Article Text

Abstract
Background and aims Digestive endoscopy is considered a high-risk procedure for COVID-19. Recommendations have been made for its practice during the pandemic. This study was conducted to determine adherence to recommendations for endoscopy practice during the COVID-19 pandemic in Latin America (LA).
Methods A survey was conducted of endoscopists from LA consisting of 43 questions for the evaluation of four items: general and sociodemographic features, and preprocedure, intraprocedure and postprocedure aspects.
Results A response was obtained from 338 endoscopists (response rate 34.5%) across 15 countries in LA. In preprocedure aspects (hand washing, use of face masks for patients, respiratory triage area, training for the placement/removal of personal protective equipment (PPE) and availability of specific area for the placement/removal of PPE), there was adherence in <75%. Regarding postprocedure aspects, 77% (261/338) had reused PPE, mainly the N95 respirator or higher, and this was with a standardised decontamination procedure only in 32% (108/338) of the time. Postprocedure room decontamination was carried out by 47% on >75% of occasions. In relationship to intraprocedure aspects (knowledge of risk and type of endoscopic procedures, use of PPE, airway management in patients and infrastructure), there was adherence in >75% for all the parameters and 78% of endoscopists only performed emergencies or time-sensitive procedures.
Conclusions Adherence to the recommendations for endoscopy practice during the COVID-19 pandemic is adequate in the intraprocedure aspect. However, it is deficient in the preprocedure and postprocedure aspects.
- endoscopy
- general practice
- gastrointestinal endoscopy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known about this subject?
Different associations around the world have made recommendations for gastrointestinal endoscopy practice during the COVID-19 pandemic to protect patients and healthcare providers during the pandemic.
What are the new findings?
Adherence to the recommendations for endoscopy practice during the COVID-19 pandemic in Latin America is adequate in the intraprocedure aspect. However, it is deficient in the preprocedure and postprocedure aspects.
How might it impact on clinical practice in the foreseeable future?
Given the fact that pandemic is still active in Latin America, endoscopists need to be more actively involved in monitoring and enforcing preprocedure and postprocedure recommendations.
Introduction
On 30th January 2020, the WHO declared a Public Health Emergency of International Importance due to the outbreak of a new coronavirus originating in the province of Hubei, China.1 The virus was later named SARS-CoV-2.2 The resulting disease is called COVID-19.3 SARS-CoV-2 enters and replicates by binding to ACE type 2 (ACE2) receptor. ACE2 receptor is abundant in the alveolar epithelium but it is also present in epithelial cells of the digestive tract.4 Viral fragments have been found in the stools of infected individuals raising concern about a digestive infection route.5 Therefore, SARS-CoV-2 is potentially transmissible during endoscopy because endoscopic procedures generate aerosols and microdroplets with a possibility of infection via the faecal–oral route.6 7
Healthcare workers (HCWs) have an increased risk of COVID-19.8 In Mexico, it is estimated that 20% of confirmed cases of COVID-19 are HCWs.9 Doctors make up 32% of those affected.10
Different associations around the world have made recommendations for gastrointestinal endoscopy practice during the COVID-19 pandemic aimed to protect patients and HCWs during the pandemic.11–15 These recommendations begin with risk stratification of patients by searching for signs or symptoms of COVID-19 prior to endoscopic procedures followed by the implementation of preventive measures for HCWs, training in wearing and removing personal protective equipment (PPE), the use and possible reuse of PPE, cleaning of endoscopic facilities and tracing patients after the procedure.16
However, the level of adherence to these recommendations by endoscopist doctors in Latin America (LA) is not known. Information related to the practice of endoscopy during the COVID-19 pandemic is important to take focused action and improve endoscopy practice. The objective of this study was to determine adherence to recommendations for endoscopy practice during the COVID-19 pandemic in LA.
Methods
A prospective survey directed towards endoscopists in LA was performed. A questionnaire in Spanish comprising 43 questions was designed using an electronic application (SurveyMonkey, Palo Alto, California, USA) to investigate issues related to adherence to recommendations for endoscopy practice during the COVID-19 pandemic, based mainly on the European Society for Gastrointestinal Endoscopy and the European Society of Gastroenterology and Endoscopy Nurses and Associates recommendations covering four main areas: 17 questions on general aspects (sociodemographic, work sector, information medium and current situation of the workplace), 9 questions on preprocedure (assessment of the patient and previous training received), 11 questions on intraprocedure (knowledge of risk and type of endoscopic procedures, use of PPE, airway management in patients and infrastructure), and 6 questions on postprocedure (telephone follow-up of the patient, PPE reutilisation and disinfection of the endoscopy room). We defined adequate adherence when the aspect evaluated was followed >75% of the time. No personal or sensitive data from the respondents were included, and responses were completely anonymous.
