Article Text

Abstract
Background The probiotic mixture VSL#3 has proven efficacious in inflammatory bowel diseases and irritable bowel syndrome; however, its efficacy in microscopic colitis (MC) is being investigated.
Objective To evaluate the safety and efficacy of a multistrain probiotic, VSL#3, in inducing clinical remission and achieving clinical response, as compared with mesalamine, in patients with active MC.
Methods A randomised, open labelled study comparing the efficacy of 900 billion colony-forming units/day of VSL#3 (group (Gp) A) or 1.6 g of mesalamine/day (Gp B) for 8 weeks in 30 patients with MC was conducted. After a washout period of 2 weeks, Gp B received 8 weeks of VSL#3 and Gp A was off medication for the next 8 weeks. The primary end points were clinical remission and clinical response at 8 weeks.
Results Of 30 patients, 15 were randomised in each arm. 11 patients in Gp A and 13 patients in Gp B completed 8 weeks of treatment. 5 (46%) of 11 patients in Gp A and 1 (8%) of 13 patients in Gp B attained clinical remission (p=0.022). Clinical response was seen in Gp A, as evidenced by a lower stool weight (377.6±104.5 g) as compared with Gp B (507±168.2 g; p=0.03). VSL#3 was effective in maintaining clinical response up to 10 weeks, even after discontinuation of therapy. Secondary end points like stool parameters, histology and well-being improved in both treatment groups.
Conclusions The probiotic VSL#3 was found to offer the benefit of inducing as well as maintaining short-term clinical response in patients with active MC.
Trial registration number The clinical trial is registered with CLINICAL TRIAL REGISTRY INDIA; http://ctri.nic.in, CTRI No. “CTRI/2008/091/000086” (registered on: 23/06/2008).
- MICROSCOPIC COLITIS
- PROBIOTICS
- 5-AMINOSALICYLIC ACID (5-ASA)
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Summary box
What is already known about this subject?
▸ Microscopic colitis (MC) was once thought to be a rare disorder, but it is now apparent that it is a relatively common cause of diarrhoea in middle-aged and elderly patients.
▸ The aetiology of MC is not fully understood; however, altered gut immunity has a role to play in its pathogenesis.
▸ Data demonstrate budesonide to be an effective treatment option, and suggest that prednisolone, bismuth subsalicylate, and mesalamine with or without choloestyramine may be beneficial.
▸ High relapse rates within 2 weeks of discontinuation of budesonide have been observed and long-term budesonide is associated with significant adverse effects.
What are the new findings?
▸ VSL#3 seems to offer the benefit of inducing as well as maintaining short-term clinical response in patients with active MC.
▸ VSL#3 was able to induce clinical remission and achieve partial clinical response but not histological response.
▸ VSL#3 seems to improve the associated symptoms of MC, namely stool weight, frequency and consistency, amount of mucus and general well-being.
How might it impact on clinical practice in the foreseeable future?
▸ Probiotics are one of the safest supplements available today.
▸ Probiotics have been found to be beneficial in patients with inflammatory bowel disease, irritable bowel syndrome, traveller's diarrhoea, etc. The current study demonstrates the efficacy of probiotic VSL#3 in patients with MC by reducing the bowel movements and improving stool consistency, overall improving their well-being and quality of life. Larger studies are implicated; however, they can be tried as a safe therapeutic option in patients with MC.
Introduction
Microscopic colitis (MC) is a chronic inflammatory disorder of the gut characterised by episodic watery diarrhoea occurring most commonly in elderly women with a normal radiological and endoscopic appearance of the colon. Historically, two subtypes of MC were described, collagenous colitis (CC) and lymphocytic colitis (LC), distinguished by the presence or absence of a thickened subepithelial collagen band.1 Falodia et al extended this spectrum and reclassified MC into five subtypes: CC, LC, minimal change colitis, MC with giant cells and MC not otherwise specified (MC-NOS).2–5
Mucosal inflammation and increased intraepithelial T lymphocytes suggest immunological response to luminal agents in predisposed individuals as a possible aetiology.6 This is supported by the reversal of histopathological improvement in CC postileostomy closure.7 Hence, manipulation of luminal bacteria appears to be a promising therapeutic approach.
Therapy for MC is challenging and several drugs have been proposed largely based on case reports, uncontrolled studies and small randomised trials. Of the several agents, budesonide is found to be the most effective in inducing and maintaining remission, but relapse rates on discontinuation are very high. MC has a benign course with resolution of diarrhoea and normalisation of histology in over 80% within 38 months.8 ,9 Thus, the benefit of any drug treatment should be carefully weighed against its potential side effects.
