimal.3
Non-invasive tests (NITs) are currently used to risk stratify patients with NAFLD needing to see a liver specialist. The current recommendation is to use a two-step strategy with an initial, simple test with high negative predictive value (NPV), such as FIB-4 or NAFLD Fibrosis Score (NFS), followed by a second test with more positive predictive value such as vibration controlled transient elastography (VCTE).4 5 FIB-4, requires age, platelet count and AST (aspartate aminotransferase)/√ALT (alanine aminotransferase) ratio to calculate the score6 and has some theoretical advantages since it can be computed directly from routine laboratory results,7–9 whereas NFS includes albumin and additional clinical information (body mass index, BMI and presence of diabetes/glucose intolerance).10 The recently proposed Hepamet score requires similar variables.11
The prevalence of risk factors for cardiovascular disease is very high in patients with NAFLD.12 13 Furthermore, NAFLD has been suggested to be an independent risk factor for cardiovascular disease.12 14 15 Hydroxy-methyl-glutaryl-coenzyme A (HMG-CoA) Reductase Inhibitors or statins are the mainstay of primary and secondary prevention of cardiovascular disease.16–18 Patients with NAFLD have higher probability of having an indication for statin treatment than patients without NAFLD (~twofold). Previous studies have shown that statins can modify liver transaminases levels, demonstrating both increases or decreases, though the clinical significance of this finding is unclear.19 Since most NITs for assessing liver fibrosis are based on either AST or the calculation of some form of AST to ALT ratio, there is the possibility that statins, by modifying transaminases,20–23 could modify the performance of these NITs in predicting liver fibrosis. Indeed, a common question among primary care providers (PCPs) is if FIB-4 is still valid in patients on statins. In addition, more advanced NAFLD stages are associated with higher prevalence of metabolic risk factors, especially diabetes and dyslipidaemia, which are the main determinants of statin indication.17 24 Thus, assessing the impact of statin treatment on non-invasive prediction of liver fibrosis is critical to understand the performance of these NITs as triage methods in NAFLD referral pathways
The aim of this study was to assess if statins modify NITs predictions of fibrosis (determined by VCTE) in patients referred from PC for NAFLD assessment. A secondary aim was to assess the prevalence of statin indication and current use in patients with NAFLD from our referral base.
Methods
Study population selection
We prospectively collected data from asymptomatic patients referred from PC through a standardised pathway for patients with suspected NAFLD in Edmonton, Canada. Patients were triaged in a nurse-led hepatology triage clinic as previously described.25 This study included patients referred from November 2016 to October 2019.
Clinical, laboratory and VCTE assessment
All patients completed their laboratory tests according to the American College of Gastroenterology to rule out alternative liver diagnosis.26 Medical history was obtained by the Registered Nurse who, in this pilot phase of the referral programme, performed VCTE in every patient. A single operator performed all the VCTE tests with a Fibroscan 502 touch (M Probe or XL Probe; Echosens, France) device. We included in this study patients with a final diagnosis of NAFLD after excluding other potential causes of liver disease.
We considered different thresholds for classifying patients as suspected of having advanced fibrosis based on VCTE: 8 kPa, 10 kPa, 12 kPa and 16 kPa. Each has been proposed to define advanced fibrosis, favouring higher sensitivity and NPV for lower thresholds, or higher specificity and positive predictive value for higher thresholds. The 16 kPa threshold, in addition, has been recently proposed as an indication to initiate hepatocellular carcinoma (HCC) screening.27–31 Unreliable VCTE results were defined as having fewer than 10 valid shots or IQR/median value greater than 30% with a VCTE median of 7.1 kPa or higher.32 Lab values and clinical data were collected from the local EMR and transferred to a dedicated excel database.
Determination of statin indication
We used the Canadian Cardiovascular Society guidelines to evaluate how many patients in our sample had an indication for a statin.17 Details of how patients were classified as requiring a statin are provided in online supplemental material 1.