A pilot study (validation) was conducted by invitation addressed to 30 endoscopist members of the Mexican Association of Gastrointestinal Endoscopy (AMEG) to determine the correct understanding of questions and deficiencies in response options. The final questionnaire format was sent to all members of AMEG and the Inter-American Society for Digestive Endoscopy (SIED) using email. The duration of the survey was less than 10 min and it could only be answered once. For the survey in Brazil, the final questionnaire was translated and subsequently revised by a Brazilian doctor for the correct understanding in Portuguese. In this case, the questionnaire was sent through an electronic messaging service using the researcher’s endoscopist contacts. The survey remained open for 14 days for the questionnaire in Spanish (7–21 May 2020) and in Portuguese (16–30 June 2020).
A database was created using Excel and analysis was performed using SPSS V.24. Sample size calculation was performed using Epi info. Knowing that the total AMEG population of endoscopists by 2020 is 784, 258 participants were required for the survey to be representative, expecting a confidence level of 95%. The exact number of SIED members is not known since it does not count members individually, but through membership of the different LA societies. Therefore, it does not have a database of all members, only members of the director’s boards of each society. The survey was sent to those members. In the case of Brazil, the survey invitation was made through the contacts of local authors participating in this project.
Descriptive statistics were performed using means, medians and frequencies according to the type of variable with the χ2 test and multiple logistic regression for the analysis of categorical variables considering statistically significant differences with a p value of less than 0.05. All analyses were performed using the program SPSS V.20.
Results
General features
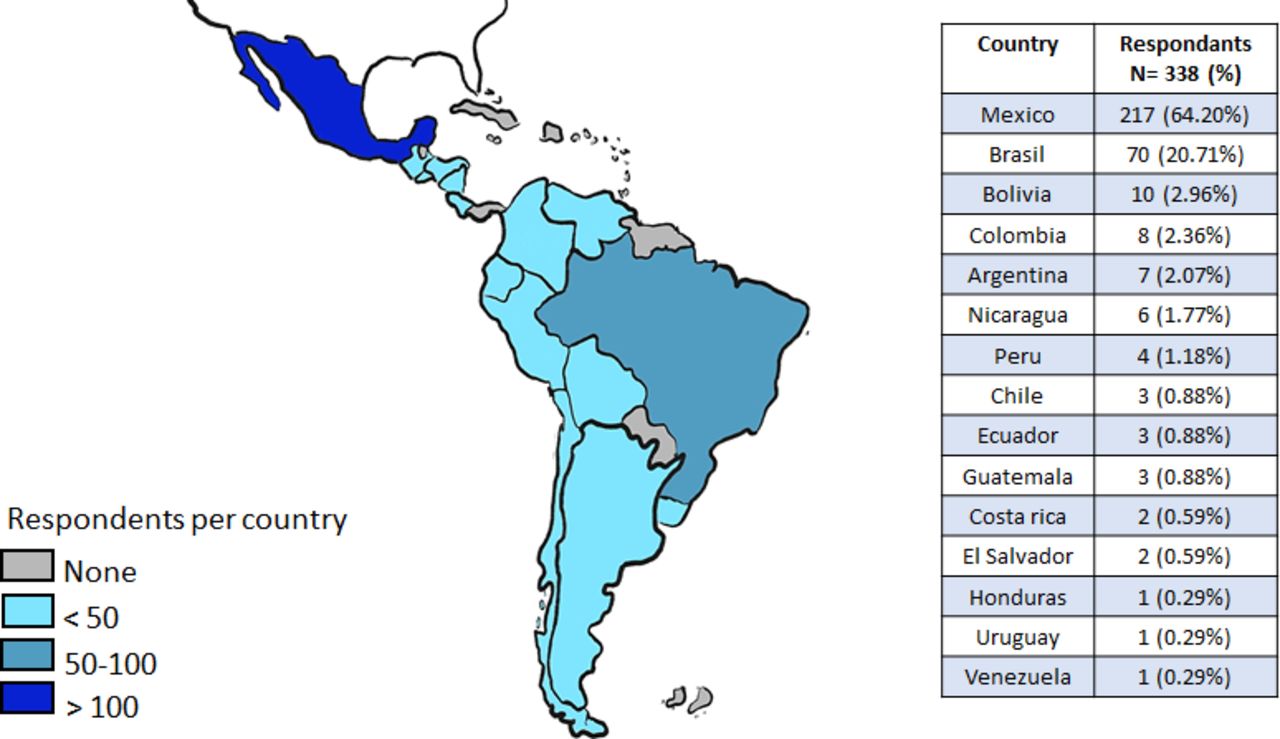
The time taken to answer the survey was in average 9 min. The survey was sent to 784 members of the AMEG, 92 members of the director’s boards of SIED, and 102 endoscopists from Brazil. A response was obtained from 338 endoscopists (response rate 34.5%) from 15 countries in LA (figure 1). Demographic characteristics of the participants are shown in table 1. Thirty-three per cent (114/338) reported suffering from a disease associated to a risk of serious evolution of COVID-19.