Probiotics are living microorganisms that, when consumed in adequate amounts, may confer a health benefit to the host.10 Only two studies on probiotic therapy in CC have been published using Escherichia coli Nissle, Lactobacillus acidophilus LA-5 and Bifidobacterium animalis, with some response, but its role in treatment remains unclear.11 ,12 VSL#3 is a high-concentration probiotic preparation with growing data on its efficacy in inflammatory bowel disorders.13–15 The objective of this study was to evaluate the safety and efficacy of VSL#3 in inducing clinical remission and achieving clinical response in patients with active MC, compared with mesalamine.
Materials and methods
Study design
This is a two-phase, open labelled randomised trial, conducted in a tertiary care centre (All India Institute of Medical Sciences, New Delhi) in India, from June 2006 to December 2008. All eligible patients received open-label therapy with either VSL#3 (group (Gp) A) or mesalamine (Gp B), in phase I, followed by a 2 week washout period. Subsequently, in phase II, Gp B received VSL#3 and Gp A was closely followed without medications for the next 8 weeks (figure 1).
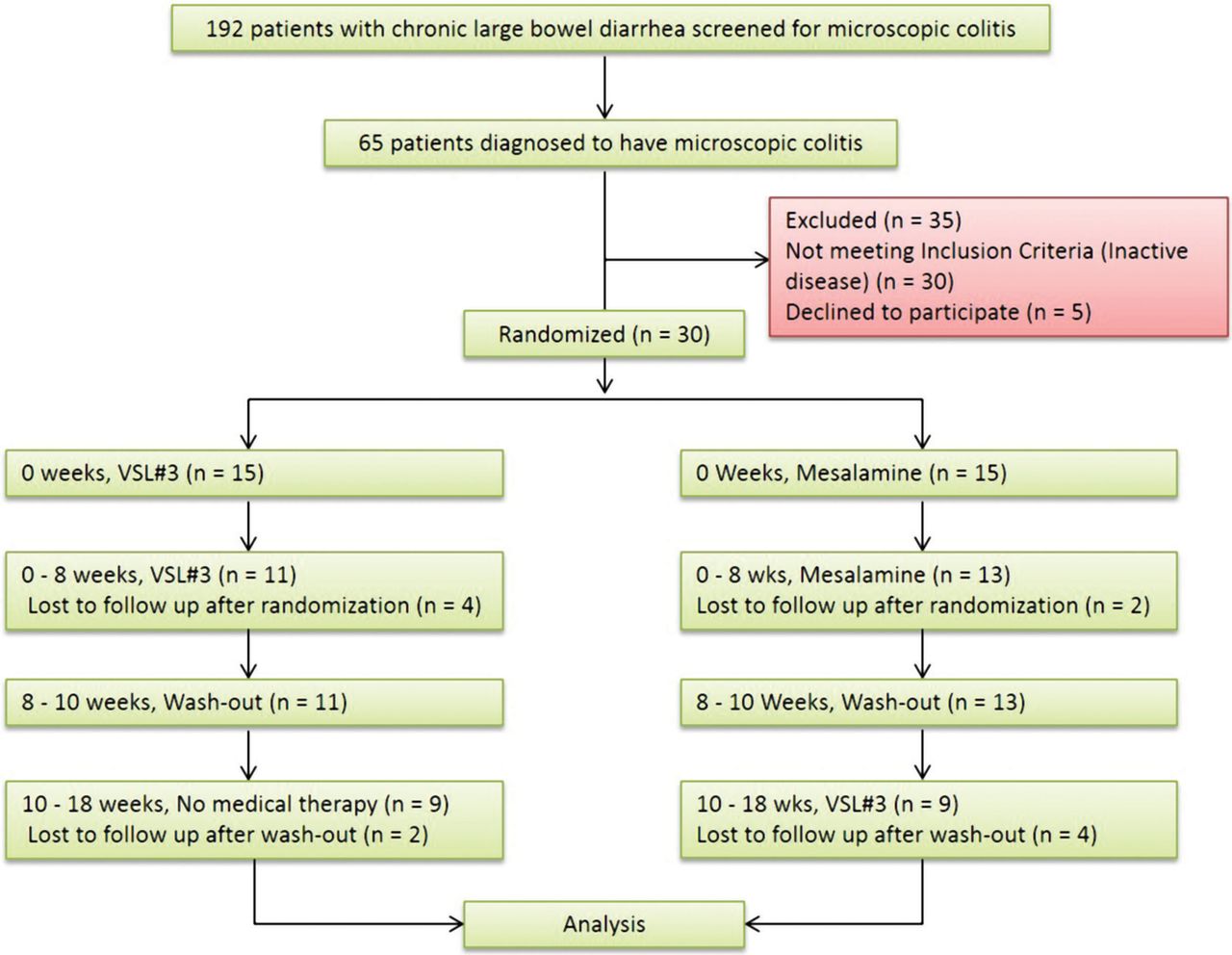
Consort flow chart showing participant flow in both the treatment groups.
