Article Text

Abstract
Background Non-alcoholic steatohepatitis (NASH) is a severe state of non-alcoholic fatty liver disease (NAFLD), which is pathologically characterised by steatosis, hepatocyte ballooning, and lobular inflammation. Host–microbial interaction has gained attention as one of the risk factors for NASH. Recently, cnm-gene positive Streptococcus mutans expressing cell surface collagen-binding protein, Cnm (cnm-positive S. mutans), was shown to aggravate NASH in model mice. Here, we assessed the detection rate of cnm-positive S. mutans in oral samples from patients with NASH among NAFLD.
Methods This single hospital cohort study included 41 patients with NAFLD. NASH was diagnosed histologically or by clinical score. The prevalence of cnm-positive S. mutans, oral hygiene and blood tests, including liver enzymes, adipocytokines and inflammatory and fibrosis markers, were assessed in biopsy-proven or clinically suspected NASH among NAFLD.
Results Prevalence of cnm-positive S. mutans was significantly higher in patients with NASH than patients without NASH (OR 3.8; 95% CI 1.02 to 15.5). The cnm-positive S. mutans was related to decreased numbers of naturally remaining teeth and increased type IV collagen 7S level (median (IQR) 10.0 (5.0–17.5) vs 20.0 (5.0–25.0), p=0.06; 5.1 (4.0–7.9) vs 4.4 (3.7–5.3), p=0.13, respectively).
Conclusions Prevalence of cnm-positive S. mutans in the oral cavity could be related to fibrosis of NASH among NAFLD.
- nonalcoholic steatohepatitis
- infectious disease
- bacterial infection
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known about this subject?
Multiple parallel hits hypothesis is widely accepted for the pathogenesis of non-alcoholic steatohepatitis (NASH).
The association of oral microbiota with NASH is poorly investigated.
What are the new findings?
The prevalence of cnm-positive Streptococcus mutans in the oral cavity was associated with NASH.
The prevalence of cnm-positive S. mutans in the oral cavity was associated with poor oral hygiene.
How might it impact on clinical practice in the foreseeable future?
Future research is needed to explore the potential role of oral probiotics as a potential therapeutic target of NASH.
Introduction
Non-alcoholic fatty liver disease (NAFLD) is a common cause of chronic liver disease and a major indicator of metabolic syndrome that is becoming increasingly prevalent worldwide.1 2 Non-alcoholic steatohepatitis (NASH), which is encapsulated within NAFLD, is an aggressive state that is pathologically defined by the presence of steatosis, hepatocyte ballooning and lobular inflammation,3 ultimately leading to cirrhosis, hepatocellular carcinoma and even a variety of cardiovascular diseases.4 5 As underlying mechanisms of NASH, the ‘multiple parallel hits’ hypothesis is widely accepted, which claims that fatty liver is the first stage leading to NASH, followed by parallel hits derived from various factors including microbiota, adipose tissue, and genetic factors.6 Focusing on the specific strain Streptococcus mutans, which is one of the major causative pathogens of dental caries, we suggested the role of this bacterium in development of systemic diseases including inflammatory bowel disease,7 immunoglobulin A nephropathy,8 and intracerebral haemorrhage.9 10 Moreover, we identified the contribution of cnm gene-positive S. mutans expressing the collagen-binding protein, Cnm, on the cell surface (cnm-positive S. mutans), to the aggravation of NASH in obesity model mice.11 12 However, in humans, the relationship between NASH and oral hygiene, with a focus on cnm-positive S. mutans infection, remains unknown. Herein, we aimed to study the association between cnm-positive S. mutans and NASH.
Subjects and methods
Study subjects
In a single hospital-based, cross-sectional observational study, we collected outpatients who had been diagnosed with fatty liver disease using medical record within 5 years in Nara City Hospital from April 2017 to January 2018. Subjects who fulfilled eligibility criteria were collected and registered after obtaining written informed consent. All participants underwent physical examinations, blood tests, abdominal ultrasound, and questionnaires. Of all participants, subjects who had other causes of liver diseases (viral, autoimmune), consumed excessive amounts of alcohol (alcohol >30 g/day in men and 20 g/day in women),13 had no findings of fatty liver including hepatorenal echo contrast, bright liver, deep attenuation, or vascular blurring at the baseline assessment,14 withdrew informed consent, could not undergo oral sampling were excluded. This study was carried out in accordance with the Japanese Ethical Guidelines for Medical and Health Research Involving Human Subjects (Public Notice of the Ministry of Health, Labor and Welfare No.475 of 2014). All subjects gave written informed consent in accordance with the Declaration of Helsinki.