Supplemental material
Non-invasive tests
The NITs were used as continuous variables. However, we also tested the previously described thresholds for low-risk for fibrosis to assess NPVs. FIB-4 was calculated as described in Sterling et al.6 Patients with FIB-4 less than 1.3 were considered as having low risk for advanced fibrosis, while those with higher FIB-4 values were considered to be intermediate/high risk patients requiring further assessment. Hepamet was calculated as described in Ampuero et al with a threshold 0.12 to define low risk.11 This threshold is roughly equivalent to the 1.3 FIB-4 threshold, according to our previous study showing a pointwise risk of VCTE >8 of ~12% in patients with a FIB-4 of 1.3.25 NFS was calculated as described in McPherson et al with a threshold of −1.455 defining as low risk.7
Statistical analysis
Median (IQR) was used to describe the numerical variables, whereas absolute and relative frequencies were used to describe the categorical variables. The impact of current statin treatment on the association between NITs and different thresholds of VCTE was modelled using logistic regression (detailed in online supplemental material 2). To further assess whether the effect of statins could be explained by the different clinical profile of patients rather than the statin treatment, we conducted additional logistic regression models adjusted by age, diabetes status (classified as normal, pre-diabetes and diabetes), and BMI. To further understand the relation of statin treatment and NITs predictions of fibrosis we used linear regression (detailed in online supplemental material 3). R statistical software (R Foundation for Statistical Computing, Vienna, Austria) was used to conduct the analysis with rms33 and ggplot234 packages.
Supplemental material
Supplemental material
Results
Baseline characteristic of the patients
Of the 934 patients referred to the triage clinic, 856 were classified as having NAFLD. All patients underwent VCTE, and 832 patients had reliable VCTE measurements. Of the 129 patients who were on a statin, 82 were on rosuvastatin, 35 on atorvastatin, 9 on simvastatin and 3 on pravastatin (table 1). One hundred and thirty-eight additional patients had indications for statin treatment according to the Canadian Cardiovascular Society guideline for primary prevention from cardiovascular events but were not on a statin treatment (table 1).
Baseline characteristics of patients with and without indications for a statin who were/were not taking a statin
Table 1 shows the baseline characteristics of the patients, according to whether they were on a statin and whether they had an indication for a statin (vs no indication). Online supplemental material 4 shows the characteristics of those on lipophilic statins (atorvastatin or simvastatin) and those on hydrophilic statins (rosuvastatin or pravastatin). Patients with indications for a statin were older and more frequently had diabetes than patients without indication for a statin. There were no differences in liver enzymes or liver function tests between those with indication and those without indication. For every NIT (FIB-4, Hepamet, NFS and VCTE), the median value for those with statin indication was higher than those without indication for a statin. In addition, the prevalence of advanced fibrosis according to VCTE (using different definitions as shown in table 1) was higher in patients with an indication for a statin than the patients without indication for a statin.
Supplemental material
Patients with an indication for statin but not on a statin had comparable characteristics to those patients that were actually on a statin, except for their lipid profile (table 1).
Effect of statin use on FIB-4 based predictions of VCTE, with thresholds of 8, 10, 12 and 16 kPa
To assess if statins modify FIB-4 based predictions of VCTE, we modelled with logistic regression the association between FIB-4 and VCTE adjusting for statin treatment. For any given value of FIB-4, patients on a statin had higher probabilities of having a VCTE value >8 or 10 kPa (figure 1). Of note, there was no significant interaction between FIB-4 and statins, indicating that the effect of statins on FIB-4 predictions was homogeneous across values of FIB-4.