At the screening visit, the medical history, demographic data and current medications list were recorded. Baseline blood tests included complete blood count, basic metabolic panel, liver function tests, erythrocyte sedimentation rate, C reactive protein, antinuclear antibody, perinuclear antineutrophil cytoplasmic antibody (p-ANCA), IgA tissue transglutaminase serology and urine pregnancy test. Infection was excluded by stool examination for parasite and bacterial pathogens.
Patients were evaluated at −2, 0, 8, 10 and 18 weeks. All patients recorded their daily symptoms in a symptom booklet, along with intake of concomitant medications, starting at −2 weeks, over 18 weeks. If the patient failed to complete the questionnaire, verbal scoring was performed by patient recollection of past 2 days. Mean stool weight of the past 3 days before scheduled visit at 0 week, 8 weeks and 18 weeks was determined. Physical examination and blood tests were done at 0-week, 8-week and 18-week visits.
Flexible sigmoidoscopy and biopsy were performed at baseline, 8 and 18 weeks by the same investigator. After a normal saline enema, the scope was inserted up to 60 cm. On withdrawal, four random biopsy specimens were taken separated by 10–15 cm each and fixed in separate bottles for histopathological analysis.
Participants
All enrolled patients were ≥18 years of age, symptomatic with histologically proven MC (CC, LC, MC-NOS as reviewed by our gastrointestinal (GI) pathologist).
Inclusion criteria included ≥3 stools per day, stool consistency score >3 and diarrhoea severity score >1, averaged over a week prior to enrolment; ≥8 weeks of watery non-bloody diarrhoea; normal endoscopic appearance of colonic mucosa; no significant neutrophilic/eosinophilic infiltration, crypt abscesses, granulomata or any evidence of inflammatory bowel disease.
Exclusion criteria included pregnant or breastfeeding women; significant hepatic, renal, endocrine, respiratory, neurological or cardiovascular diseases; evidence of infectious or other active diarrhoeal conditions (coeliac disease, hyperthyroidism); previous bowel surgeries; patients on antibiotics, immunosuppression or non-steroidal anti-inflammatory drugs in the past 4 weeks; patients unwilling or unable to give informed consent.
The study was conducted according to the Declaration of Helsinki and adhered to good clinical practice guidelines. All participants provided signed informed consent.
Data collection and storage
The collected data were stored in a password protected institutional computer with limited access only to physicians directly involved in the study. The backup data created regularly were stored in a password protected external hard drive in the principal investigator's office.
Diagnosis of MC
Patients with chronic diarrhoea, apparently normal colonic mucosa and histologically proven MC were screened for recruitment. The patients were classified as CC (subepithelial collagen layer ≥10 µm with chronic mononuclear infiltrates in lamina propria), LC (increased intraepithelial lymphocytes ≥20/100 surface epithelial cells with surface epithelium damage, lymphocytic and plasma cells infiltration in lamina propria and normal collagen layer) or MC-NOS (chronic inflammatory cell infiltrates, subepithelial collagen layer <10 µm, and/or intraepithelial lymphocytosis of 10–20/100 surface epithelial cells).
Study drug
The investigational drug used was VSL#3, a probiotic supplied by CD Pharma India Pvt Ltd (an affiliate of VSL Pharmaceuticals Inc, USA). Each sachet contains 450 billion CFU (colony-forming units) comprising four strains of Lactobacillus (L. acidophilus DSM 24735, L. plantarum DSM 24730, L. paracasei DSM 24733, L. delbrueckii subsp. bulgaricus DSM 24734), three strains of Bifidobacterium (B. longum DSM 24736, B. breve DSM 24732, B. infantis DSM 24737) and one strain of Streptococcus (S. thermophilus DSM 24731). The comparator drug, mesalamine (mesacol 400 mg tablets), was obtained from the manufacturer, Sun Pharmaceuticals Industries Ltd., India.