Geographical distribution of participating endoscopists.
General characteristics of participating endoscopists
Seventy-one per cent (239/338) received a written plan for patient care and operation of the endoscopy unit during the coronavirus pandemic. Work teams had been set up to avoid simultaneous contagion in 10.6% (36/338). There were hospitalised patients with COVID-19 in 71% (239/338) of endoscopist workplaces. At the time of the survey, changes in the schedule of endoscopic procedures since the beginning of COVID-19 pandemic had been in place for more than 8 weeks in the case of 41% (140/338) of endoscopists, between 4 and 8 weeks for 38% (129/3338), between 2 and 4 weeks for 17% (56/338) and less than 2 weeks for only 4% (13/338). Seventy-four per cent (165/223) of endoscopists who had seen patients with a high suspicion of or confirmed COVID-19 considered that they adhere to current recommendations >75% of the time. At the time of the survey, 1.8% (6/338) of endoscopists had been infected with COVID-19.
Information about recommendations for endoscopy practice during the COVID-19 pandemic was most frequently obtained from scientific journals (81%, 246/338), followed by webinars/online sessions (73%, 246/338), the internet (49%, 164/338) and newspapers/television (6%, 19/338).
Preprocedure aspects
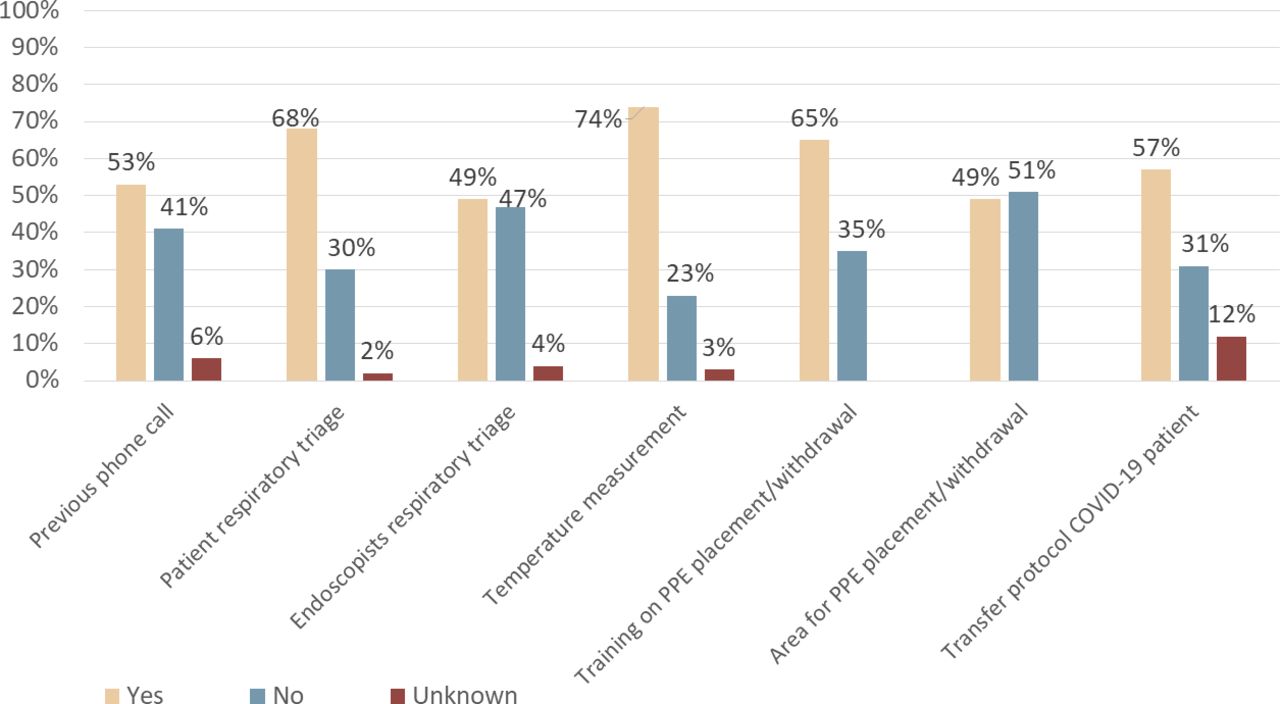
None of the items of this area had adequate adherence (figure 2).
