Article Text

Abstract
Introduction Transjugular intrahepatic portosystemic shunt (TIPS) placement is a well-established but technically challenging procedure for the management of sequelae of end-stage liver disease. Performed essentially blindly, traditional fluoroscopically guided TIPS placement requires multiple needle passes and prolonged radiation exposure to achieve successful portal venous access, thus increasing procedure time and the risk of periprocedural complications. Several advanced image-guided portal access techniques, including intracardiac echocardiography (ICE)-guided access, cone-beam CT (CBCT)-guided access and wire-targeting access techniques, can serve as alternatives to traditional CO2 portography-based TIPS creation.
Methods A literature search was performed on the electronic databases including MEDLINE and Embase, from 2000 to the present to identify all relevant studies. The reference list also included studies identified manually, and studies referenced for other purposes.
Findings The main benefit of these advanced access techniques is that they allow the operator to avoid essentially blind portal punctures, and the ability to visualise the target, thus reducing the number of required needle passes. Research has shown that ICE-guided access can decrease the radiation exposure, procedure time and complication rate in patients undergoing TIPS placement. This technique is particularly useful in patients with challenging portal venous anatomy. However, ICE-guided access requires additional equipment and possibly a second operator. Other studies have shown that CBCT-guided access, when compared with traditional fluoroscopy-guided access, provides superior visualisation of the anatomy with similar amount of radiation exposure and procedure time. The wire-targeting technique, on the other hand, appears to offer reductions in procedure time and radiation exposure by enabling real-time guidance. However, this technique necessitates percutaneous injury to the liver parenchyma in order to place the target wire.
Conclusion Advanced portal access techniques have certain advantages over the traditional fluoroscopically guided TIPS access. To date, few studies have compared these advanced guided access options, and further research is required.
- interventional radiology
- portal hypertension
- cirrhosis
Data availability statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Since its introduction almost 40 years ago, transjugular intrahepatic portosystemic shunt (TIPS) placement has become a well-established procedure for managing sequelae of portal hypertension such as variceal bleeding, refractory ascites and hepatic hydrothorax on optimal medical therapy. Further, TIPS placement is used as salvage therapy for acute gastrointestinal variceal haemorrhage, as secondary prophylaxis for oesophageal or gastric variceal bleeding, and as early prophylaxis after initial variceal bleeding.1–4 Despite its efficacy, however, TIPS placement remains one of the more technically challenging endovascular procedures .
Traditionally, TIPS placement is performed with fluoroscopic guidance. Wedged CO2 portography is performed to demonstrate the main portal vein anatomy and its major branches. Using the two-dimensional (2D) CO2 portography as a virtual roadmap, the operator makes needle passes from the appropriate hepatic vein into the target portal branch until a direct portohepatic venous connection is made. The tract is subsequently dilated and stented. The most challenging step is direct cannulation of the portal branch from the hepatic venous branch, as the needle pass is performed essentially blindly in a three-dimensional (3D) volume with a 2D road map for reference. Multiple needle passes are often required for successful cannulation, especially for inexperienced operators and in cases of more challenging portal venous anatomy.
The main perioperative complications of traditional fluoroscopic TIPS placement stem from these multiple needle passes and may include inadvertent injuries to the liver capsule, extrahepatic portal vein, hepatic artery, biliary ducts or surrounding viscera.5 Hepatic artery injury can occur in up to 6% of the cases, and clinically relevant biliary injury is reported in 5% of the cases.5 In addition, repeated cannulation prolongs procedure time (including anaesthesia time) and increases the radiation dose.6 Lastly, CO2 extravasation is reported in 1.8% of cases; this complication can lead to serious morbidities such as hepatic capsular laceration which is a known though rare cause of immediate intraprocedure mortality.7
To mitigate some of these challenges, a variety of technical innovations have been proposed to provide image-guided safe portal access, including alternative access options such as intracardiac echocardiography (ICE) catheter-guided portal access, wire-targeting access and cone-beam CT (CBCT)-guided access techniques. In this paper, we describe these alternative access options based on our extensive clinical experience.
Intracardiac echocardiography catheter-guided access
Initially conceptualised by Kew and Davies,8 the technique uses a side-firing ICE catheter for intraoperative ultrasound navigation. At our institution, we typically use the Acuson X300 AcuNav ICE catheter (Siemens Healthineers, Erlangen, Germany). This catheter is a side-firing, 8 French system with an ultrasound probe that operates at 3 to 10 MHz and provides a 90° acoustic window. It allows for grayscale and colour Doppler imaging, as well as depth, angular and rotational control.
The preprocedural workup for ICE-guided TIPS placement does not differ from that of traditional fluoroscopy-guided TIPS placement. Patients with a high Model for End-Stage Liver Disease score (>25) should not undergo TIPS placement unless they are being treated for life-threatening variceal haemorrhage which cannot be controlled with endoscopy. Contraindications to the procedure include the presence of at least moderate pulmonary hypertension, right heart failure or uncontrolled hepatic encephalopathy. At our institution, the procedure is typically performed under general anaesthesia so that patients are not affected by the uncomfortable cannulation, tract dilation and catheter manipulation.
The inferior vena cava (IVC), femoral vein, internal jugular vein, hepatic vein and main portal branches should first be assessed carefully on preprocedural cross-sectional imaging. Under ultrasound guidance, venous access is then obtained into either the femoral or internal jugular vein. Right common femoral venous access is preferred, as it offers a straightforward path to the intrahepatic IVC. However, using the ICE catheter via the right common femoral venous access requires a second operator, with the first operator navigating the TIPS needle from the selected hepatic vein into the portal venous branch. If the ICE catheter is instead inserted through the right internal jugular vein, this may enable the experienced operator to run the ultrasound device with one hand while managing the TIPS needle pass with the other hand.
To introduce the ICE catheter, an 8 French sheath is advanced into the venous access site over a 0.035-inch Bentson guidewire. The ICE catheter is then advanced through the sheath and is negotiated into the intrahepatic IVC. Because the ICE catheter does not allow for over-the-wire placement, care must be taken to ensure slow and steady advancement to avoid device kinking or damage of IVC wall/branch vessels. We typically advance the sheath over the Bentson guidewire to the level of the IVC–right atrial junction and then remove the guidwire. Next, we bring the ICE catheter tip-to-tip with the 8 French sheath and unsheathe the ICE catheter. We then carefully retract the ICE catheter until it reaches the ideal position to provide visualisation of both the TIPS sheath within the selected hepatic vein and the target portal venous branch (figures 1 and 2).