Randomisation
Eligible patients were randomised in blocks of 6 (1:1) according to a computer generated random list to receive either VSL#3 (one sachet twice daily; 900 billion CFU/day) or mesalamine (2 tablets twice daily, 1600 mg/day). Randomisation and dispensing of drugs was performed by a pharmacist, not involved in the study, in a sealed opaque box to be opened by the patient.
Histopathology
Colonic biopsies were stained with either H&E or a connective tissue stain (Van Gieson, Weigert alcian blue or Sirius red). All the biopsies were reviewed by a single GI pathologist blinded to the treatment.
Scoring pattern was: surface epithelium microulceration, cell flattening and mucin depletion (0: normal; 1: moderate; 2: severe), crypts (0: normal; 1: distorted architecture and/or cryptitis with neutrophils; 2: crypt abscesses), lamina propria (0: normal; 1: focal increase in neutrophils and/or mononuclear infiltrates; 2: diffuse increase in neutrophils and/or mononuclear infiltrates), number of intraepithelial lymphocytes in surface and crypt epithelium assessed separately (0: normal; 1: moderately increased; 2: significantly increased), and thickness of subepithelial collagen layer (0: normal; 1: focal thickening; 2: diffuse thickening). For each of these five parameters, the arithmetic means of the scores from four separate colonic biopsies were calculated. The sum of these five means were then compared within and between groups.
Immunohistochemistry
Tissue slides were incubated with anti-iNOS (inducible nitric oxide synthase) rabbit clonal primary antibody (DB Biotech) at 1:50 dilution. After washing in tris-buffered saline, slides were incubated with a universal secondary antibody (DAKO, Envision real system, Denmark). The iNOS stain was analysed in terms of distribution of staining (1: <30% surface area, 2: 30–60% surface area and 3: >60% surface area) and intensity of staining of the mucosal epithelium, lymphocytes and blood vessels (0: no staining, 1: <control stain intensity, 2: =control stain intensity, 3: >control stain intensity). The total score was determined by multiplying these two scores.
Outcome measures
Primary outcome measure
Primary outcome measures included attainment of clinical remission and clinical response. Clinical remission was defined as the proportion of patients reporting a reduction in stool frequency or stool weight by ≥50% at 8 weeks. Clinical response was defined as a significant reduction in stool frequency or stool weight at 8 weeks.
Secondary outcome measure
Secondary outcome measures included improvement in stool frequency (no. of bowel movements per day); diarrhoeal rate (0: normal stools, no diarrhoea; 1: up to 4 loose stools per day above normal, 2: 5–7 loose stools per day above normal, 3: >7 loose stools per day above normal); stool consistency (Likert scale, 1: very hard; 2: hard; 3: formed; 4: loose; 5: watery); abdominal pain and stool mucus (Likert scale, 0: none; 1: mild; 2: moderate; 3: severe); overall well-being score (visual analogue scale, 1–5: lower score signifies better well-being); histopathological response (reduction of histopathological score by ≥50%); and iNOS immunohistochemical response (significant reduction in total score).
Assessment of compliance and safety
Compliance was evaluated by interview and counting of returned empty study drug sachets or strips. Patients with <80% medication consumption were considered non-compliant. Safety was assessed by detailed medical history, physical examination, serum biochemistry, etc.
Sample size calculation and statistical analysis
For comparing therapeutic effects of VSL#3 and mesalamine, a two-phase partial crossover trial was designed. Superiority margin was predefined as a 25% difference in clinical responses between the two treatments in phase I. For a power of 80% and α value of 5%, we calculated the sample size of 25 patients. Keeping a 10% provision for dropouts, a total sample size of 30 was planned. Comparisons between VSL#3 and the mesalamine group for various parameters were performed by unpaired t tests and non-parametric tests. Intragroup comparisons were done by the paired t test or non-parametric Wilcoxon signed rank-sum test. Comparison for categorical variables between groups was performed by the χ2 test/Fisher exact test. A p value of ≤0.05 was considered statistically significant. Data were analysed using SPSS statistical software V.16.0 (SPSS Inc, Chicago, Illinois, USA).
Statistical analysis of all data sets pertaining to efficacy and safety was independently performed by a biostatistician not employed by the corporate entity.
Results
Participant flow
Of 65 patients diagnosed with MC, 30 did not meet the inclusion criteria and five refused to consent. Thirty patients were randomised to receive either VSL#3 (Gp A, n=15) or mesalamine (Gp B, n=15). Eleven patients in Gp A and 13 patients in Gp B completed phase I and entered phase II. Finally, nine patients in each group completed the 18-week visit (figure 1).