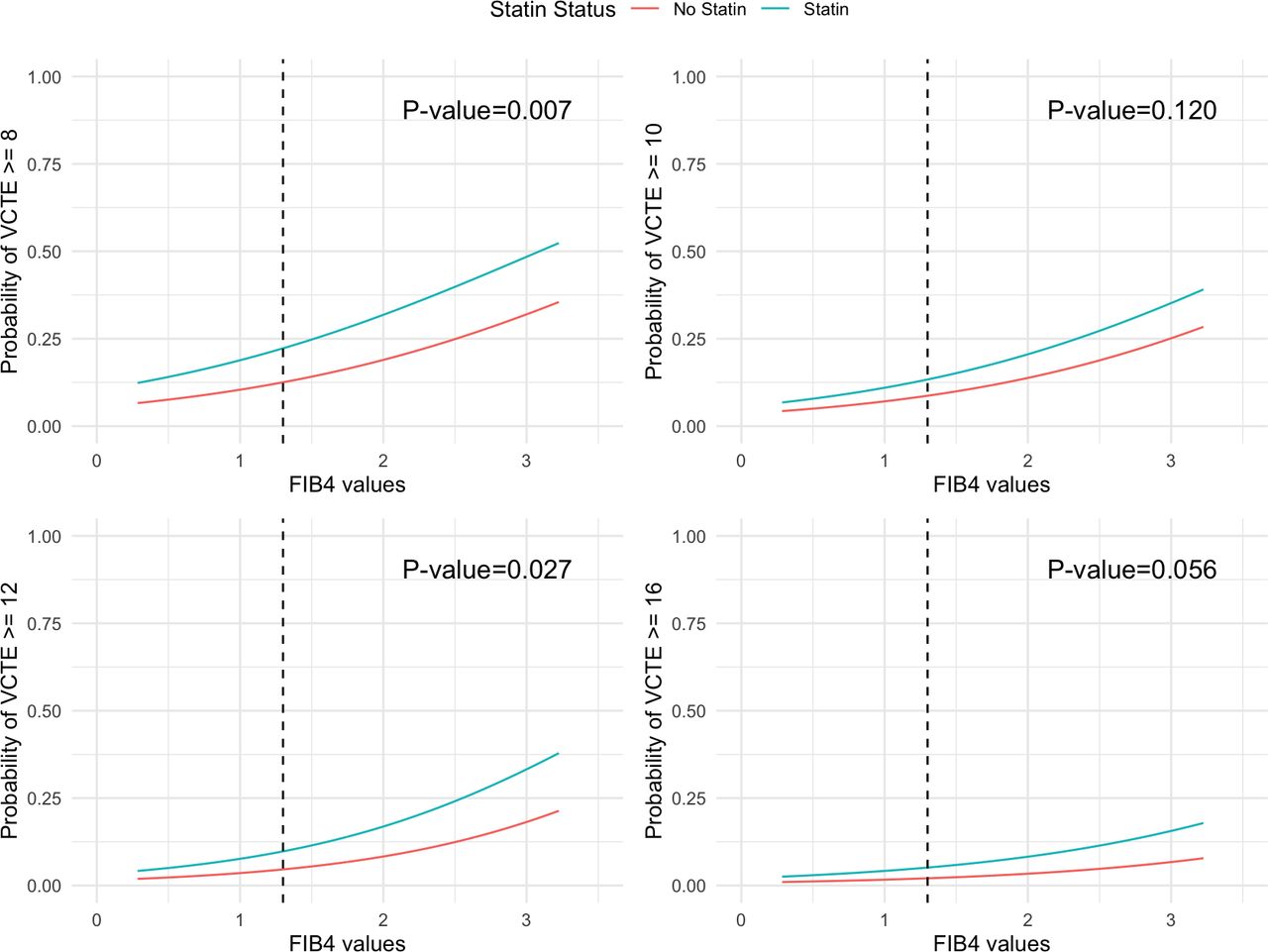
Effect of statin treatment on FIB-4-based prediction of different clinically relevant VCTE thresholds (8, 10, 12 and 16 kPa). Patients taking a statin had a higher risk of having probabilities of high VCTE than patients not on a statin, but this difference attenuated for higher thresholds. VCTE, vibration controlled transient elastography.
We previously showed that age, BMI and diabetes status modify the association between FIB-4 and VCTE.25 In this study the patients on statins were older, had a higher BMI, and more frequently had diabetes (table 1). Thus, to assess if the effect of statins on FIB-4 based predictions were the results of these differences in patient characteristics, we modelled again the effect of statins, in this case adjusting by BMI, diabetes status and age.
After adjusting for BMI, diabetes and age, the effect of statins was markedly blunted. At VCTE of 8 kPa, patients on statins still had higher probabilities of having VCTE >8 kPa, but when higher VCTE thresholds were tested, the difference between patients on statins and not on statins were negligible and non-significant (figure 2).