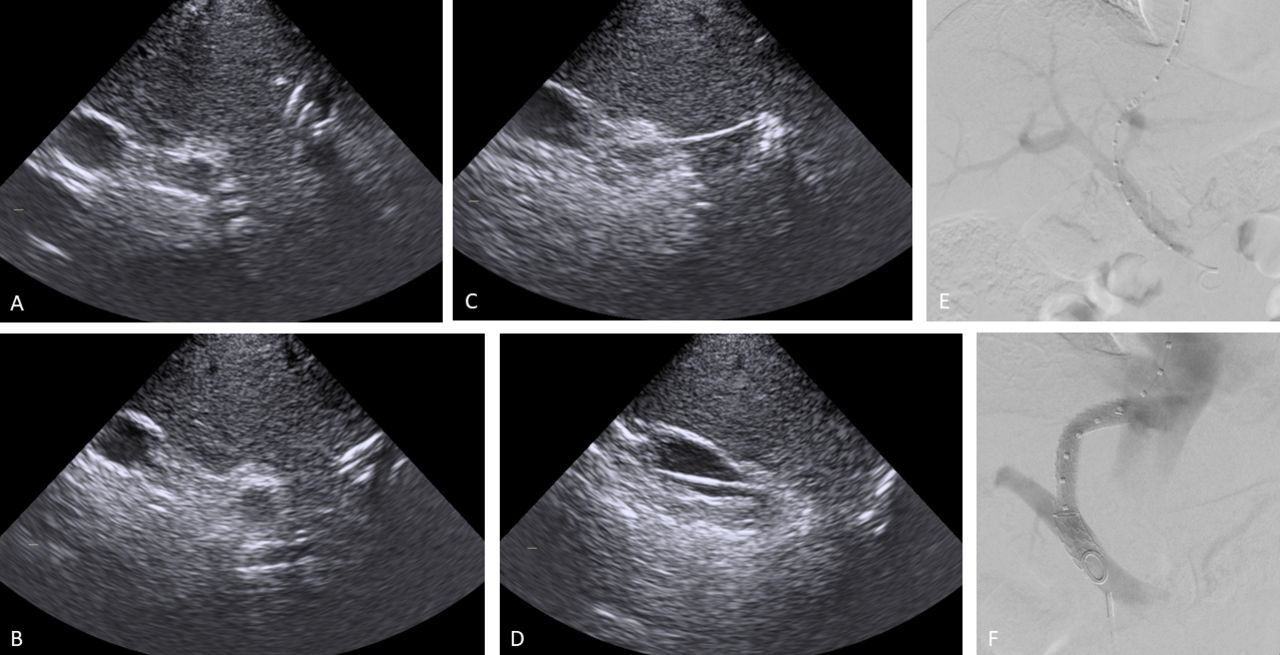
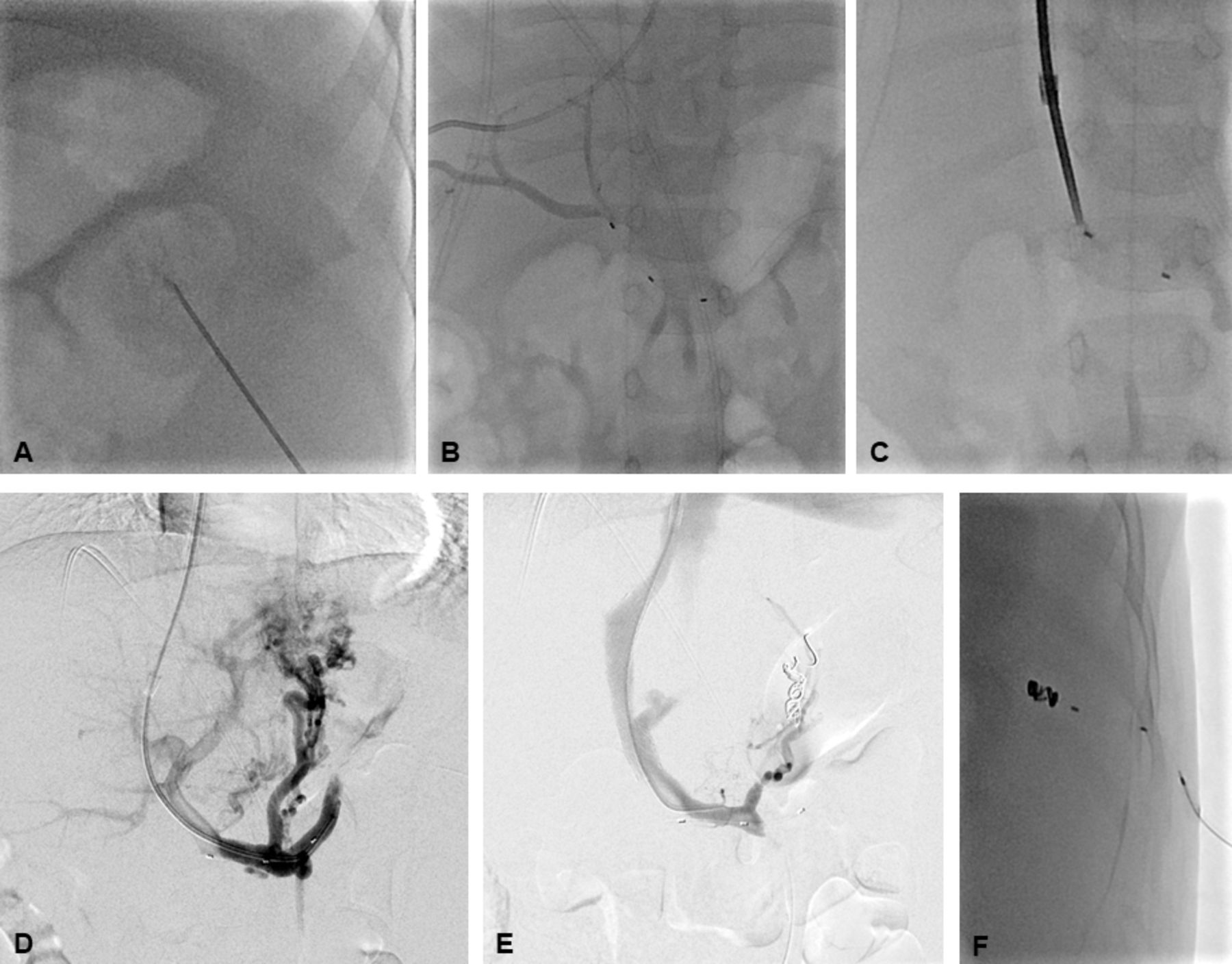
Middle-aged patient with a history of liver cirrhosis presented with haematemesis. Oesophagogastroduodenoscopy demonstrated gastric varices in the setting of portal hypertension. For TIPS creation, access was obtained into the portal venous system using ICE catheter guidance. (A) The TIPS needle is seen within the middle hepatic vein, with direct visualisation of the portal venous system as the target. (B) The TIPS needle is visualised advancing through the hepatic parenchyma towars the proximal left portal vein. (C) The TIPS needle is shown within the hepatic parenchymal tract reaching the proximal left portal vein. (D) The ICE catheter demonstrates the wire and catheter within the main portal vein. (E) On digital subtraction angiography, the access for TIPS creation is depicted between the middle hepatic vein and the most proximal portion of the left portal vein, with a 5 French flush pigtail catheter formed within the main portal vein. Of note, the ICE catheter tip is faintly seen within the inferior vena cava, at the level of the main portal vein. (F) A widely patent TIPS stent with brisk flow of contrast has been created. As expected, residual flow of contrast into the right portal vein is present, thereby ensuring portal venous supply to the right liver lobe. The ICE catheter tip is again faintly seen within the inferior vena cava, at the level of the main portal vein. For this patient a Viatorr 6+2 cm stent (Gore medical, Flagstaff, Arizona, USA) was placed and dilated using an 8 mm high-pressure balloon. The portal venous-atrial gradient was decreased from 9 mm Hg to 4 mm Hg. ICE, intracardiac echocardiography.