Baseline data
Baseline characteristics of patients are given in table 1. No significant difference was found in age, gender distribution and blood test results between the two groups. Similarly, study parameters like stool frequency, stool weight, consistency and mucus, diarrhoeal rate, abdominal pain and well-being were comparable between the two groups.
Demographic and baseline characteristics of patients
Clinical efficacy of VSL#3 and mesalamine at 8 weeks
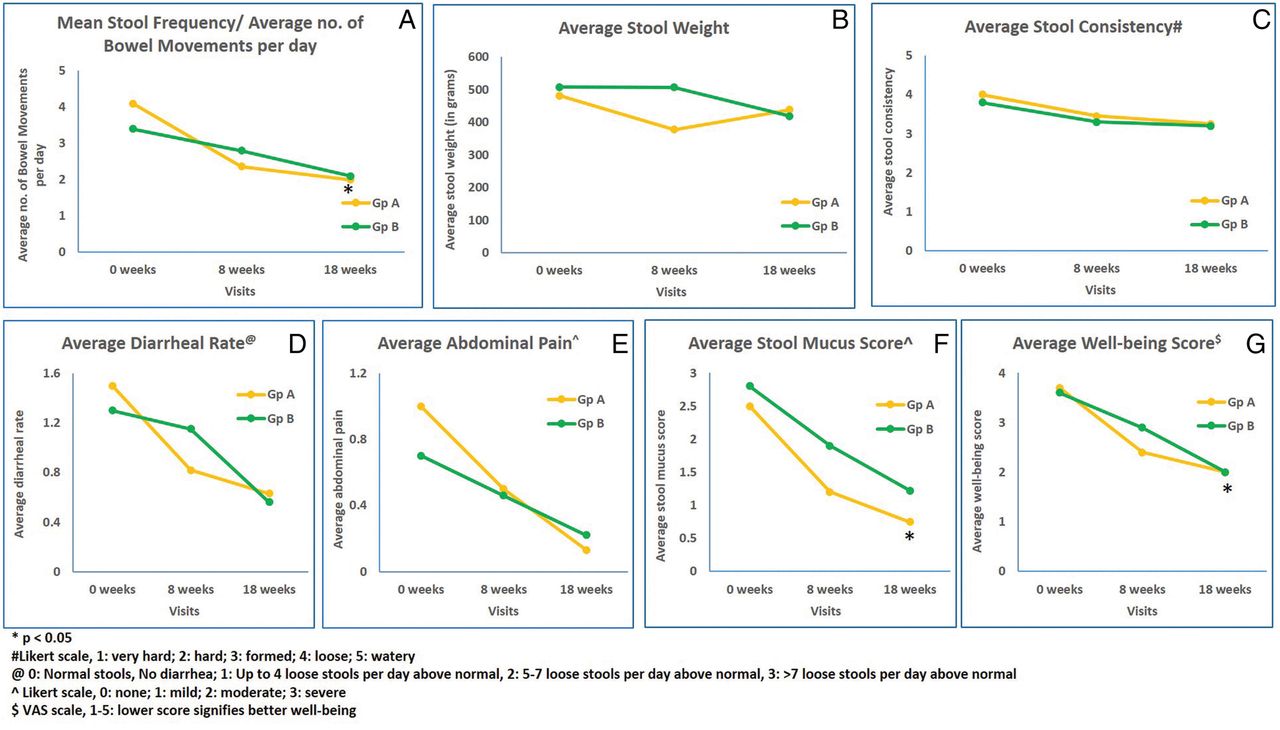
In Gp A, VSL#3 significantly decreased stool frequency, stool weight, stool mucus, diarrhoeal rate, with improvement in well-being, but there was no significant improvement in stool consistency and abdominal pain (figure 2A–G). In Gp B, mesalamine significantly decreased stool mucus and improved stool consistency and well-being but no significant changes were observed in other parameters (figure 2). Weight loss was observed across both groups at 8 weeks; however, it was non-significant (mean weight loss of 200 g in Gp A and 600 g in Gp B; p=NS)

Within-group comparison of stool parameters from 0 to 8 weeks (Gp, group; VAS, visual analogue scale). VSL#3 significantly decreased stool frequency, stool weight, stool mucus, diarrhoeal rate, with improvement in well-being. Mesalamine significantly decreased stool mucus and improved stool consistency and well-being.