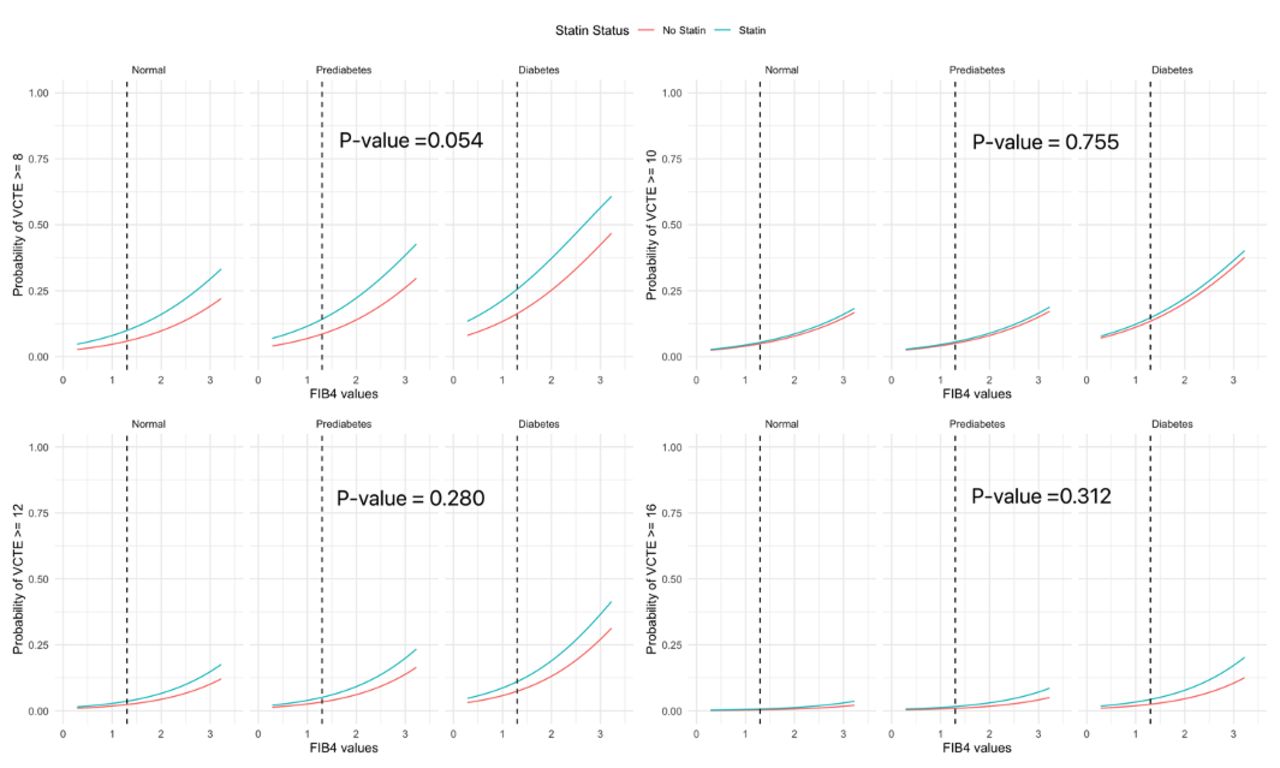
Effect of statin on FIB-4-based prediction of different clinically relevant VCTE thresholds (8, 10, 12 and 16 kPa) after adjusting for age, BMI and diabetes. Adjusting for BMI, diabetes and age almost completely abrogated these differences, suggesting that these were related to patients’ profile rather to a specific effect of statins. BMI, body mass index; VCTE, vibration controlled transient elastography.
To further analyse potential confounding factors by indication, we assessed if statin treatment still altered FIB-4 predictions within the subset of patients with indications for statins (that were comparable in every patient characteristic except for the lipid profile). In this subgroup of patients, the effect of statins on FIB-4 predictions behaved similarly as in the adjusted analysis with the full sample, showing some effect only with the VCTE threshold of 8 kPa. The difference was progressively attenuated with higher VCTE thresholds and became not significant (online supplemental material 5).
Supplemental material
Next, we assessed the impact of statin treatment on the NPVs of FIB-4 <1.3 for different thresholds of VCTE. FIB-4 was <1.3 in 85% of the patients not on statins and 64% of patients on statins. Table 2 shows the NPVs of a FIB-4 <1.3 for different VCTE thresholds. Statins had a small impact on the FIB-4 NPVs for detecting a VCTE <8, which became negligible for VCTE thresholds of 10, 12 or 16.