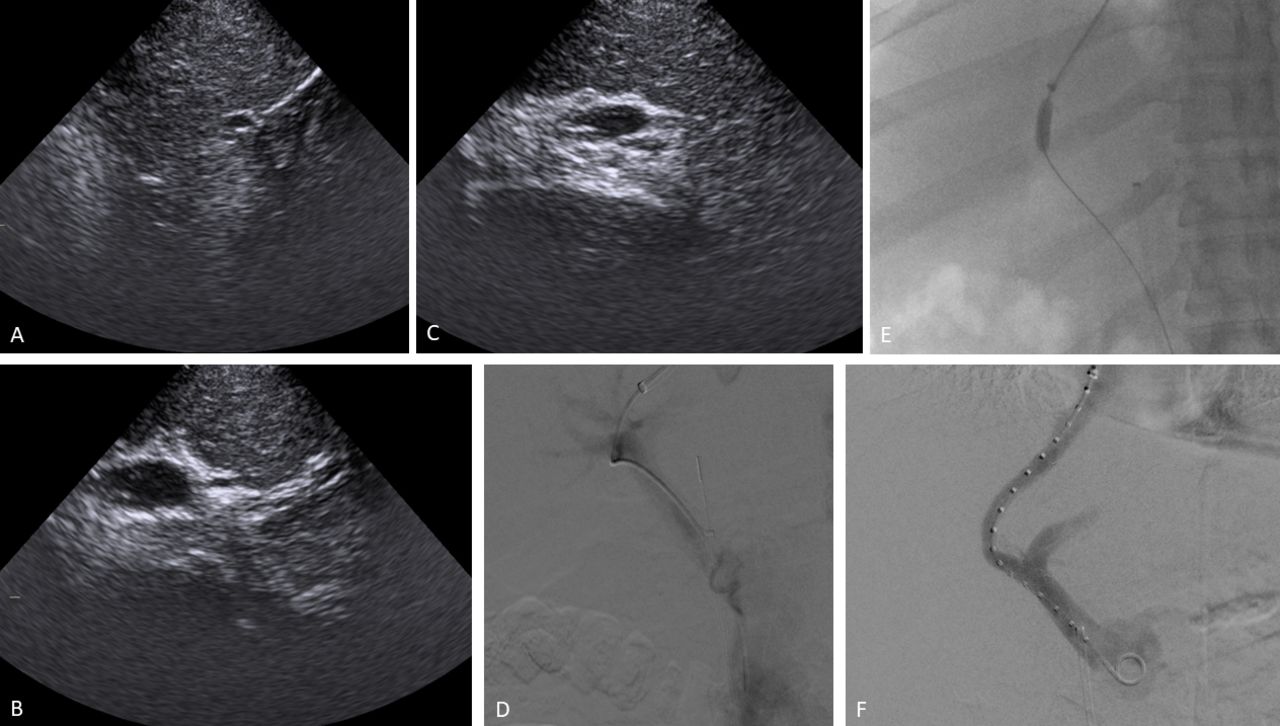
(A) Middle-aged patient with liver cirrhosis and portal hypertension presented with melena to an outside Hospital. Oesophagogastroduodenoscopy demonstrated gastro-oesophageal varices. TIPS creation was attempted at the outside Hospital but had to be aborted because of multiple unsuccessful attempts to gain access into the portal venous system. The patient was referred to our institution for ICE catheter-guided TIPS placement. (A) ICE catheter guidance is used to navigate the TIPS needle from the right hepatic vein toward a branch of the right portal vein. (B) Access into the branch of the right portal vein has been obtained via ice catheter guidance. (C) The ICE catheter shows wire advancement into the main portal vein. (D) Digital subtraction angiography confirmed access into the portal venous system, with the parenchymal tract visualised. A 4 French Glidecath is in place from the right hepatic vein through the right portal vein branch, with the tip of the catheter within the superior mesenteric vein. of note, the ICE catheter tip is faintly seen within the inferior vena cava, at the level of the proximal main portal vein. (E) Parenchymal tract dilatation with a 6 mm compliant balloon as depicted on fluoroscopy. (F) A widely patent TIPS stent with brisk flow of contrast is demonstrated on digital subtraction angiography. As expected, residual flow of contrast into the left portal vein is visualised, ensuring portal venous supply to the left liver lobe. A Viatorr 8+2 cm stent was placed and dilated using 8- and 9 mm high-pressure balloons. The portal venous-atrial gradient was decreased from 12 mm Hg to 8 mm Hg. ICE, intracardiac echocardiography.
Once the ICE catheter is advanced to the intrahepatic IVC, there is usually an excellent acoustic window through the caudate lobe (often hypertrophied in the setting of liver cirrhosis) into the adjacent liver parenchyma. The ICE catheter can then be rotated to identify the hepatic confluence, with converging hepatic veins typically seen. The probe is then rotated clockwise or posteriorly to identify the aorta and the retroperitoneal fat. Once the left-right anatomical orientation is ascertained, the probe can be rotated counterclockwise or anteriorly to identify the right hepatic vein, which is usually seen in profile. The probe can be adjusted in the craniocaudal dimension by advancing or retracting the probe and in the medial-lateral dimension by increasing or decreasing the ultrasound beam depth. Careful counterclockwise or anterior rotation of the probe can be used to identify the posterior right portal branch, which is typically seen in cross-section. Further anterior rotation of the probe usually brings the anterior right portal branch into the field of view. The operator can then retract the probe to trace the portal branch until it reaches the main portal venous confluence. A sweep at this level can offer sufficient evaluation of the main portal trunk to identify evidence of intraluminal thrombus, stenosis, web formation or other pathologies. Once the portal branches are identified, the probe is then negotiated such that the right hepatic vein is again seen longitudinally and the right portal vein is again seen in cross-section on a single ultrasound view. At this point, the ICE catheter should be held in place to allow for continuous visualisation of relevant portal and hepatic branches while access is obtained from the selected hepatic venous branch into the portal venous branch. Again, careful adjustment of the ultrasound probe in the craniocaudal dimension is needed to avoid inadvertent damage to the IVC, its side branches or the caudal portion of the right atrium.
For TIPS placement, initial access is obtained under ultrasound guidance via either the right (preferred) or left internal jugular vein. A 9 French 35 cm Brite Tip sheath is advanced over the guidewire. The right atrial pressure, free hepatic pressure and wedged hepatic pressures are obtained in the usual fashion. If the pressure measurements are suitable for TIPS placement, the venous access is sequentially dilated and is exchanged for the TIPS sheath. Next, the right hepatic vein is cannulated with the TIPS sheath, which should be visualised by the ICE catheter. The TIPS sheath should be positioned such that the target portal branch is directly anterior and inferior to the sheath (in the classic right hepatic vein to right portal vein approach), with the sheath then rotated such that the anticipated needle path is directly aimed towards the target portal branch. Slight angle modification of the needle and sheath may be needed to better match the anticipated needle trajectory. The needle is then advanced under real-time ICE catheter guidance just beyond the TIPS sheath toward the portal venous branch without traversing the liver capsule. Care must be taken to account for fibrotic parenchyma, as the needle trajectory may be affected by the tissue stiffness. Because direct visualisation is available for this step, CO2 portography is not needed. The entire needle trajectory can usually be visualised in the same imaging plane. Occasionally, in cases of tortuous vessels or difficult anatomy, the ICE probe will need to be rotated slightly to capture the needle path while continuously visualising the target portal branch. Once the needle tip is visualised within the right portal branch, the location can be confirmed with aspiration of blood or contrast injection. Next, a guidewire (typically a 0.035-inch angled Glidewire) is advanced via the accessed right portal branch into the main portal vein, and the tract is subsequently dilated, followed by stent placement. The steps after portal venous access are beyond the scope of this article; previous papers have discussed the technical details of this procedure.9 10
There is a steep learning curve associated with using an ICE catheter. Anatomical orientation of relevant vessels may be confusing for beginners, particularly because the orientation is flipped on the horizontal plane. Users should, therefore, be familiar with the cross-sectional anatomy on preprocedural imaging, with particular attention paid to the anatomical relationship between the hepatic and portal vessels.
Wire-targeting technique
Teitelbaum et al11 described a technique involving placement of a platinum-tipped guidewire in a portal venous branch as a target for fluoroscopic transvenous access to facilitate TIPS placement. The wire-targeting technique is particularly useful for patients with cirrhosis, as the distorted parenchymal architecture can render transvenous access from a hepatic venous branch to a portal venous branch difficult. At our institution, some operators use this procedure as the primary method for portal access.
As previously described, access is gained into a hepatic vein with a TIPS sheath. The right hepatic vein is typically preferred because of its lateral position and ease of access from an internal jugular approach. However, in our experience, one of the advantages of the wire-targeting technique is that it facilitates access into the portal venous system even when a middle or left hepatic vein is selected. Once access has been gained into a hepatic vein with the TIPS sheath, direct venography is performed through the sheath to confirm its position. Traditional CO2 wedge portography is again not required when using the wire-targeting technique.
To this point, the steps used with this technique are identical to those involved in a traditional TIPS placement. The variation with this technique lies in the percutaneous portal access. If ascites is present, paracentesis should be performed before percutaneous access is obtained. Under real-time ultrasound guidance, a portal vein branch is accessed percutaneously with a 21-gauge echogenic tip Chiba needle. Typically, the right portal vein is accessed when the right hepatic vein is used for TIPS stent placement because of the proximity of these two veins. Once the portal vein is accessed, a small 5 French sheath is placed. A 5 French flush pigtail catheter is then advanced through the venous access, and direct iodine based contrast portography is performed. The direct portal pressure is obtained. Next, the 5 French pigtail catheter is exchanged over a guidewire for a straight catheter such as a 5 French MPA catheter or Kumpe catheter. Under fluoroscopic guidance, the position of the catheter is adjusted so that it lies in close proximity to the selected hepatic venous branch, allowing for the most direct tract for TIPS stent placement; this position is usually anterior and inferior to the TIPS sheath in the traditional right hepatic vein-to-right portal vein TIPS stent placement. We tend to use the 5 French catheter in the portal vein branch as our target; however, the catheter can be exchanged for a traditional wire target or a platinum-tipped guidewire based on operator preference. A TIPS access needle is passed through the TIPS sheath from the hepatic vein branch into the portal vein branch using the percutaneously placed 5 French catheter as a target. Transvenous access is obtained with a wire advanced through the needle into the main portal vein, and the position is confirmed by direct portography (using a 4 French Glidecath) though the internal jugular venous access site. Once portal vein access has been confirmed, the parenchymal tract can be dilated with a balloon and a TIPS stent can be placed, with poststent angioplasty (figure 3). Finally, post-TIPS pressure measurements of the right atrium and portal vein are obtained in the traditional fashion. Once adequate decompression of the portal pressure has been confirmed, the sheath in the internal jugular vein is removed, and haemostasis is obtained by applying direct pressure to the internal jugular vein access site. For the percutaneous access site, we typically perform closure by deploying through the 5 French sheath a combination of pushable coils and Gelfoam slurry using the ‘sandwich technique.’

