Article Text

Abstract
Background The effectiveness of early cholecystectomy for gallstone diseases treatment is uncertain compared with conservative management/delayed cholecystectomy.
Aims To synthesise treatment outcomes of early cholecystectomy versus conservative management/delayed cholecystectomy in terms of its safety and effectiveness.
Design We systematically searched randomised control trials investigating the effectiveness of early cholecystectomy compared with conservative management/delayed cholecystectomy. We pooled the risk ratios with a 95% CI, also estimated adjusted number needed to treat to harm.
Results Of the 40 included studies for systematic review, 39 studies with 4483 patients are included in meta-analysis. Among the risk ratios of gallstone complications, pain (0.38, 0.20 to 0.74), cholangitis (0.52, 0.28 to 0.97) and total biliary complications (0.33, 0.20 to 0.55) are significantly lower with early cholecystectomy. Adjusted number needed to treat to harm of early cholecystectomy compared with conservative management/delayed cholecystectomy are, for pain 12.5 (8.3 to 33.3), biliary pancreatitis >1000 (50–100), common bile duct stones 100 (33.3 to 100), cholangitis (100 (25–100), total biliary complications 5.9 (4.3 to 9.1) and mortality >1000 (100 to100 000).
Conclusions Early cholecystectomy may result in fewer biliary complications and a reduction in reported abdominal pain than conservative management.
PROSPERO registration number 2020 CRD42020192612.
- meta-analysis
- gallstone disease
- cholecystectomy
Data availability statement
No data are available. All the data is available in the online supplementary material.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known about this subject?
Although from individual trials, early cholecystectomy is considered safe and effective compared with conservative management/delayed cholecystectomy, but the synthesised evidence is limited.
What are the new findings?
Gallstone-related complications are significantly lower with early cholecystectomy compared with observation management, endoscopic management and delayed cholecystectomy.
The perioperative and intraoperative complications are significantly higher with early cholecystectomy compared with delayed cholecystectomy.
Overall early cholecystectomy is effective compared with conservative management/delayed cholecystectomy for gallstones.
How might it impact clinical practice in the foreseeable future?
Our meta-analysis has reported both adjusted and unadjusted number needed to treat to harm, which is a beneficial measure for the surgeons and policymakers to arrive at appropriate clinical and policy decision-making, respectively.
Introduction
Cholelithiasis/gallstone disease management imposes a significant burden on healthcare systems worldwide, costing about 6.5 billion dollars/year only in the USA itself.1 The prevalence of gallstones ranges from 0.1% to 50.5% worldwide2. Although gallstone disease is usually asymptomatic, certain risk factors drive the progression from asymptomatic to symptomatic illness, with or without complications, making it imperative to treat.3 Gallstone-related complications include common bile duct stones (CBD stones)/choledocholithiasis, acute cholecystitis, cholangitis, gallstone pancreatitis and others.3 Surgical removal of the gallbladder (known as cholecystectomy) is the treatment of choice for symptomatic gallstones.4 Laparoscopic cholecystectomy is the preferred treatment option over open cholecystectomy for gallstones and cholecystitis.5 However, approximately 12% of patients who have undergone cholecystectomy continue to experience pain and recurrent gallstone-related symptoms.6
Conservative management (CM), involving pain and symptomatic treatment with gallbladder in situ, carries no risk of operative complications and is also considered an alternative to cholecystectomy.7 However, among conservatively managed patients with uncomplicated gallstones, recurrence of gallstone symptoms and subsequent development of gallstone-related complications often lead to cholecystectomy.8 Similarly, several randomised control trials (RCTs) comparing early versus delayed cholecystectomy (DC) for gallstone disease reported recurrence of symptoms/complications in the waiting period before surgery and also reported higher postsurgical complications with delayed surgery.9 Thus, the effectiveness of early cholecystectomy (EC) over CM/DC is ambiguous. Therefore, we aimed to conduct this systematic review and meta-analysis to synthesise treatment outcomes between EC and CM/DC. The study’s objective is to synthesise treatment outcomes such as (1) gallstone-related complications between EC and CM/DC (2) surgical complications, length of hospital stays and operative time between early and DC.
Methods
Screening and study selection
We carried out this systematic review and meta-analysis in compliance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and registered the protocol at PROSPERO.10 11 We systematically searched the studies indexed in PubMed-Medline, Scopus and Embase. The search terms were constructed based on domains of population, intervention, comparator and outcome (PICO) as described below. The search terms were combined using Boolean operator ‘OR’ within the same domains, and Boolean operator ‘AND’ between domains of PICO as described in online supplemental tables 1–3. An initial search was performed on 16 June 2020 and an updated search was performed on 12 January 2021.