NAFLD and NASH diagnosis
Diagnosis of NAFLD is based on the following criteria: (1) hepatic steatosis on imaging or histology, (2) no other cause of liver diseases (viral, autoimmune) and no significant alcohol consumption (alcohol >30 g/day in men and 20 g/day in women),13 and (3) no competing causes for hepatic steatosis. Liver biopsy remains the only reliable method to identify the severity of conditions that encapsulate NAFLD (ie, a condition that encompasses simple steatosis, NASH, and cirrhosis). For 16 subjects who underwent liver biopsy within 5 years, we referred to the pathological diagnosis of NASH following the NAFLD activity score.15 For subjects who did not undergo liver biopsy, conventional ultrasound was used to evaluate fatty liver clinical setting16 17 using Aplio 500 (Canon Medical Systems Co, Tochigi, Japan) and possible NASH was diagnosed using the NASH, ferritin, insulin, type Ⅳ collagen (NAFIC) score using ferritin, fasting insulin and type IV collagen 7S. In a previous cohort study, the sensitivity, specificity, positive predictive value, negative predictive value of NAFIC score ≥2 for NASH diagnosis were 60, 89, 85, and 64%, respectively.18
Risk factors and covariate assessments
Risk factors and covariates were evaluated using physical examination, blood tests, and self-reported questionnaires after receiving written informed consent. Body mass index (BMI) was defined as weight (in kg) divided by the square of height (in m). Obesity was defined as BMI ≥25 kg/m2.19 Sitting blood pressure was measured at 5 min intervals and the mean was used for analysis. Subjects were considered to have hypertension if they were taking antihypertensive medications, self-reported diagnosis of hypertension, or systolic blood pressure of ≥140 mmHg or diastolic pressure of ≥90 mmHg. Diabetes mellitus was defined as a fasting blood glucose level of ≥126 mg/dL or treatment with insulin or hypoglycaemic agents. For further assessments, insulin sensitivity and secretory ability were calculated using the fasting values of serum glucose and insulin according to homeostasis model assessment (HOMA) methods.20 Dyslipidaemia was defined as fasting plasma triglyceride level ≥150 mg/dL, low-density lipoprotein cholesterol levels ≥140 mg/dL, or treatment with statins or fibrates. Liver enzymes including aspartate aminotransferase and alanine aminotransferase; liver fibrosis markers including platelet count, ferritin, and type IV collagen 7S; inflammatory markers including interleukin-6 and hypersensitive C-reactive protein and adipocytokines including adiponectin and tumour necrosis factor-α (TNF-α) were evaluated. Subjects were defined as never, past, or current smoker according to self-reported cigarette smoking habitation. Daily alcohol consumption was assessed by the questionnaires and subjects were defined as alcohol drinkers if they drank >30 g/day in men and 20 g/day in women.13 Oral hygiene was evaluated by the self-reported number of naturally remaining teeth21 22 and past dental treatment.
Oral sample collection
We asked subjects to visit the hospital at least 9 hour from their last meal. Oral samples were collected after light gargling with water. Dental plaque and saliva specimens were collected from subjects using Seed Swab (EIKEN Chemical Co, Tokyo, Japan) and 50 mL Eppendorf Conical Tube (Eppendorf AG, Hamburg, Germany), respectively. Oral samples were transported to Okayama University Graduate School of Medicine, Dentistry, and Pharmaceutical Sciences and frozen at −20°C until analysis.
Bacterial strains and growth conditions
Oral samples were inoculated in Mitis-Salivalius (MS) agar plates (Difco Laboratories, Detroit, Michigan, USA) containing bacitracin (0.2 U/ml; Sigma-Aldrich Co, Sent Louis, Missouri, USA) and 15% sucrose (MSB plates), and then anaerobically incubated at 37°C for 48 hours. At least five colonies of S. mutans were isolated morphologically and cultured in brain heart infusion broth (Difco Laboratories) at 37°C for 24 hours.