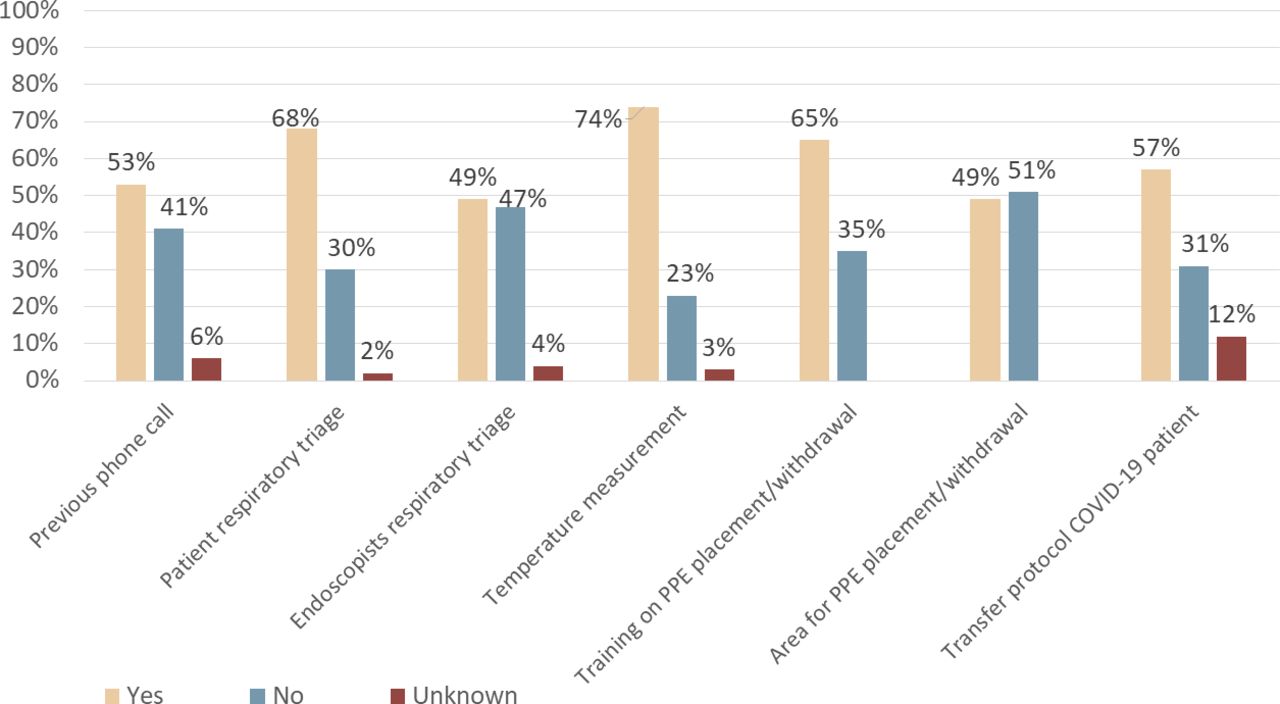
Adherence to preprocedure recommendations. PPE, personal protective equipment.
For outpatient care, 41% (139/338) reported that the patients were invited to perform hand washing >75% of the time, 19% reported <25% of the time (64/338), 13% (44/338) reported between 25% and 75% of the time and 27% (91/338) did not know. Fifty-three per cent (179/338) of the respondents provided surgical masks to patients >75% of the time, 34% (115/338) to <25% of the time and 13% (44/338) between 25% and 75% of the time.