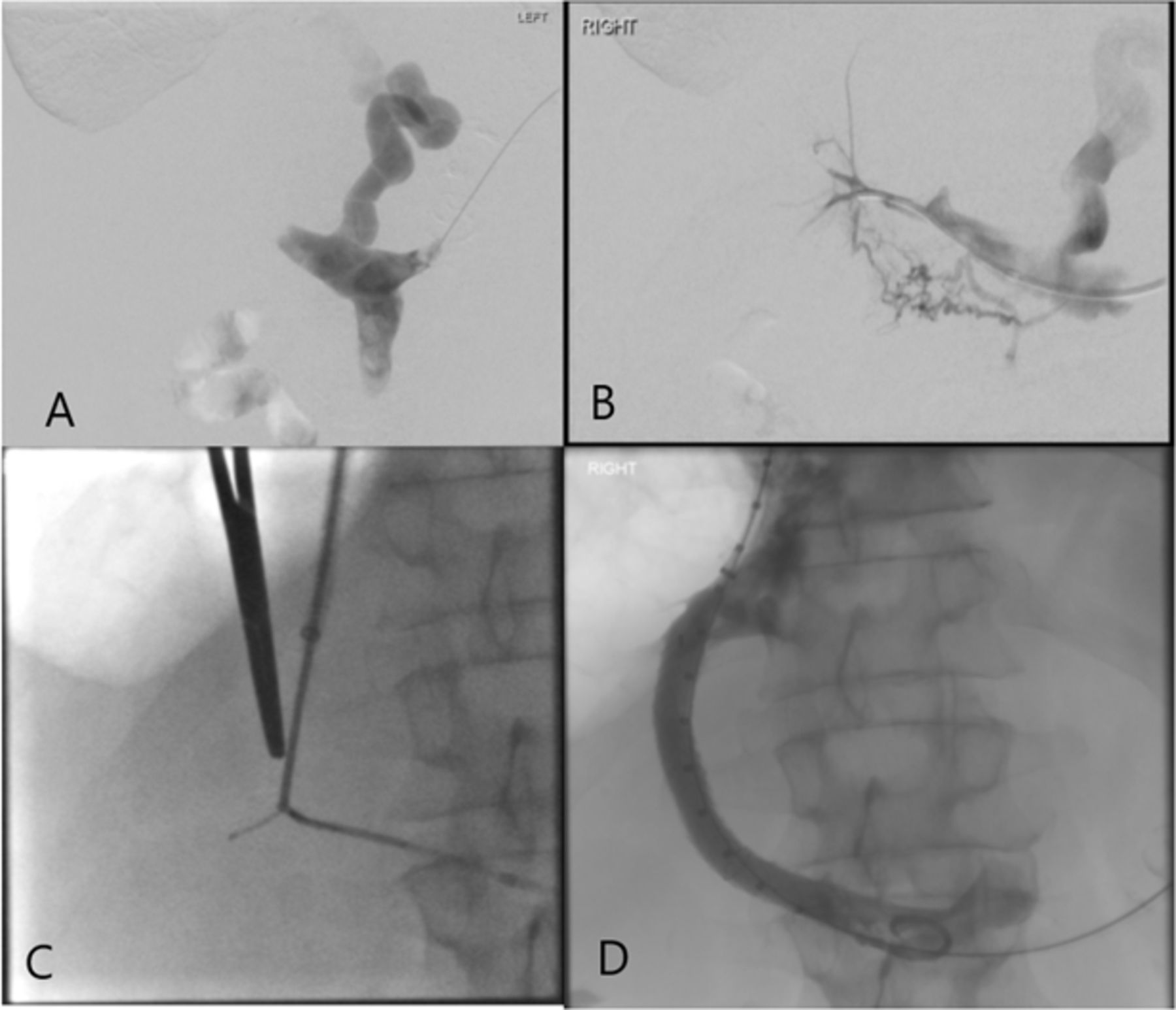
(A) CO2 portography through a catheter wedged within the right hepatic vein. (B) Direct portography through a percutaneous transhepatic catheter, with the tip within the main portal vein. (C) TIPS sheath in place within the right hepatic vein. (D) Transvenous access from the right hepatic vein to the right portal vein obtained by using the percutaneous transhepatic catheter as the angiographic target for the TIPS needle. (E) Balloon dilation of the parenchymal tract. (F) Successful TIPS creation with placement of a Viatorr stent. TIPS, transjugular intrahepatic portosystemic shunt. CO2: Carbon dioxide
A variation of this wire-targeting technique can also be used in the setting of portal vein thrombosis, which is seen in 5%–25% of patients with cirrhosis who are undergoing liver transplant.12 13 In these patients, TIPS placement can be performed in conjunction with thrombectomy to restore flow within the portal venous system. This variation employs the traditional hepatic venous access via the internal jugular vein as discussed above, but instead of percutaneous transhepatic access of the portal vein obtained under ultrasound guidance, percutaneous transsplenic access of the splenic vein is pursued. Once splenic vein access has been obtained, contrast is injected while retracting the access sheath (with guidewire in place to secure access) in order to ensure that a splenic artery or a splenic vein branch was not traversed within the percutaneous route. After appropriate splenic venous access has been confirmed, a 5 or 6 French sheath is placed over the guidewire. Next, a 0.035-inch angled Glidewire and a 5 French Kumpe catheter are advanced through the thrombosed portal venous system. Once recanalisation has been performed successfully, the Kumpe catheter and Glidewire are exchanged for a vascular snare. This snare is used as a target for the TIPS needle, which is advanced from the selected hepatic venous branch toward the thrombosed portal venous system. A guidewire is then negotiated through the TIPS needle and snared through the percutaneous transsplenic sheath. After through-and-through access between the internal jugular vein and splenic vein through the thrombosed portion of the portal venous system has been gained, thrombectomy and venoplasty are performed at the site of occlusion. The parenchymal tract is then dilated, and a TIPS stent is placed once inflow from the portal venous system has been established (figures 4–6). Once portal venous flow has been restored through the recanalised portion of the portal venous system and TIPS stent into the hepatic venous system, the sheath in the internal jugular vein is removed, and haemostasis is obtained by applying direct pressure to the venous access site. For the percutaneous transsplenic access site, we typically perform closure by deploying through the sheath a combination of detachable plugs, pushable coils and Gelfoam slurry using the sandwich technique.