Supplemental material
According to the inclusion criteria, search results were screened for eligibility. The population included individuals with gallstones (cholelithiasis/cholecystolithiasis) or CBD stones (choledocholithiasis) or acute cholecystitis or gallstone pancreatitis. The intervention included surgical removal of the gallbladder through open or laparoscopic methods, where surgery was performed on an emergency basis or within 7 days, treated as EC. The comparator is CM and DC. CM included both observation management (OM) (also known as wait and watch strategy) and Endoscopic management (EM). Under OM, this study considered patients with gallstones who were symptomatically managed using pain killer, antibiotics, diet and lifestyle changes. Under EM, this study considered patients who underwent endoscopic removal of CBD stones with gallbladder left in situ. In DC, we considered patients who were initially managed conservatively and later underwent cholecystectomy after 6 weeks. Outcomes included complications related to gallstone disease, perioperative, intraoperative and postoperative complications with cholecystectomy, length of hospital stays, operative time and the studies included were RCTs. Nonrandomised trials, observational studies, reviews and studies published in non-English languages for which a translation could not be obtained were excluded. Studies were also excluded for their selection of PICO, that is not of study’s interest.
Titles and abstracts of studies listed from the electronic database search were meticulously screened independently by authors (BSB, MH, AS) using Rayyan-web application.12 After screening, authors independently reviewed and selected studies based on inclusion and exclusion criteria with authors’ mutual consensus (figure 1).
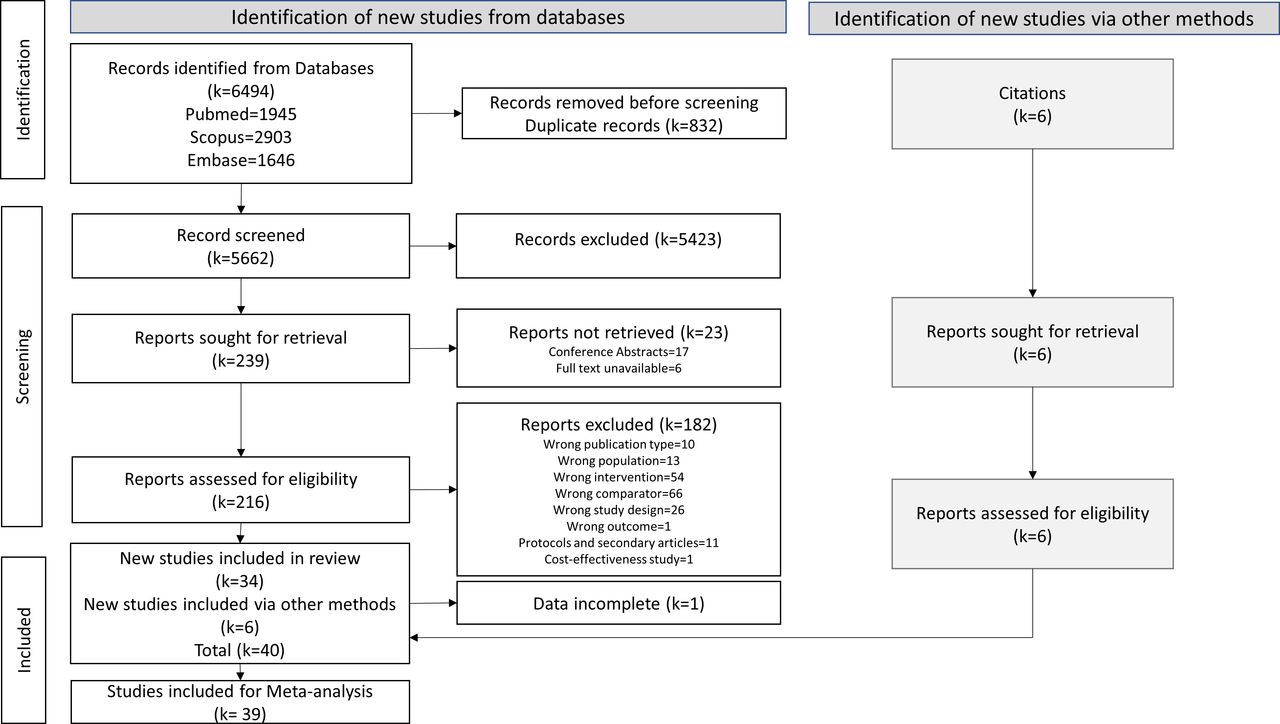
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flowchart of study selection.