Intraprocedure aspects
Regarding the type of endoscopic procedures during the pandemic, 78% (262/338) reported that they had exclusively performed emergencies or time-sensitive procedures.
Seventy-five per cent (254/338) considered all endoscopic procedures (gastroscopy, duodenoscopy and colonoscopy) to have a risk of aerosol generation, while 17% (59/338) did not consider colonoscopy to have risk of aerosol generation.
Eighty-three per cent (281/338) of endoscopists who undertook an endoscopic procedure in the last 4 weeks had used full PPE. Components of the PPE were provided entirely by the endoscopy centre 40% (139/338) of the time. The most frequent PPE components that were not provided were: goggles (65%, 130/199), an N95 respirator or higher (46%, 92/199), and face shields (39%, 77/199). The use of different PPE components in the care of patients with a high suspicion or confirmed diagnosis of COVID-19 is shown in figure 3.

PPE used during endoscopic procedures for patients with a high suspicion or confirmed COVID-19 diagnosis. PPE, personal protective equipment.
For airway management during endoscopic procedures in patients with a high suspicion or confirmed COVID-19, 55% (186/338) of endoscopists individualised each case, 21% (70/338) would prefer to do it with the patient intubated, 20% (68/338) not intubated and 4% (14/338) considered intubation contraindicated in this scenario.
Eleven per cent (37/338) had a negative-pressure room available for performing endoscopy in patients with confirmed COVID-19.
Postprocedure aspects
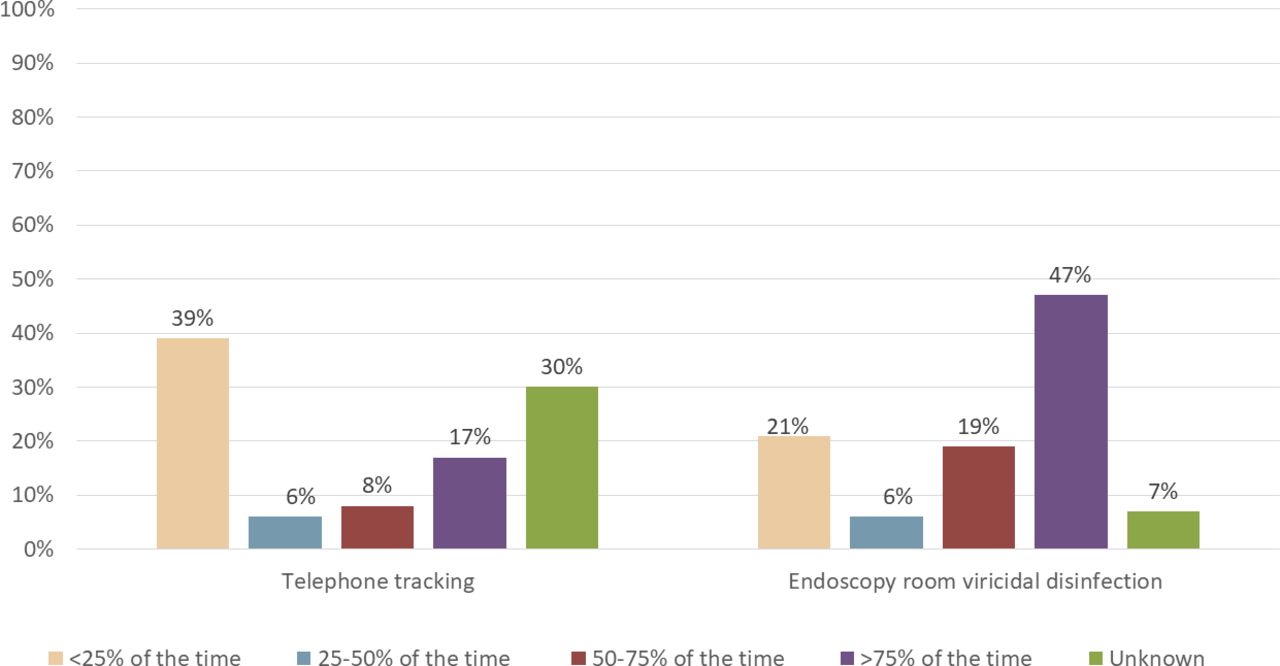
Figure 4 shows the rate of postprocedure telephone monitoring and disinfection of the endoscopy room. Up to a quarter of the time, none of these measures were carried out in the centres. Seventy-seven per cent (261/338) had reused PPE. The three most frequently reused components were: the N95 respirator or higher (78%, 194/261), goggles (67%, 67/261) and face shields (66%, 174/261). Those endoscopists who had reused a N95 respirator or higher did this with a standardised decontamination procedure 32% (108/338) of the time. The decontamination procedures used for the reutilisation of an N95 respirator or higher were: not using it for more than 72 hours (61%, 139/229), ultraviolet light (9%, 20/229), oven heat greater than 70°C (5%, 12/229) and vaporised hydrogen peroxide (4%, 9/229). Eight per cent (19/229) did not know the procedure used for decontamination and 21% (52/229) reused it without any standardised decontamination procedure.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Telephone tracking and postprocedure room disinfection.