Five of 11 (46%) patients in Gp A and 1 of 13 (8%) patients in Gp B achieved the primary outcome measure by demonstrating ≥50% reduction in stool frequency or stool weight (p=0.022; not shown in the figure or table). Gp A achieved clinical response by showing a significant reduction in stool weight (p=0.03, table 2), but the reduction in stool frequency was comparable between the two groups (p=0.31, table 2). Secondary outcome of significant reduction in stool mucus was achieved in Gp A when compared with Gp B (table 2), but other parameters were comparable.
Comparison of efficacies of VSL#3 and mesalamine at 8 weeks
Temporal effect of VSL#3 therapy
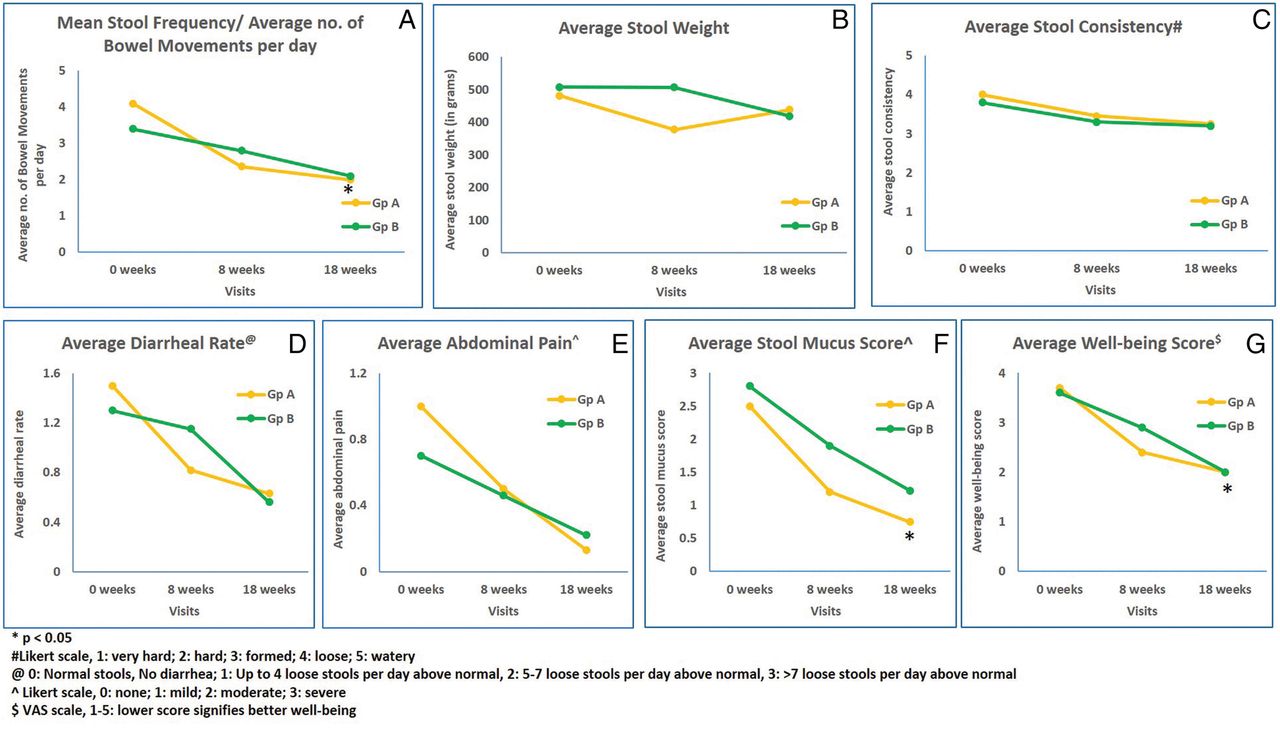
In Gp A, nine patients completed phase II. A beneficial effect of VSL#3 seems to be maintained throughout the 18 weeks as noted by continued significant improvement in stool frequency, stool mucus and well-being (figure 3A, F, G). An improvement trend in stool consistency, diarrhoeal rate and abdominal pain along with an increase in stool weight was noted, but none of it was significant (figure 3B–E).
Changes in secondary outcome measures from baseline to 18 weeks (Gp, group; VAS, visual analogue scale).The beneficial effect of VSL#3 seems to be maintained throughout the 18 weeks study period, observed as continued significant improvement in stool frequency, stool mucus and well-being.
Effects of VSL#3 therapy in patients after 8 weeks treatment with mesalamine
In Group B, nine patients completed the second phase. Improvement was noted in all study parameters (p=NS; figure 3A–G), except stool consistency.