The difference between NPV of patients with or without a statin among different NITs
Finally, to further understand how statins, BMI, age and diabetes interplay to modify the association between FIB-4 and VCTE, we conducted a multiple linear regression analysis as detailed in online supplemental material 3. For a given value of FIB-4, patients on a statin had only a slightly higher mean VCTE value than those not on a statin but the difference was small and non-significant (p=0.339). BMI had a significant and major impact on the FIB-4-based predictions of VCTE. The higher the BMI, the higher the predicted mean VCTE. In the case of diabetes status, only the diagnosis of diabetes but not pre-diabetes had significant effects on predicted mean VCTE as compared with normal patients. The predicted mean VCTE for a given FIB-4 value was higher in diabetes patients than in patients with pre-diabetes or euglycaemia (online supplemental material 3).
Effect of statin use on Hepamet and NFS-based predictions of VCTE
We additionally tested whether statins impacted Hepamet score and NFS. The effect of statins on the association between Hepamet and VCTE was comparable to that observed with FIB-4. For a given value of Hepamet, patients on statins had higher probabilities of having VCTE >8 compared with patients not on statins. The effect of statins on Hepamet became attenuated for higher clinically relevant VCTE values of 10, 12 and 16 kPa (figure 3). Ninety-one per cent of patients not on statins and 73% of the patients on statins were classified as low risk by Hepamet (<0.12). Table 2 shows the NPVs of Hepamet <0.12 for different VCTE thresholds for liver fibrosis and these predictions were minimally impacted by statins.

Effects of statin on Hepamet-based prediction of different clinically relevant VCTE thresholds (8, 10, 12 and 16 kPa). Patients taking a statin had a higher risk of having probabilities of high VCTE than patients not on a statin, but this difference attenuated for higher thresholds. Vertical dashed line represents the 0.12 threshold. VCTE, vibration controlled transient elastography.
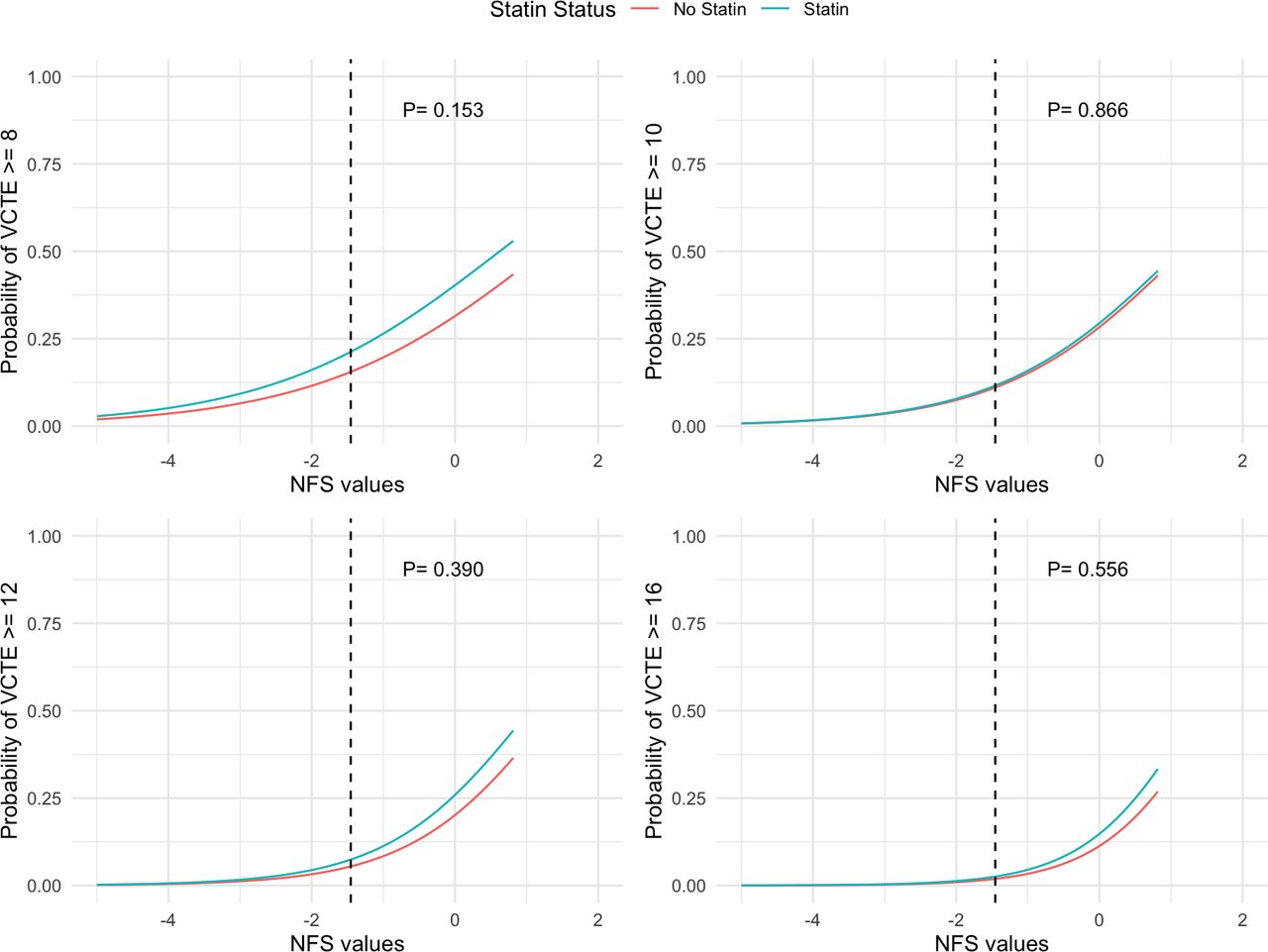
The effect of statins on NFS-based prediction of VCTE was distinct from the effect of FIB-4 and Hepamet predictions. Indeed, statins did not alter the association between NFS and VCTE even at a low VCTE threshold (8 kPa) (figure 4). However, NFS classified a smaller proportion of patients as low risk (83% on statins and 49% not on statins) than FIB-4 and Hepamet, while the NPVs were comparable to those of FIB-4 and Hepamet.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effect of statins on NFS-based prediction of different clinically relevant VCTE thresholds (8, 10, 12 and 16 kPa). Statin use did not affect NFS predictions of VCTE at any thresholds. The dashed line represents the threshold −1.455. NFS, NAFLD Fibrosis Score; VCTE, vibration controlled transient elastography.