We analysed possible differences in the adherence of all recommendations between private and public practice. In univariate analysis, a difference was observed in favour of the private sector in the following aspects: prior telephone evaluation of the patient (69.6% (87/125) vs 43.7% (93/213); p<0.001), patient hand washing >75% of occasions (53.6% (67/125) vs 32.9% (70/213); p<0.001), patient surgical mask supply >75% of occasions (63.2% (78/125) vs 47.4% (101/213; p=0.005), complete PPE (89.6% (112/125) vs 79.3% (169/213); p=0.015), N95 respirator reutilisation using a standardised decontamination method (39.2% (49/125) vs 27.7% (59/213); p=0.029), postprocedure telephone tracking >75% of the time (34.7% (23/213) vs 26.4% (29/125); p<0.001) and postprocedure endoscopy room disinfection >75% of the time (62.4% (78/125) vs 38% (81/213); p<0.001). The only aspect that favoured the public sector was training for PPE placement/removal (69% (147/213) vs 58.4% (73/125); p=0.048). Multivariate analysis is shown in table 2.
Multivariate analysis* of adherence to recommendations by endoscopists classified by type of practice (private vs public practice)
Discussion
According to our data, adherence to the recommendations for endoscopy practice during the COVID-19 pandemic in LA is adequate regarding intraprocedure aspects but is deficient in the preprocedure and postprocedure aspects.
Fever, cough, fatigue, and dyspnoea are reported symptoms that occur frequently in patients with COVID-19 (68%, 49%, 20%, and 20%, respectively).17 Respiratory triage for patients is a simple strategy that can be helpful. A prior telephone evaluation can detect these symptoms and prevent a suspected patient with COVID-19 from transferring to the endoscopy unit, thus avoiding the risk of contagion. Mathematical models have estimated that a symptom-based screening strategy may fail to detect more than 50% of COVID-19 cases.18 However, given the fact that it is a simple and cheap strategy, we believe that it should be used frequently. In our study, telephone assessment the day before the procedure was performed in only 53% of cases, maybe it can be related to availability of personnel to do it.
The greater contagiousness of SARS-CoV-2 is caused by a high viral load even in the presymptomatic phase.19 In addition, SARS-CoV-2 can be transmitted via faecal–oral routes, which means that even colonoscopy can transmit the virus if it is present in the stool. Faecal clearance of SARS-CoV-2 in convalescent patients is slower compared with nasopharyngeal clearance.20 Therefore, full PPE should be used for any endoscopic procedure. PPE training is a universal recommendation in which all associations from different continents agree and has been promoted by the World Organization of Gastroenterology even in low-resource settings.21 We observed that even though 79% of endoscopists had seen changes to endoscopic procedures schedule more than 4 weeks ago because of COVID-19, only 65% reported specific PPE training. It is worrying that only 49% had a specific assigned area for the placement/removal of PPE. This represents a higher risk of infection. Greater and constant training is required, as well as the adaptation of endoscopy areas for safer working environments. Gastrointestinal endoscopy is considered a high-risk procedure because of the generation of aerosols. Complete PPE use was frequently reported by the participants in our study (83%). A recent North American survey showed similar rates of PPE utilisation for endoscopic procedures (86%).22 An international survey (which did not include LA) showed a high rate of use of PPE (>90%) during endoscopic procedures.23
At the time of the study, 1.8% of endoscopists reported being infected with COVID-19. That rate is low if we take into account that up to 20% of the confirmed cases of COVID-19 in some LA countries have occurred in HCWs.7 The rate of COVID-19 infection between endoscopists reported in a survey study done in Brazil alone was similar (1.7%).24 In Italy, a study of HCWs carried out in the active phase of the pandemic, showed that 4.3% of HCWs had COVID-19. Most of the cases (85.7%) occurred before adopting generalised security measures (use of PPE, selection of cases of digestive endoscopy).25 This suggests that the selection of endoscopy cases and the use of PPE are effective measures and explains the low frequency of COVID-19 infection observed in our survey.