Data extraction and management
All relevant details were extracted from the studies included, using a specific data extraction form. Data extracted include study characteristics (study design, location of study etc), participant characteristics (age, gender, duration of symptoms and timing of surgery), intervention, comparators and treatment outcomes (gallstone symptoms and complications, surgical complications). All the data for pooling were extracted as reported in the primary studies. For quality control, data extraction was performed by one reviewer and cross checked by another reviewer (BSB, MH). Any discrepancies between authors were resolved by discussion and consulting with a third reviewer (AS), whenever necessary. The extracted data were checked and used for further analysis after confirmation of its consistency.
Assessment of risk of bias
We assessed the risk of bias using a revised Cochrane risk of bias tool (RoB-2 tool) for randomised trial.13 RoB-2 tool comprises five domains: bias arising from randomisation process, deviation from intended intervention, missing outcome data, bias in the measurement of outcome and selection of reported results. The judgement regarding the risk of bias was determined by means of signalling questions with responses as ‘yes’, ‘probably yes,’ ‘probably no,’ ‘no’ and ‘no information’. Two authors (MH and KVJ) independently assessed the risk of bias; later, a consensus was reached for any disagreement through discussion. However, a third reviewer’s opinion (BSB) was obtained wherever necessary. The overall risk of bias was ascertained as high, some concerns or low for each study.
Statistical analysis
Risk ratio along with its 95% CI was estimated for each complication from individual studies. Subsequently, risk ratios were pooled across studies using a random effects DerSimonian and Laird method considering possible heterogeneity across studies. For continuous variables, such as operation time and duration of hospital stay, mean difference and its 95% CI were estimated for individual studies and then pooled using a random-effects DerSimonian and Laird method. While performing the analysis, zero cells were corrected by adding 0.5.
Assessment of heterogeneity
Heterogeneity was assessed using visual inspection of forest plots, Cochran-Q test and I2 statistics. I2 describes the percentage of the variability in effect estimates that is due to heterogeneity rather than sampling error (chance). I2 values in our analysis were interpreted using the standards laid down in Cochrane’s handbook for Systematic Reviews of Interventions.14 Cochran’s Q is the weighted sum of squared differences between individual study effects and the pooled effect across studies, with the weights being those used in the pooling method. Q is a χ2 statistic with k (number of studies) minus one degree of freedom. If the Q(k-1) value is greater than the tabulated value (obtained using df) and p value is <0.1, then the heterogeneity is considered to be present.15
Analysis of subgroups
Results were further explored using subgroup analysis based on intervention and comparators: EC versus OM (EC vs OM), EC versus EM and EC versus DC. A subgroup analysis of baseline gallstone complications (CBD stones/acute cholecystitis/gallstone pancreatitis) was performed within each comparison to address the hetergeneity of patients included in the systematic review. We also performed a subgroup analysis, to determine whether the timing of surgery influenced the surgical complications. We have also performed a separate analysis of EC with CM alone (combining OM and EM). Risk ratios and mean differences were pooled between all interventions and comparators; however, perioperative and intraoperative complications were pooled only among early versus DC studies.
Estimation of number of needed to harm
In this systematic review and meta-analysis, we additionally estimated the number needed to treat to harm (NNTH) for each outcome.16 NNTH is defined as ‘the number of people exposed to a given treatment such that on average and over a given follow-up period one additional person experiences the adverse effect of interest because of the treatment’. It expresses the additional absolute risk of an adverse effect conferred by treatment and is, therefore, a useful and intuitively understandable decision-making tool for practicing clinicians.16 As there is no consensus for the calculation of NNTs from pooled meta-analysis, we estimated the NNTH for each outcome using the two approaches suggested.17 In the first approach, the log of risk difference (RD) and its 95% CIs between intervention and comparator for each complication was estimated. RDs were then pooled across studies using a random-effect model. Following, mean NNTH for each complication and its 95% CI were calculated as the inverse of mean and inverse of upper and lower limits of 95% CI of pooled RD, respectively.18

We also calculated adjusted NNTH using the method suggested by Furukawa et al19 and recent evidence synthesis.17 We calculated adjusted NNTH using the following formula.

where RR is pooled relative risk, PEER is the patient expected event rate. The PEER was calculated as the ratio of the total frequency of complication among comparators to that of the total number of comparators in respective pooled studies.