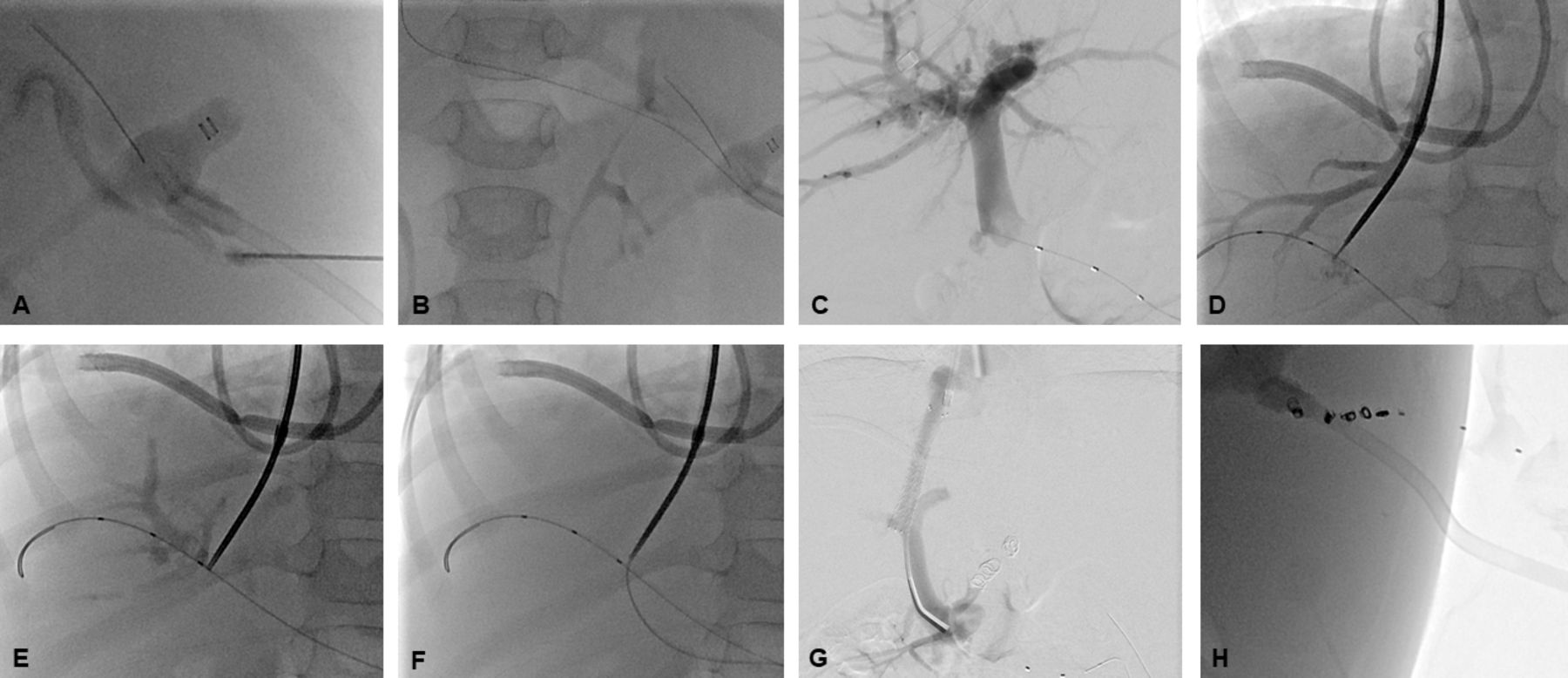
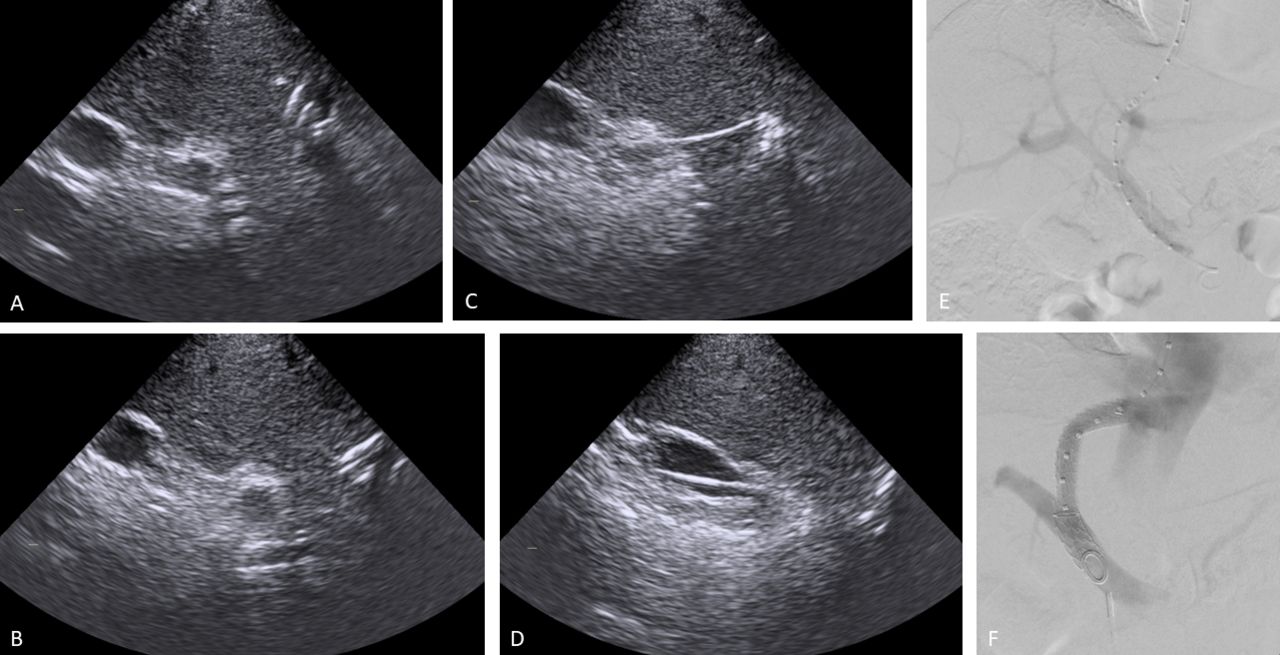
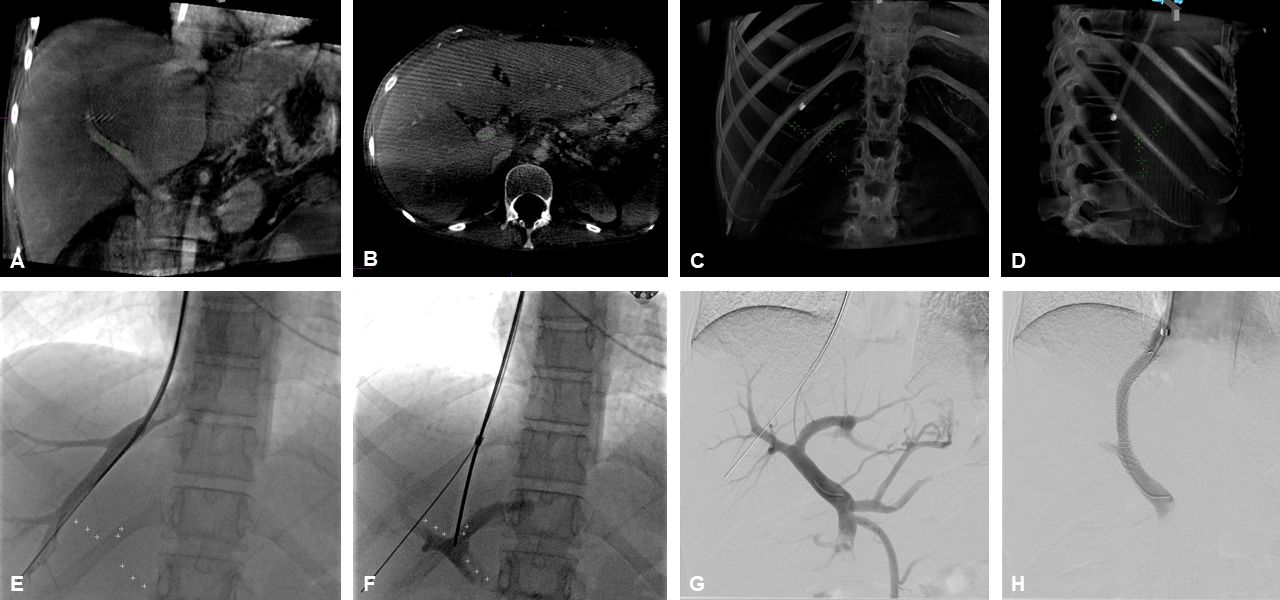
(A) Young child who was born prematurely presented with liver failure and sequelae of portal hypertension including splenomegaly, as well as oesophageal varices complicated by variceal bleeding episodes requiring banding. (A) Ultrasound-guided puncture of the splenic vein was performed using a 22-gauge Chiba needle. (B) A target catheter was inserted through the transsplenic access. (C) Consecutive angiographic visualisation of the portal venous system. (D) The third radiopaque marker of the target catheter was positioned at the portal bifurcation. (E) The TIPS needle was advanced toward the radiopaque catheter (wire/catheter-targeting technique), and access was obtained into the right portal vein. (F) A guidewire was advanced through the TIPS needle/sheath into the portal venous system, and the TIPS tract was dilated with a 4 mm compliant balloon. (G) After dilatation of the TIPS tract, a balloon-expandable stent was placed, followed by coaxial insertion of a self-expandable stent. (H) The percutaneous transsplenic tract was embolised with a total of four microcoils.