Discussion
In this study, we assessed the potential impact of statin treatment on an NAFLD referral pathway to triage NAFLD patients who need a hepatology referral. We specifically tested the potential modifying effect on statins on three NITs: FIB-4, Hepamet and NFS. In our study, patients who were taking a statin had a higher probability of having VCTE >8 for a given value of FIB-4 (though this difference was less marked when using higher VCTE thresholds to define advanced liver fibrosis). We show here that this was mainly related to the higher baseline risk (and hence, pretest probability) of liver fibrosis in patients taking statins. Patients on a statin were older, more frequently had diabetes and had a higher BMI. Second, the effect of statins on the association between Hepamet and VCTE was similar to FIB-4, while it was much less marked for NFS. Overall, statin treatment had a negligible impact on NPVs of these NITs, and therefore, do not question the value of these NITs as a first step in the referral pathway. Finally, we show that more than half of patients with a clinical indication for a statin were not on a statin at the time of referral.
According to the Canadian Cardiovascular Society, statins are indicated for any patient over the age of 40 with diabetes, which explains why most of our patients with an indication for a statin had more frequently diabetes and were older.17 Our adjusted models show that the higher probability of VCTE >8 kPa for any FIB-4 value could be mostly explained by the difference in baseline characteristics rather than the effects of the statin itself. When we assessed the effects of statins on FIB-4-based prediction of VCTE in patients with an indication for statins, the prediction difference was not significantly different between those with an indication for a statin and were taking a stain compared with those with an indication for a statin that were not taking a statin. The above analysis provided further supportive evidence that statin treatment itself has a minimal impact on FIB-4 prediction of liver fibrosis, acknowledging the limitation that in this study fibrosis was indirectly assessed by VCTE and not by liver biopsy.