DNA extraction and PCR method
S. mutans DNA was extracted using a previously described method.23 Briefly, bacterial cells were collected and incubated with 62.5 µL of lysozyme chloride from chicken egg white (2.0 mg/mL; Sigma-Aldrich Co) and 0.25 µL of lysozyme hydrochloride from chicken egg white (10 mg/mL; Wako Pure Chemical Industries, Osaka, Japan) for 90 min at 37°C. Genomic DNA was then extracted using 600 µL of Cell Lysis solution (Qiagen, Düsseldorf, Germany) and incubated at 80°C for 5 min, followed by addition of 3 µL of RNase A (10 mg/mL; Qiagen) to the mixture and incubation at 37°C for 30 min. In addition, 200 µL of protein precipitation solution (Qiagen) was added, vortexed vigorously for 20 min and then centrifuged at 10 000×g for 3 min. The supernatant was combined with 600 µL of isopropanol (Wako Pure Chemical Industries) and centrifuged. The precipitate was then resuspended with 70% ethanol (Wako Pure Chemical Industries), centrifuged at 10 000×g for 3 min, combined with 100 µL of DNA hydration solution (Qiagen) and stored as a DNA extract. Confirmation of S. mutans and presence of cnm gene was carried out by PCR using TaKaRa Ex Taq polymerase (TAKARA BIO, Shiga, Japan) with S. mutans-specific and cnm-specific primers,24 25 template DNA, and 1.5 mM of MgCl2, according to the supplier’s protocols. Amplification was performed using the following parameters. To detect S. mutans, 30 cycles of a denaturing step at 98°C for 10 s, and primer annealing and extension steps at 70°C for 1 min were performed. To detect the cnm gene, we performed initial denaturation at 95°C for 4 min, and then 30 cycles consisting of 95°C for 30 s, 60°C for 30 s and 72°C for 2 min, with a final extension at 72°C for 7 min. PCR products were subjected to electrophoresis in 1.5% or 0.7% agarose gel-Tris-acetate-EDTA buffer. The gel was stained with 0.5 µg of ethidium bromide per millilitre and photographed under ultraviolet illumination.
Statistical analyses
Continuous variables are presented as mean±SD, non-normal variables are reported as median and IQR, and categorical variables are described as numbers and frequencies (%). To compare continuous, non-normal and categorical variables among groups, we used analysis of variance, Wilcoxon signed-rank test and Pearson’s χ2 test, respectively. To identify independent risk factors for NASH, logistic regression model analyses were performed based on previously identified factors and factors for which an association was suggested in univariate analysis (p<0.25). ORs and 95% CIs were calculated for independent predictors of NASH. The statistical significance level was set at 0.05, additionally, the borderline significance level at 0.1 and the tendency at 0.2 for all analyses. All statistical analyses were conducted using JMP V.12.0 software (SAS Institute, Cary, North Carolina, USA).
Results
Subject characteristics
Among the 117 subjects who fulfilled the eligibility criteria, 56 participants gave us written informed consent to participate in this study and underwent physical examinations, blood tests, oral sample collection, abdominal ultrasound, and questionnaires. Of these subjects, one subject withdrew after providing informed consent, one subject could not undergo oral sampling, and two subjects with alcoholic hepatitis and 11 subjects with normal findings were excluded. As a result, 41 subjects were registered for this study. Table 1 shows the subject characteristics. There were 19 male subjects (46.3%). The mean age was 67.0±10.3 years. BMI was 26.4±3.8 kg/m2. Twenty-five subjects (61.0%) were classified as obese (BMI ≥25.0 kg/m2). Five subjects (12.2%) were current smokers and 11 26.8%) were past smokers. The median (IQR) of alcohol consumption was 0.0 (0.0–5.9) g/week. Hypertension, diabetes mellitus and dyslipidaemia were identified in 31 (71.6%), 11 (26.8%), and 15 (36.6%) subjects, respectively. In 16 subjects who underwent liver biopsy, 14 (87.5%) were diagnosed with NASH. Only five (20.0%) of the remaining 25 subjects who were clinically diagnosed with NAFLD fulfilled the criteria for possible NASH. S. mutans and cnm-positive S. mutans were detected in 34 (82.9%) and 15 (36.6%) subjects, respectively.