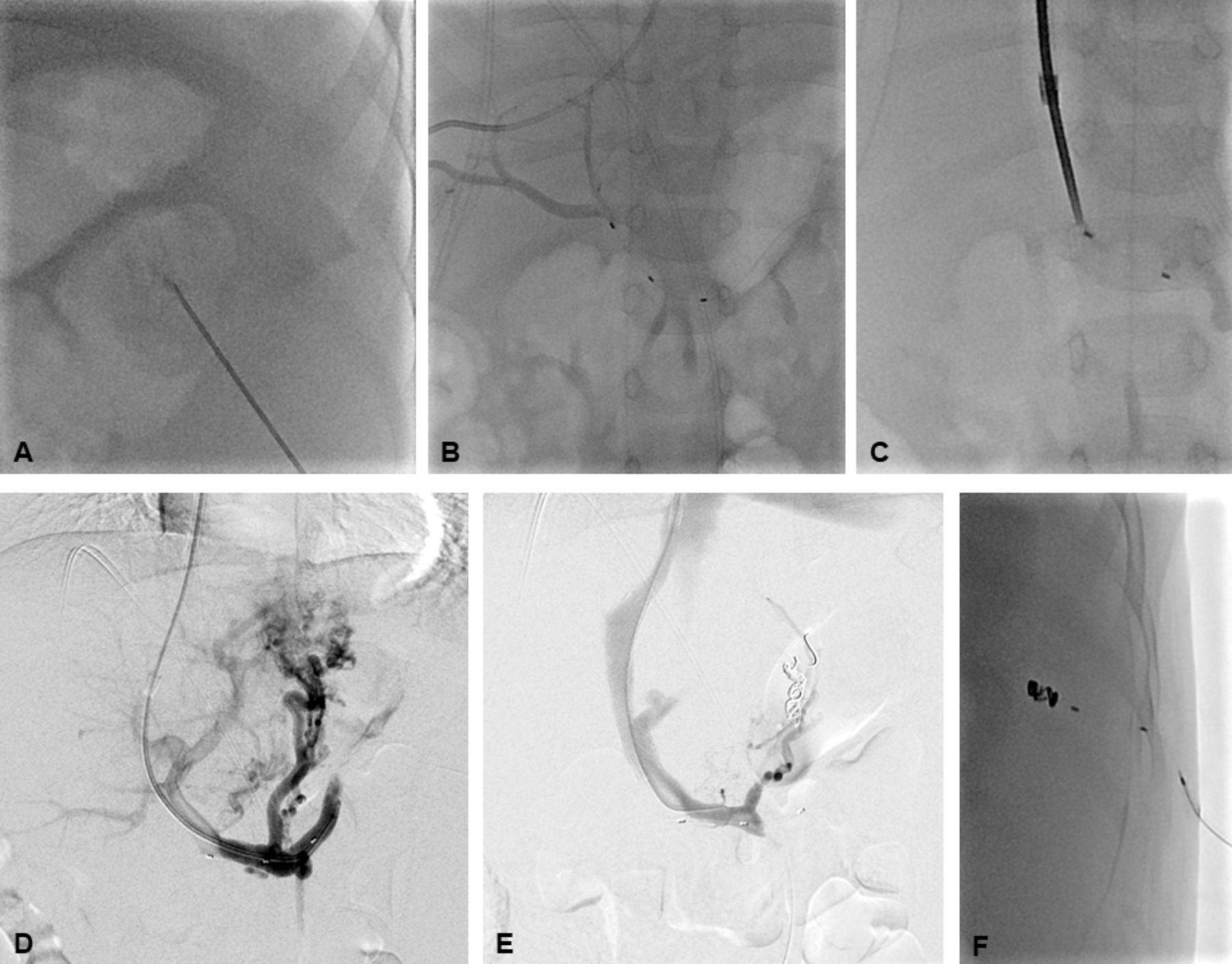
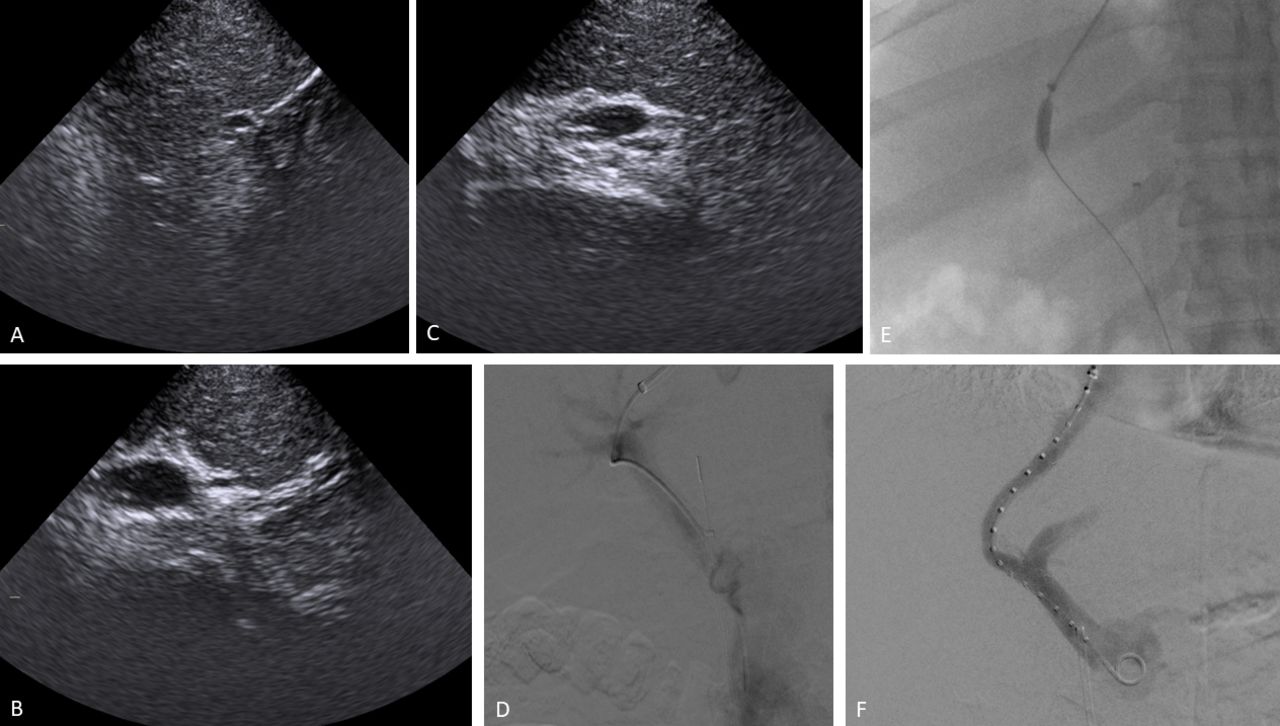
(A) Young child presented with liver cirrhosis secondary to sclerosing cholangitis leading to acute liver failure. (A) An ultrasound-guided puncture of an intraparenchymal branch of the splenic vein was performed. (B) A target catheter was inserted through the splenic vein access site into the portal vein. Injection through the catheter demonstrated the right-sided portal venous system. note that the first radiopaque marker of the catheter was located within the right portal vein. (C) The TIPS needle was advanced, targeting this first radiopaque marker of the catheter. (D) Access was obtained with the TIPS needle in the right portal vein and the catheter was advanced into the portal venous system. The varices were also visualised. (E) A self-expanding stent was placed, and the varices were embolised with detachable coils. (F) The percutaneous transsplenic tract was embolised with microcoils.