Factors related to COVID-19 in HCWs are not entirely known. A cohort study showed that the risk of having a positive test for COVID-19 is 46% higher when PPE is reused and 33% higher when inadequate PPE is used.6 These findings are a serious concern because 72.1% of respondents in our study reported PPE reutilisation, which is even higher than developing countries in other regions of the world. A survey conducted in Africa reported a PPE reuse rate of 43%.26
Although certain PPE components were originally designed for single use (eg, N95 respirator or higher), a shortage of resources has forced its reutilisation. Methods that have been shown to be effective in decontaminating a high-efficiency respirator without affecting its filtering capacity are ultraviolet light, vaporised hydrogen peroxide and dry heat.27 Unfortunately, the previously mentioned methods accounted for only 18% of the respondents regarding alternative reuse strategies. The non-use of N95 respirator for 72 hours was a common reuse strategy in our study (62%). The theoretical fundament is based on a recent report that communicated virus viability on different inert surfaces, including stainless steel and plastic, to be up to 72 hours.28 However, this strategy has not been specifically studied in high-efficiency respirators. If we consider the previously mentioned virus viability on inert surfaces, disinfection with a viricidal agent should be a frequent practice after an endoscopic procedure. Despite this, we observed that only 47% reported disinfecting the room with a viricidal agent more than 75% of the times after an endoscopic procedure.
Telephone tracking is a postprocedure recommendation that was infrequently done in our study (figure 4). A European survey reported that contact for patients after 7–14 days from endoscopy to inquire about COVID-19 symptoms was done only 28.3% of the time.29
According to our data, adherence to recommendations for endoscopic procedures during the COVID-19 LA pandemic is adequate in the intraprocedure aspect (figure 2). This is probably explained because intraprocedure aspect depends largely on the endoscopist. Deficiencies in the preprocedure and postprocedure aspects could be due to the institute/hospital/clinic policy and not purely due to ancillary staff. Here, we decided to evaluate if there were differences between public versus private practice, based on that in LA, there is a general idea that the availability of resources is better in private practice. Differences in adherence to recommendations by endoscopists from the private sector compared with those in the public sector are mainly in the preprocedure and postprocedure aspects and may be related to fewer personnel in the public sector because these processes usually require more human resources for implementation and supervision (table 2). Given the fact that pandemic is still active in LA, endoscopists need to be more actively involved in monitoring and enforcing preprocedure and postprocedure recommendations.
Our study has limitations. First, the number of participants was less than calculated sample (in Mexico) and most of participants were from Mexico and Brazil. Second, other personnel who participate in endoscopic procedures, such as nurses, fellows, and anaesthesiologists were not included in the survey, so our findings cannot be generalised to all personnel. Finally, respondents were aware of the intent of the study, which might have led to bias in their answers. However, to the best of our knowledge, this is the first and largest survey conducted that includes endoscopists from several LA countries.
In conclusion, adherence to intraprocedure recommendations for endoscopy practice in LA during the COVID-19 pandemic is adequate, but it is deficient in the preprocedure and postprocedure aspects.
Supplemental material
Acknowledgments
To the Mexican Association of Gastrointestinal Endoscopy and Inter-American Society of Digestive Endoscopy staff for their help on the distribution of this survey.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors EM-P—conceptualisation, methodology, investigation, formal analysis, writing (original draft), and visualisation. FT-A—conceptualisation, methodology, formal analysis, writing (original draft), supervision, and project administration. RAZ-M—investigation, resources, and visualisation. OA-N—investigation and writing (review and editing). GB-V—writing (review and editing). OMS-P—writing (review and editing). OVH-M—writing (review and editing). GA-DP—resources and writing (review and editing). JAT—resources and writing (review and editing).
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient consent for publication Not required.
Data availability statement Data are available in a public, open access repository. Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplemental information.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.