Subject’s characteristics
cnm-positive S. mutans and NASH
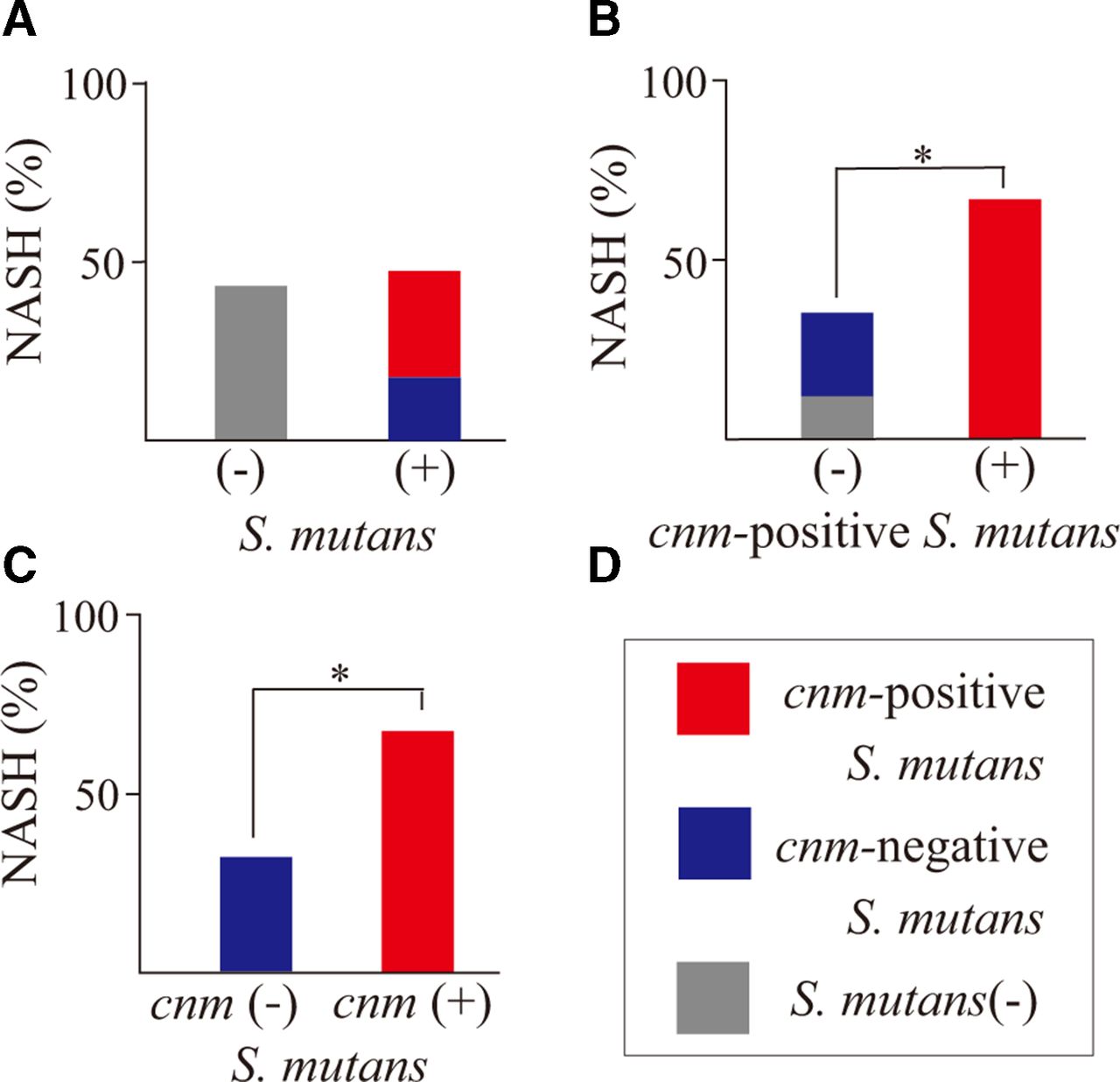
There was no significant difference in prevalence of NASH among NAFLD between the S. mutans-positive group (n=34) and S. mutans-negative group (n=7) (3 (42.9%) vs 16 (47.1%); p=0.84) (figure 1). However, the prevalence of NASH among NAFLD was significantly higher in subjects with cnm-positive S. mutans compared with those without (10 (66.7%) vs 9 (34.6%); p=0.05) (OR 3.77, 95% CI 1.02 to 15.5) (figure 1B) or those with cnm-negative S. mutans (10 (66.7%) vs 6 (31.6%); p=0.04) (OR 4.33, 95% CI 1.02 to 18.38) (figure 1C). In subjects with cnm-positive S. mutans, type IV collagen 7S levels tended to be higher (median (IQR) 5.1 (4.0–7.9) vs 4.4 (3.7–5.3); p=0.13) and adiponectin levels tended to be lower (6.7 (4.1–10.8) vs 9.2 (7.1–13.9); p=0.11) compared with those without (table 2).