Statins effect on Hepamet-based predictions was comparable to that of FIB-4-based predictions, whereas NFS predictions were minimally altered. This can be explained by the fact that neither Hepamet nor FIB-4 include BMI in their calculation, while this is included in NFS. We have shown before and show again here that BMI has a pronounced effect on NITs based prediction of advanced fibrosis25 (online supplemental material 3). Since BMI was different in patients with and without statins, this differential effect between the three NITs is not unexpected. However, in all three NITs, the effect of statins markedly attenuated for higher thresholds of VCTE (10, 12 and 16 kPa). These higher thresholds are probably more in keeping with current trends in the stratification of patients with NAFLD, since the rate of liver related events is negligible in patients with VCTE <10 or 12 kPa.35 36 Furthermore, recent guidelines for HCC screening in patients with NAFLD suggest a VCTE measurement of 16.1 kPa as the threshold for initiating screening.31
Previous studies have shown that statins were under prescribed in patients with NAFLD, with 44%–74% of patients with indication for a statin not receiving a statin.37–39 Several explanations might account for this. The most important one could be that PCPs may be concerned about statin liver toxicity in NAFLD patients with baseline serum aminotransferases elevation.40 Another explanation could be that, at the time of referral, PCPs could be awaiting hepatologist assessment to decide if statins are contraindicated. In our study, some patients may have been misclassified as having an indication for a statin. Indeed, in a subset of the patients, our definition of statin indication was based on thorough modelling with the data that was available to us (online supplemental material 1), though we show that the impact of this modelling on the calculation of statin indication was minimal. We did not explore the reasons for non-prescription of statins which is a limitation of the study. Moreover, no information about any previous therapy with statins or any potential adverse reactions resulting in statin discontinuation was collected. Finally, the indication of statin in our study was based on the Canadian Cardiovascular Society which has some differences from the American Heart Association guidelines and the European guidelines (that would have resulted in higher numbers of statin indication, and therefore, higher rates of underprescription).24 41
In conclusion, we have found that statin treatment had only a minor effect on the ability of NITs (FIB-4, Hepamet and NFS) to predict advanced liver fibrosis. This effect was relevant only when a low threshold of VCTE (8 kPa) was used to classify patients with advanced fibrosis, but not with higher thresholds of 10, 12 or 16 kPa. Our data demonstrate that performance of FIB-4, Hepamet and NFS as a first step in a referral pathway for NAFLD is not significantly affected by statin use. Furthermore, only half of the patients referred through the pathway with an indication for a statin were taking a statin, which calls for a further understanding of the factors determining this finding and strategies to optimise cardiovascular prevention, which is still the main cause of morbidity and mortality in NAFLD.
Data availability statement
Data may be obtained from a third party and are not publicly available. These data are gathered from Alberta Health services (AHS) sources and our current agreement with Alberta Health services does not allow us to share them without an agreement approved by AHS.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by University of Alberta Research Ethics Boards(number Pro00076407). The study was completed as part of a larger quality improvement project that was approved by the University of Alberta Research Ethics Boards.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
TD, MM and JGA are joint senior authors.
TD, MM and JGA contributed equally.
Contributors MA-K: planning the study, collecting and interpreting data, data analysis and drafting the final manuscript. SF and MM: planning the study, interpreting data, drafting the final manuscript and study supervision. TD: planning the study, collecting and interpreting data, drafting the final manuscript and study supervision. JGA: planning the study, interpreting data, data analysis, drafting the final manuscript and study supervision. JGA: is the guarantor of the study
Funding This project was funded in part by an unrestricted grant by Gilead Sciences. Gilead Sciences had no part in the design, analysis, interpretation of the data or in drafting the manuscript. Award/ grant number: IN-CA-989-5661.
Competing interests JGA: Grants/Research Support: Gilead; Speakers Bureau/Honoraria: Lupin; Consulting Fees: Gilead, Genfit, Intercept, Inventiva, Boehringer-Ingelheim. MM: Advisory Board: Abbvie, Gilead, Merck, Novartis, Pfizer, Eisai; Funding (Grants): Gilead Science; Research/Clinical Trials: Abbvie, Gilead, Siliagen, Transgene, Pfizer, Exelixis, GSK. MA, SF, TD declare no conflict of interest.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.