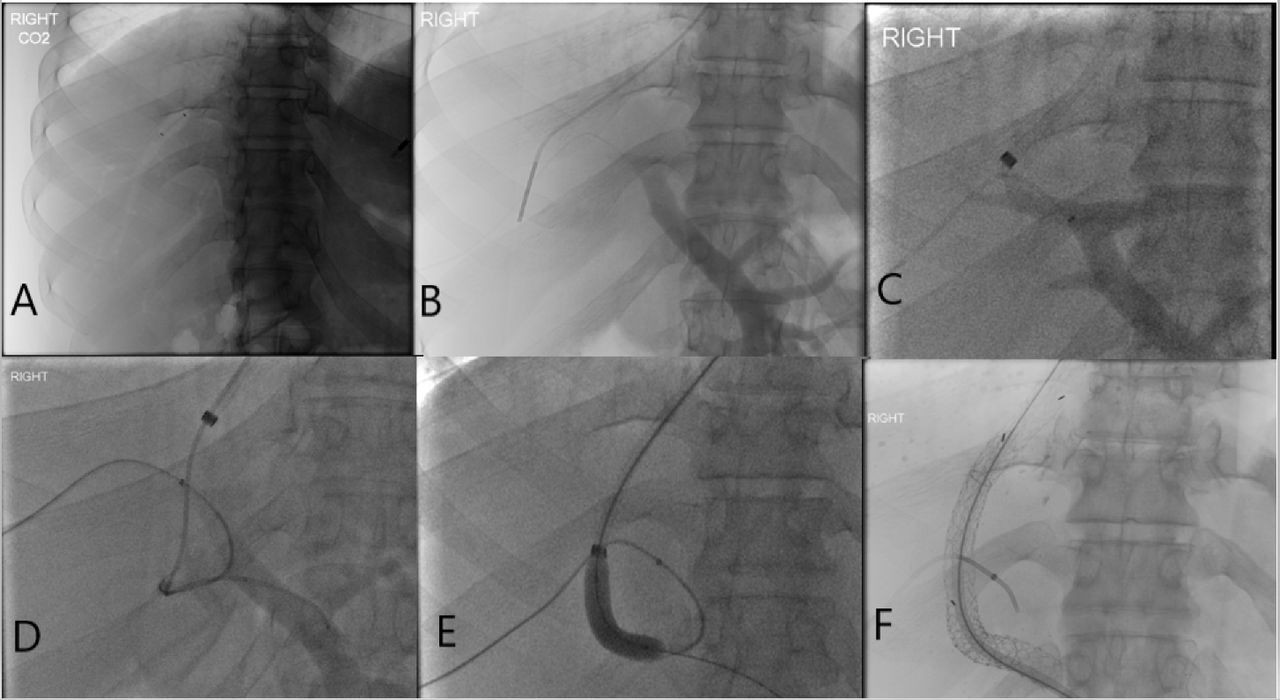
(A) Percutaneous transsplenic access was obtained under ultrasound guidance. A splenic venogram demonstrated antegrade flow in the splenic vein with complete occlusion of the midportion of the main portal vein and a large left gastric varix. (B) A 5 French Kumpe catheter and a Glidewire were used to recanalise the portal vein. (C) A vascular snare was placed via the percutaneous transsplenic access into the right portal vein, with the snare used as a target for transvenous TIPS access from the right hepatic vein into the right portal vein. (D) A TIPS stent was placed extending from the right hepatic vein to the now-patent right portal vein which underwent mechanical thrombectomy. TIPS, transjugular intrahepatic portosystemic shunt.
CBCT-guided access
CBCT uses a conical distribution of beams to provide a 3D volumetric dataset with one spin of the C-arm.14 15 The integration of CBCT into the angiography suite is opening novel avenues to pursue complex procedures requiring fluoroscopy and CT guidance. The first documented use of this technology in the interventional arena was related to neurologic procedures, where it enabled clinicians to rule out intracranial haemorrhage in the procedure suite.16 CBCT can also be used to assist with procedures involving portal venous access, embolisation, thrombolysis, percutaneous ablation and percutaneous drain placement/upsize, all with the potential to decrease radiation dose to the operator.17 18
For the TIPS placement procedure, CBCT is performed once the hepatic vein has been accessed with a catheter and guidewire and/or a TIPS sheath. Alternatively, CBCT can be performed at the beginning of the procedure just before the internal jugular vein is accessed. If ascites is present, paracentesis should be performed prior to CBCT in order to avoid fluid shifts causing substantial movement of the liver and thus leading to unreliable localisation of the portal venous system via CBCT.
CBCT is conducted during an inspiratory breath hold, regardless of whether contrast enhancement is used. Many contrast injection techniques have been described, including indirect portography through the hepatic vein access performed by wedging an end-hole catheter or using an occlusive balloon, followed by injection of iodinated contrast. One study described a technique in which a 6 French coaxial 10 mm balloon (Fogarty type balloon on catheter) was inflated at low pressure in the right hepatic vein.19 Occlusion was verified with a small injection, followed by administration of 40 mL of Iomeron 350 through the lumen of the balloon at a rate of 4 mL/s. CBCT imaging performed after a delay of 8 s provided excellent visualisation of the portal venous system.
An alternate approach is to fuse a non-contrast intraprocedural CBCT study with a preprocedural contrast-enhanced cross-sectional imaging study, typically a contrast-enhanced triple-phase liver CT study (although contrast-enhanced MRI can also be used). With this approach, the portal venous phase of the preprocedural contrast-enhanced imaging study is uploaded to the 3D workstation before the intervention, and subsequent coregistration with the intra-procedural CBCT is performed. Of note, this method is vulnerable to mismatch due to respiratory motion artefacts and variability in the liver location, particularly in patients with cirrhosis who have recurrent ascites and/or recurrent hydrothorax of variable amounts. In a study of 18 patients using this technique, 8 mismatches (44%) were reported; these mismatches were attributed to multiple factors, namely patients’ arm positions, ascites and respiratory motion.20 Some of these factors can be controlled, such as ensuring that all imaging studies are performed with the patient’s arm in the same position. However, control of disease-related factors such as ascites and hydrothorax is limited. In these cases, preprocedural paracentesis or thoracentesis should be performed prior to acquiring the imaging study as discussed above to minimise the mistmatch.
Once intraprocedural CBCT is performed, the images can be coregistered to the preprocedural contrast-enhanced imaging study. Coregistration is based on anatomical landmarks (eg, portal bifurcation or thoracic vertebral bodies) to ensure that there is no substantial mismatch. This step of image fusion can be skipped when contrast-enhanced CBCT is used. In either case, the hepatic vein catheter position should be confirmed and its position relative to the portal venous system should be evaluated on CBCT. At this stage, one of the major advantages of CBCT is the ability to reformat the image set into different projections and slice thicknesses to aid in visualising the planned trajectory, thereby avoiding traversal of critical structures along the trajectory path. A 3D virtual puncture path is then calculated and displayed along with the portal venous system directly onto the 2D fluoroscopic display, producing a form of 3D hybrid live angiography (figure 7). The puncture with the TIPS needle from the hepatic venous system toward the portal venous system is then conducted following this virtual path. Of note, it is beneficial to use more than one orthogonal viewing angle to confirm that the TIPS needle is properly aligned with the target and moves along the planned trajectory path.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Young patient presented with shock and acute liver failure with markedly elevated portal pressures. Percutaneous access was obtained via the right internal jugular vein under ultrasound guidance, and the right hepatic vein was accessed using a 6 French catheter. A total of 60 mL of diluted iodine-containing contrast agent (5:1) was injected at a rate of 4 mL/s to perform CBCT. 3D volume reconstructions and 3D stacks (volume-rendering technique) were automatically generated on a dedicated workstation. (A) Coronal reconstruction with roadmap. (B) Axial reconstruction with roadmap. (C) Coronal 3D roadmap. (D) Sagittal 3D roadmap. (E) The 3D roadmap is fused with the working fluoroscopy screen. (F, G) Under CBCT 3D roadmap guidance, the right portal branch is punctured with the TIPS needle, and access is obtained into the portal venous system as confirmed with injection through a 5 French catheter. (H) The TIPS tract was predilated using an 8 mm compliant balloon, and the TIPS stent was placed. The final angiographic image demonstrated a widely patent TIPS stent with brisk flow of contrast. 3D; three dimensions; CBCT, cone-beam CT.
Discussion
TIPS placement remains one of the more technically challenging interventional procedures owing to the essentially blind, double-oblique puncture from the hepatic venous system to the portal venous system. Operator experience therefore has a significant effect on procedure time, procedure safety and radiation dose.21 Although experienced operators can achieve good procedure metrics using the traditional fluoroscopic approach (wedged CO2 portography), advanced guided portal access techniques such as ICE guidance, wire-targeting technique, and CBCT-derived 3D roadmaps offer several advantages and are gaining increasing popularity.