Relationships between laboratory findings and cnm-positive Streptococcus mutans

Relationship between the presence of cnm-positive Streptococcus mutans in the oral cavity and NASH. There was a significant difference in the prevalence of NASH among patients with NAFLD between subjects with cnm-positive S. mutans and those without or with cnm-negative S. mutans. *P<0.05, as described by χ2 test. NAFLD, non-alcoholic fatty liver diseases; NASH, non-alcoholic steatohepatitis.
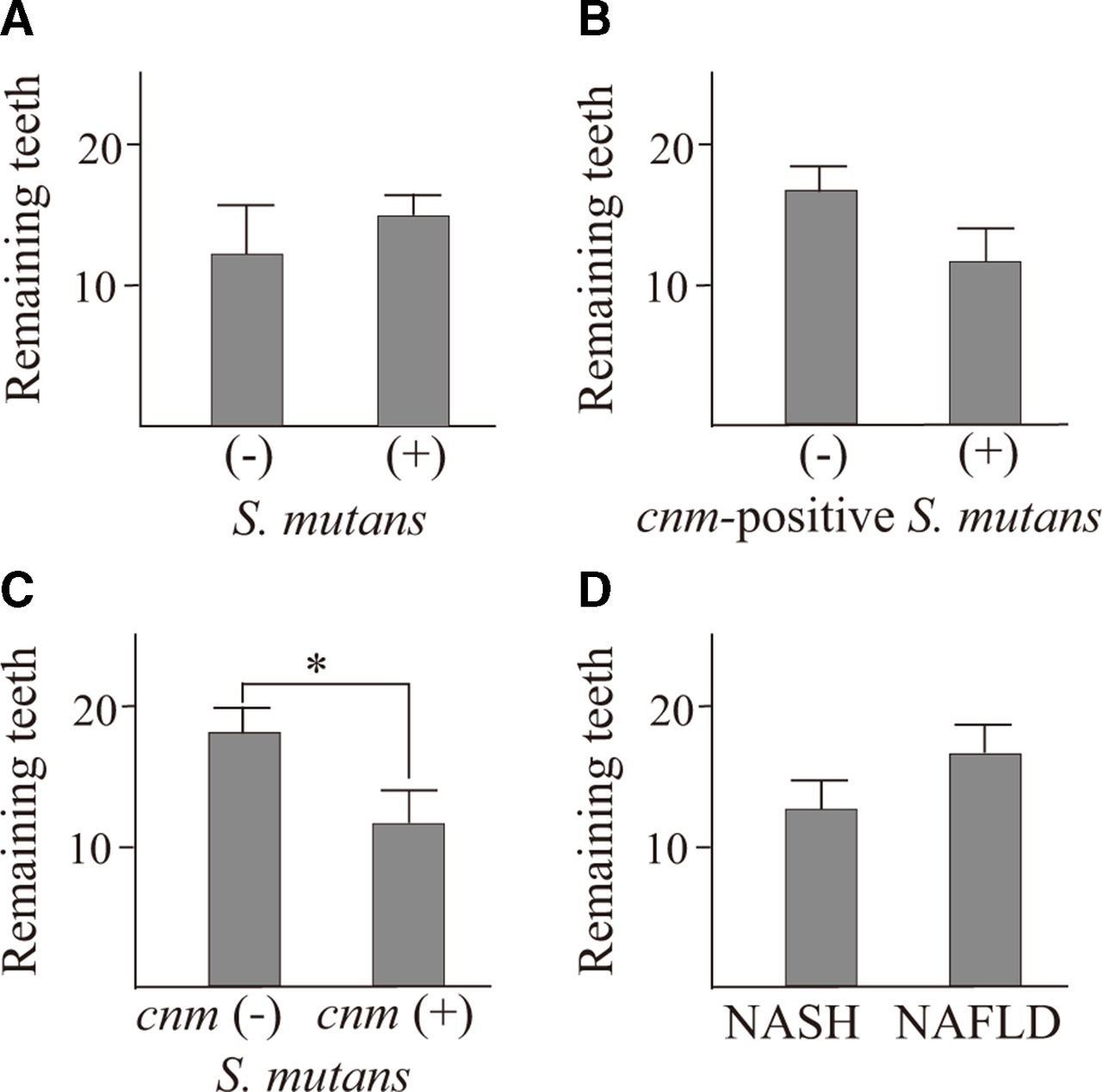
cnm-positive S. mutans and dental hygiene
Of 41 subjects, 36 answered the remaining number of teeth. Comparison of the S. mutans-positive group (n=30) with the S. mutans-negative group (n=6) revealed that there was no significant difference in the number of naturally remaining teeth (mean (SD): 14.8 (±8.0) vs 12.5 (±10.4); p=0.54) (figure 2A) However, in the cnm-positive S. mutans group (n=14), there was a borderline significant decreased number of naturally remaining teeth compared with those without (n=22) (11.4 (±6.3) vs 16.4 (±9.0); p=0.08) (figure 2B) and significantly decreased number of naturally remaining teeth compared with cnm-negative S. mutans group (n=16) (11.4 (±6.3) vs 17.8 (±8.4); p=0.03) (figure 2C). The number of naturally remaining teeth tended to be lower in subjects with NASH (n=17) compared with those with NAFLD (n=19) (12.4 (±9.0) vs 16.3 (±7.4); p=0.16) (figure 2D).