Histological and immunohistochemistry findings
Colonic biopsies for all three time points (0, 8 and 18 weeks) were available for 15 patients (Gp A: 7, Gp B: 8). The mean histological score after treatment showed no improvement in either of the treatment groups. The mean histological activity scores were 3.25±1.04, 4.13±1.54 and 4.83±1.79 at 0, 8 and 18 weeks, respectively, in Gp A. In Gp B, the mean histological scores were 3.70±1.98, 5.19±1.55 and 4.34±1.75 at 0, 8 and 18 weeks, respectively.
A significant decrease in the iNOS immunohistochemical staining scores was noted in Gp A at 8 weeks (3.2±0.70 vs 1.6±0.91; p=0.017), and at 18 weeks (1.8±0.9, p=0.027), as compared with baseline. However, in Gp B, the iNOS staining scores were comparable at 8 weeks (2.2±0.48 vs 2.0±0.81, p=0.48) and 18 weeks (1.8±0.67; p=NS), when compared with baseline (figure 4). The iNOS scores increased slightly after discontinuation of VSL#3 in Gp A, but decreased further in Gp B after initiation of VSL#3 administration. The decrease in Gp B, however, could not reach statistical significance.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Photomicrograph showing a biopsy of lung adenocarcinoma used as a positive control for inducible nitric oxide synthase (iNOS) immunostain. There is strong immunopositivity in the tumour cell nuclei and cytoplasm ((A) immunohistochemistry (IHC; iNOS) ×200). Photomicrograph of a biopsy showing baseline collagenous colitis; there is strong and diffuse immunopositivity for iNOS immunostain in surface and crypt mucosa. Few lymphocytes also showing positivity for iNOS ((B) IHC (iNOS) ×100). Eight weeks after VSL#3 treatment, there is a marked reduction in the area distribution and stain intensity of iNOS immunostain ((C) IHC (iNOS) ×40; Blue arrow showing nuclear positivity). Eighteen weeks post VSL#3 treatment, there is still a very minimum expression of iNOS in the colonic biopsy ((D) IHC (iNOS) ×40; Brown arrow showing occasional nuclear positivity).
Concomitant medications and diet
There were seven patients on concomitant medications, two patients on antihypertensives, two patients on pantoprazole for gastric ulcer, one patient on antidiabetics, one patient on prokinetics for irritable bowel syndrome (IBS) and one patient on leflunomide for rheumatoid arthritis. Few patients used paracetamol and antibiotics for 3–4 days in fever and upper respiratory tract infections. No change in food habits or fibre intake was prescribed or allowed during the entire trial duration.
Compliance and tolerability
All patients who completed the study showed ≥80% compliance. VSL#3 was found to be safe and well tolerated. Two patients in Gp A reported abdominal pain, bloating and altered taste for a few days, but resolved without treatment. Abdominal pain and bloating in three patients and dry mouth in one patient was reported in Gp B, which are well-known side effects of mesalamine. None of the patients in either group discontinued therapy due to any adverse events.
Discussion
This open labelled randomised controlled study compares the effect of VSL#3 with mesalamine in patients with active MC. At 8 weeks, VSL#3 appears to be better than mesalamine in inducing clinical remission (p=0.022) and in achieving clinical response by reducing stool weight (p=0.03) and mucus (p=0.03). On crossover, VSL#3 therapy led to a further decrease in stool weight and frequency, although it was not significant. Continued improvement seen in patients without treatment endorses the possibility of the VSL#3 effect being maintained for at least 10 weeks after discontinuing therapy. Also, a significant reduction in iNOS scores in Gp A is suggestive of improvement in the inflammatory status of the disease. VSL#3 therapy in phase II treatment in Gp B showed a decrease in iNOS, but the change was comparable as the patients had already improved after phase I treatment with mesalamine.
There have been several small trials on the management of MC, but evidence for Budesonide is most persuasive.16 A Cochrane review by Chande et al8 showed that budesonide achieves a clinical response in 81% (95% CI 67% to 90%) of patients after 6–8 weeks of treatment compared with placebo (17%; 95% CI 9% to 30%; p<0.00001). In two other budesonide trials, 75% patients maintained clinical response for 6 months on therapy (p<0.0001), but clinical relapse occurred in 61–88% of patients on treatment discontinuation, with a median time to relapse of 2–5 weeks.8 ,17–19
This raises two important issues. First, the rate of relapse after discontinuing budesonide is very high and does not depend on the duration of induction therapy.20 Second, although budesonide is well tolerated, it may lead to steroid-related adverse effects after short-term and long-term therapy. Thus, the chronicity of MC demands a well-tolerated long-term therapy with minimal side effects. Hence, a need arises to consider alternative therapies.