In the initial human study of ICE-guided portal access, all 25 ICE-guided TIPS placements were technically successful.22 However, when compared with the traditional TIPS approach, ICE-guided access provided no significant reduction in the number of needle passes (4 vs 5; p=0.47) or total fluoroscopy time (30.6 min vs 30 min; p=0.80). Despite these findings, the authors found that ICE-guided portal venous access was beneficial in managing complicated portal venous access situations. For example, ICE guidance was used to avoid puncturing through an existing tumour, to navigate portal thrombotic disease, and to mitigate distorted Budd-Chiari anatomy.
A recent retrospective study comparing ICE-guided access to traditional fluoroscopic-guided TIPS placement found that ICE-guided TIPS access was associated with a significantly lower number of needle passes (2 vs 6), decreased radiation dose (174 mGy vs 981 mGy), and shorter procedure times (86 min vs 125 min) (p<0.01 for all).23 In addition, the use of ICE-guided portal access eliminated extreme outlier cases. For example, there were two traditional fluoroscopic TIPS cases in which 30 and 35 needle passes were required to gain portal venous access, whereas the maximum number of needle passes required for ICE-guided cases was 12. Similarly, one traditional fluoroscopic TIPS case took 360 min to complete, compared with a maximum procedure time of 188 min for ICE-guided TIPS creation. Although the authors did not report the number of perioperative complications, these outlier cases are likely to be associated with an increased risk of such complications.
In another comparison of ICE-guided access and traditional TIPS techniques, the fluoroscopy time (27 min vs 45 min; p=0.003), radiation dose (850 mGy vs 1442 mGy; p=0.01), and total procedure time (124 min vs 161 min; p=0.02) were significantly lower for the ICE-guided cases compared with the traditional fluoroscopic cases.24 In another study, the incidence of capsule perforation (9% vs 34%) and the radiation dose (1592 mGy vs 1816 mGy) were significantly lower in the ICE-guided group than in the traditional fluoroscopic group (p=0.004 for both).25 In this study, the mean time to achieve portal venous access was significantly shorter in the ICE-guided group than in the traditional fluoroscopic group for inexperienced operators (28 min vs 48 min; p=0.01), whereas no significant difference was observed for experienced operators (34 min vs 44 min; p=0.89). Another study similarly found that the radiation dose was significantly lower in the ICE-guided group than in the traditional fluoroscopic group (457 mGy vs 875 mGy; p=0.039).26 However, no significant differences were seen in procedure time (84 min vs 81.5 min; p=0.8281), incidence of capsular perforation (16.7% vs 20%; p=0.7055), or time to accomplish portal venous access (53.5 min vs 62.7 min; p=0.4237). Of note, the ICE operators in this study were relatively inexperienced when compared with the traditional fluoroscopic operators (4.2 y vs 11 y; p=0.0004).
In general, ICE-guided TIPS creation is associated with decreased radiation exposure, shorter procedure times, and lower complication rates. Direct visualisation of the needle path is invaluable in the management of complicated cases with distorted anatomy and neoplastic involvement. Further, inexperienced operators using ICE guidance are able to accomplish results similar to those achieved by more experienced operators using traditional fluoroscopic guidance. The obvious disadvantage of this technique is the need for an additional set of equipment and potentially an additional operator to perform the ICE ultrasound. Previous research has suggested that the dual systems can be used by a single operator when obtaining two tandem accesses through the same internal jugular vein.27
In comparison to ICE-guided TIPS placement, fewer data are available regarding CBCT-guided and wire-targeting techniques for TIPS creation. With regard to CBCT-guided TIPS creation, one of the first reported cases was in a patient with polycystic liver disease, a condition that has been considered a relative contraindication for the procedure because of an elevated risk of bleeding.28 More recently, successful CBCT-guided TIPS creation was reported in 20 prospectively registered patients.29 A recent study comparing CBCT-guided TIPS placement with traditional fluoroscopic TIPS placement demonstrated no significant differences between the groups in mean procedure time (115 min vs 110 min; p=0.996) or radiation dose (563 Gy.cm2 vs 469 Gy.cm2; p=0.069),30 results similar to those were reported in a separate study (overall procedure time: 66 min vs 78 min; p=0.62; fluoroscopy time: 19 min vs 19 min; p=0.86; total radiation dose: 188 Gy.cm2 vs 134 Gy.cm2; p=0.18).31 Another study found that total procedure time and time to puncture were similar between groups, but the CBCT-guided cohort demonstrated a significantly shorter fluoroscopic time than the traditional fluoroscopic group (29 min vs 42 min; p=0.023).19 Other research demonstrated no significant difference in total procedure time or radiation dose between CBCT-guided access and traditional fluoroscopic TIPS placement, but the mean number of needle passes was significantly lower in the CBCT group (2 vs 3.7; p=0.021).32
One of the limitations of CBCT is the misregistration artefact secondary to patient motion, respiratory motion and liver rotation. Therefore, the time period between acquiring the CBCT and portal venous puncture with the TIPS needle should be as short as possible. CBCT guidance also requires additional administration of intravascular nephrotoxic contrast agent, which can be problematic in patients with hepatorenal syndrome. Additionally, CBCT-guided TIPS placement requires the same level of radiation as traditional fluoroscopic TIPS placement. However, CBCT-guided access does not require additional equipment, an additional operator, or an additional venous puncture site. Finally, CBCT may be superior to CO2 portography in identifying portal vein entry sites and anatomical details.33
The wire-targeting access technique has been reported in the literature since the early 1990s.34 In a recent study comparing wire-targeting portal access with traditional fluoroscopic TIPS placement, the technical success rate was comparable between the two groups (92% vs 94%; p>0.99).24 In addition, there was no significant difference in fluoroscopy time (39 min vs 45 min; p=0.55), radiation dose (1421 mGy vs 1442 mGy; p=0.2), contrast volume (194 mL vs 212 mL; p=0.72) or total procedure time (140 min vs 161 min; p=0.18). In contrast, in a more recent study, the wire-targeting access technique was associated with significantly reduced fluoroscopy time when compared with the traditional CO2 portography based technique (29.5 min vs 38.9 min; p=0.005).35 In addition, wire-targeting access required fewer needle passes (2 vs 4; p=0.039).
In general, the wire-targeting access technique requires an additional percutaneous puncture site through a highly vascular organ, risking injury to hepatic artery and biliary system. However, this risk can be minimised by using small-bore needles for percutaneous access (21- or 22-gauge Chiba needles) and 0.018-inch platinum microwires. In comparison to CBCT guidance, the wire-targeting technique offers real-time navigation vs the relatively static CBCT-derived 3D roadmaps. No expensive equipment is required for either of these two techniques.
Few studies have directly compared the different portal venous access methods for TIPS creation. One study compared the wire-targeting technique with ICE-guided TIPS placement and found that the radiation dose (850 mGy vs 1421 mGy; p=0.4) and total procedure time (124 min vs 140 min; p=0.16) were comparable between the techniques. However, the fluoroscopy time was significantly decreased in the ICE-guided group (27 min vs 39 min; p=0.01).24 In practice, the choice of advanced portal venous access technique for TIPS creation is often dictated by available resources and local expertise.
Conclusion
TIPS placement, although an effective method for managing the sequelae of portal hypertension, is one of the more technically challenging interventional procedures. With the traditional fluoroscopic TIPS technique, the needle puncture from the hepatic vein into the portal venous system is performed essentially blindly based on wedged CO2 portography, and inexperienced operators often require a large number of needle passes for successful cannulation. Therefore, advanced guided portal access techniques, specifically ICE guidance, wire-targeting technique, and CBCT-derived 3D roadmaps, are gaining increasing popularity. These advanced portal venous access techniques are advantageous over the traditional CO2 portography-based TIPS placement techniques, with research suggesting that the number of needle passes is generally decreased when these advanced access techniques are used, potentially leading to a reduction in perioperative TIPS placement complication rates. Particularly less experienced operators seem to benefit from these advanced portal access navigation techniques. Prospective studies are required to better evaluate and directly compare the various advanced portal venous access techniques for TIPS creation.
Data availability statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
Acknowledgments
We wish to thank Kerry Hawkins and Megan Griffiths for their administrative and organisational support.
References
Footnotes
Contributors SP, XL, OS, BR, CR, GG, SG, DS, DT, GD, AL, BK contributed equally to the idealization, and editing of the manuscript. SP, XL, OS, and BR contributed equally to the drafting of the manuscript. SP is the guarantor of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.