{kind=link}
{kind=link}
Number of naturally remaining teeth in subjects with cnm-positive Streptococcus mutans and those without. Subjects with cnm-positive S. mutans had fewer naturally remaining teeth compared with cnm-negative S. mutans. Data present the mean number of naturally remaining teeth±SE of the means. *P<0.05, as described by Student’s t-test. NAFLD, non-alcoholic fatty liver diseases; NASH, non-alcoholic steatohepatitis.
Logistic regression analysis with NASH as the independent variable
In univariate analysis, NASH was significantly associated with cnm-positive S. mutans and marginally related to the number of naturally remaining teeth and HOMA-β. In logistic regression analysis, only cnm-positive S. mutans was independently associated with NASH (OR (95% CI): 6.28 (1.29 to 40.8); p=0.02) (table 3).
Univariate and multivariate analyses of risk factors associated with NASH
Discussion
To our knowledge, we demonstrated, for the first time, the association between a specific strain of S. mutans, cnm-positive S. mutans, and NASH in human. The present study provided three essential findings to consider the aetiologies: (1) the possible pathway by which cnm-positive S. mutans acts on hepatic cells, (2) the association between the number of naturally remaining teeth and presence of cariogenic bacteria, and (3) biomarkers reflecting the role of cnm-positive S. mutans in the development of NASH.
Potential pathway through which cnm-positive S. mutans acts on the liver
Our study surprisingly showed a significantly higher detection rate of cnm-positive S. mutans in subjects with NASH among NAFLD. However, it remains unknown whether this finding is consistent with previous animal studies. In animal models, intravenous administration of cnm-positive S. mutans was shown to accumulate in the liver and aggregated NASH,11 12 while we detected cnm-positive S. mutans in oral cavities, not in the blood. To explain this contradiction, it is necessary to introduce the unique host–pathogen interaction in the periodontal crevice and evaluate the bacterial properties of S. mutans. The gingival crevice, which lines the inside of the gingiva, is a particularly vulnerable site of the oral barrier. At the base of the sulcus where the mucosa connects to the tooth, the epithelium tapers down to 3–5 layers of thickness and allows constant passage of neutrophils from the tissue into the oral cavity26 and microbes from the oral cavity into the tissue.27 In fact, not only tissue trauma induced by procedures such as tooth extraction, periodontal probing, or scaling but also poor oral hygiene or toothbrushes can cause transient bacteraemia in human.28 S. mutans, a facultative anaerobic Gram-positive coccus, can survive in the blood with higher oxygen partial pressure, while most periodontal pathogens are anaerobic. Furthermore, specific S. mutans strains can escape host immunity by inhibiting complement activation29 30 and can invade into human endothelial cells.31 Clinically, S. mutans is well known as one of the major pathogens for infective endocarditis32 and a recent study using real-time PCR detected S. mutans DNA in the oral cavities and atherosclerotic plaques, which implicate the direct interaction of S. mutans in systemic diseases through the bloodstream.33 Based on these findings, we considered the direct effect of cnm-positive S. mutans on hepatic cells via transient bacteraemia for the progressive state of NASH. However, further research is necessary to confirm this mechanism and alternative aetiologies must be considered, for example, chronic inflammation34 or dysbiosis of gut microbiome driven by oral microbes.35
Association between number of naturally remaining teeth and cariogenic bacteria
In this study, the number of naturally remaining teeth was significantly lower in subjects with cnm-positive S. mutans compared with those with cnm-negative S. mutans. The diagnostic validity of self-reported remaining number of teeth have been shown in multicohort studies.21 22 And many epidemiological studies have suggested an association between periodontal disease severity and decreased number of naturally remaining teeth in adults.36 37 Although there are few reports discussing the number of naturally remaining teeth and caries, especially focusing on S. mutans, high proportions of S. mutans were seen in supragingival plaques in patients with chronic periodontitis38 incorporates, recently, there is an increasing number of root caries cases in the elderly population due to exposed root surfaces.39 The correlation between S. mutans count in the oral cavity and naturally remaining teeth might be in line with these findings. Furthermore, Cnm has high affinity to the human extracellular matrix, especially type I and IV collagens. In the oral cavity, cnm-positive S. mutans should bind to dentin, which is contained under the enamel, and invade tooth roots, which are composed of type I collagen,40 or dental pulp, which is composed of extracellular matrix.41