Munch et al,21 in their study of 46 budesonide-dependent or budesonide-intolerant patients with active MC, showed long-term clinical remission in 28% patients with azathioprine.22 Other immune suppressants such as methotrexate, adalimumab and antitumour necrosis factor (TNF) therapies have also been used in refractory MC for attaining clinical remission, improving quality of life and possibly avoiding colectomy.23 ,24
Mesalamine has been evaluated only in one study, though several case reports have been published. In Calabrese et al's25 study, 8/11 patients clinically responded to mesalamine alone compared with a 100% response to mesalamine and cholestyramine (p=0.14). Mesalamine appears to work topically, with no established or suggested dosing for MC and different trials, and case reports have used a wide dose range of 1.5–2.4 g/day. Since there was no evidence on specific dosing of mesalamine in MC, we used a dose of 1.6 g/day considering that the body mass index of Asians is lower than Caucasians.
Probiotics have a good safety profile. Reported cases of infection from Lactobacilli and Bifidobacteria are extremely rare, mostly associated with extreme ages and/or immunosuppression.10 ,26–30 The precise mechanism of action of VSL#3 is unknown, but in vivo and in vitro studies have shown that VSL#3 modulates host-immune response, improves the epithelial barrier function, increases mucus production and reduces proinflammatory factors in the colon. It increases anti-inflammatory cytokine interleukin (IL)-10, and inhibits secretion of proinflammatory cytokines such as TNF-α, interferon gamma and IL-1β.10 ,28 ,31 Dai et al32 showed that VSL#3 was effective in inducing and maintaining remission in acute colitis in rodent models by reducing myeloperoxidase activity, evident by the decreased expression of inflammatory mediators (iNOS, nuclear factor κB, etc) and cytokines and increased expression of IL-10, in colonic tissue and serum. Even though our work did not show significant improvement in abdominal pain with VSL#3, Distrutti et al33 reported downregulation of the tryptophan hydroxylase-1 gene, involved in pain transmission and inflammation, with the VSL#3 therapy of murine models of IBS, suggesting potential benefit with long-term use.
The strength of our study is the two-phase partial crossover design which shows that the beneficial effect of VSL #3 may be maintained up to 10 weeks postinduction therapy. The two published trials on the use of probiotics in MC have not found any advantage over placebo, unlike our trial which shows evidence of clinical improvement.11 ,12
Limitations of our study include a small sample size, only 8 weeks of therapy to study histological response and an open labelled study design owing to the practical limitation of available medications. However, the physicians and pathologists involved in the study were blinded to drug allocation. MC is reported to be more common in elderly women; however, in our study, 73% of the recruited patients were males. The sex break-up is similar to that in an earlier report by Falodia et al,5 where the authors reported 75.8% of study population to be males. This may be due to the fact that Indian males have more and better access to tertiary medical care as compared with Indian females, as a result of which three-fourths of our study population were males. MC is more prevalent than was previously thought, but the lower incidence explains our small sample size. Hence, a study with a longer induction period and a larger sample size would be ideal to show complete benefit from VSL#3 as suggested by our study.
In summary, we conclude that in patients with active MC, VSL#3 offers a potential benefit of inducing as well as maintaining short-term clinical remission as compared with mesalamine.
Acknowledgments
The authors sincerely acknowledge the help of Mr. Aditya Ranjan Sahu in the conduct of the study and preparation of the manuscript.
References
Footnotes
Contributors SR contributed to the study concept and design, acquisition of data, analysis and interpretation of data, and drafting of the manuscript. VA is the guarantor of the article; he contributed to the study concept and design, study supervision, acquisition of data, analysis and interpretation of data, drafting of the manuscript, critical revision of the manuscript, statistical analysis; he also obtained funding, and provided technical and material support. GKM contributed to study concept and design and critical revision of the manuscript. TR, PD and VM contributed to acquisition, analysis and interpretation of data, and drafting of the manuscript. SD contributed to acquisition, analysis and interpretation of data, and drafting and critical revision of the manuscript. SKG contributed to analysis and interpretation of data, drafting and critical revision of the manuscript and statistical analysis. All authors have approved the final version of the article.
Funding This trial has been sponsored by CD Pharma India Pvt Ltd (a VSL affiliate), New Delhi, India.
Competing interests None.
Patient consent Obtained.
Ethics approval The trial project has been approved by the ‘Institute Ethics Committee’, All India Institute of Medical Sciences, New Delhi, India (Reference No. A 64: 12-08-2005).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.