Biomarkers reflecting the role of cnm-positive S. mutans in the development of NASH
Although NASH model mice injected with cnm-positive S. mutans showed increased TNF-α levels,11 there were no significant relationships between the oral pathogen and inflammatory biomarkers including hypersensitive C-reactive protein, interleukin-6 and TNF-α. Chronic inflammation associated with oral infectious diseases should be essential pathogenesis.42 As a limitation of this study, the duration between the diagnosis of NASH and oral or blood samplings varied between subjects. We considered that, in some subjects, the inflammation state of NASH might partially improve due to treatment or lifestyle change. However, our findings showed the interaction between cnm-positive S. mutans and aggregation of NASH. The tendency of higher type IV collagen 7S levels in subjects with cnm-positive S. mutans, which has higher affinity to type IV collagen, proposed an alternative bidirectional mechanism between oral caries and NASH. Type IV collagen is a major basement membrane protein of liver parasinusoidal cells.43 After secretion of type IV collagen, the 7S domain in the NH2-terminal polymerisation domain is inserted in tissues and released into the bloodstream by turnover in connective tissue. The increased type IV collagen 7S level correlated with the amount of fibrosis and increase in synthesis from fibroblasts following increasing fibrosis in the liver.44 45 Accumulating evidence demonstrates that fibrosis stage predicts the mortality and morbidity in NAFLD,46 which might support the clinical importance of the interaction between type IV collagen and cnm-positive S. mutans.
In summary, there are mainly two methodological limitations due to the pilot study. The main limitation is the small number of patients with biopsy-proven NASH. There are only 16 patients with histological confirmation for diagnosis of NASH. The other limitation is that we combined subjects with possible NASH due to clinical diagnostic score, which indicate our study incorporates potential errors (false positive and false negative). Even though our preliminary results are based on a small number of subjects, our pilot study does provide a possible association between cnm-positive S. mutans in the oral cavity and NASH. Larger scale evaluation and validation studies are statistically necessary to determine our findings and further assessment of specific biomarkers associated with specific bacteria. Moreover, experimental studies using animal models of dental caries using clinically isolated strains of the pathogen and NAFLD might be essential to elucidate the underlying mechanism of the oral-liver axis, cnm-positive S. mutans might be a possible modifiable factor of intervention for NASH.
Acknowledgments
We thank Christina Croney, PhD, from Edanz Group (www.edanzediting.com/ac), for editing a draft of this manuscript.
References
Footnotes
Contributors Shuichi Tonomura, TH, KM, NT, Saiyu Tanaka, NT and YS participated in patient recruitment. Shuichi Tonomura and TH explained the study to patients, obtained written informed consent and collected oral samples. Shuichi Tonomura, SN, YS, KK, MI and NT designed the study. SN, KT and MM-N performed Streptococcus mutans detection and PCR. Shuichi Tonomura, SN and RN evaluated statistical analyses and drafted the manuscript. RN, MM-N, MI and KN interpreted the data and made substantial comments on the study. All authors approved the final draft submitted.
Funding This research was supported in part by a grant from the Smoking Research Foundation.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The protocol was approved by the ethical committee of Nara City Hospital, Nara, Japan (approval number: NCH 17–32).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.