Assessment of publication bias
Publication bias was assessed using a funnel plot (asymmetry) and Egger’s test (p<0.05) of the effective measures, only if sufficient (at least 10) number of studies were available for pooling.20 21 Furthermore, on identifying asymmetry in the funnel plot, the source of asymmetry was explored using a contourenhanced funnel plot. Data were recorded using a Microsoft Excel sheet and analysed using Stata software V.1622. Two-sided p<0.05 was considered statistically significant except for the subgroup analysis and heterogeneity test, wherein p<0.10 was regarded as significant.
Results
We retrieved a total of 6494 studies through our initial and updated search, out of which 40 studies were included for systematic review, as shown in the PRISMA flow diagram (figure 1). We had excluded one study from the meta-analysis since no information on complications was reported.23 Therefore, 39 studies with 4483 patients with gallstone disease (intervention—EC, n=2265 and comparator (CM/DC), n=2218) were included in meta-analysis.8 24–61 Characteristics of included studies are provided in online supplemental table 4.
Patient’s mean age was 53.47 years and 54.41 years in intervention and comparators, respectively. Sample sizes in individual studies ranged from 15 to 314 patients. In total, 6, 3 and 31 studies that compared EC versus OM,8 54–58 EC versus EM59–61 and EC versus DC,23–53 respectively, were analysed. Among the 32 studies, which reported gender proportions, 26 studies (81.25%) had a higher proportion of female participants. Only 9 out of 40 included studies for systematic review were multicentric RCTs, and the rest were conducted in single centres. The baseline gallstone complications reported were acute cholecystitis, CBD stones, gallstone pancreatitis and uncomplicated gallstones in 20, 12, 7 and 1 study, respectively. Out of the 40 studies included in systematic review, open cholecystectomy was reported among 9 studies and cholecystectomy was performed laparoscopically among the rest. Duration of symptoms was reported only in seven studies, in which duration varied from 35.1 to 96 hours. In all the included EC versus DC studies, EC was performed within 7 days of randomisation and DC was performed after 6 weeks of randomisation.
Risk of bias assessment
Out of 40 studies included in systematic review, 31 (77.5%) studies adequately followed the randomisation process. None of the included studies reported that patients and caregivers were blinded for the intervention under study, which might be due to the involvement of surgical intervention. Nine (22.5%) studies had shown deviations from the intended intervention. There were seven (17.5%) studies under the missing outcome data domain, one study (2.5%) in each domain for measurement of outcome data and selection of the reported results were assessed as high risk of bias. The overall risk of bias was estimated as low in 22 (55.0%), some concerns in 6 (15.0%) and high in 12 (30.0%) studies (online supplemental figure 1).
Gallstone-related complications
Pain/biliary colic
We pooled the risk ratios of pain/biliary colic from 12 studies comparing EC and CM/DC, consisting of subgroups EC versus OM (n=5),8 54 56–58 EC versus EM (n=2)59 61 and EC versus DC (n=5).27 30 32 41 45 The pooled risk ratio was 0.38 (0.20 to 0.74, I2=51.57%) with moderate heterogeneity indicating significantly lower pain events with EC (see table 1). However, among subgroups, only in EC versus OM, there was significantly lower pain events with EC (0.39, 0.16 to 0.94, I2=39.4%). The adjusted and unadjusted NNTH were 14.0 (10.9 to 33.4) and 12.5 (8.3 to 33.3), respectively. Subgroup analysis was conducted based on baseline gallstone complications within each comparison (EC vs OM, EC vs EM and EC vs DC). In EC versus OM, subgroups included were patient with (1) CBD stones, (2) uncomplicated gallstones and (3). acute cholecystitis. The pooled risk ratio shows significantly lower pain events with EC compared with OM in CBD stones and uncomplicated gallstones, whereas in acute cholecystitis, no significant difference was observed (online supplemental figure 3). In EC versus EM, subgrouping based on baseline gallstone complications was not performed due to lack of published studies. In EC versus DC, one study each for acute cholecystitis30 and CBD stones45 and three studies for gallstone pancreatitis22 27 36 were identified. Significantly lower pain was observed in the EC compared with DC for acute cholecystitis and CBD stones, whereas for gallstone pancreatitis, no significant difference was observed between EC and DC online supplemental figure 3. The funnel plot for EC versus DC shows asymmetry (p=0.508), indicating publication bias (online supplemental figure 4). Separate analysis of pain in EC versus CM alone (combining OM and EM) showed significantly lower pain events in EC (online supplemental table 5).
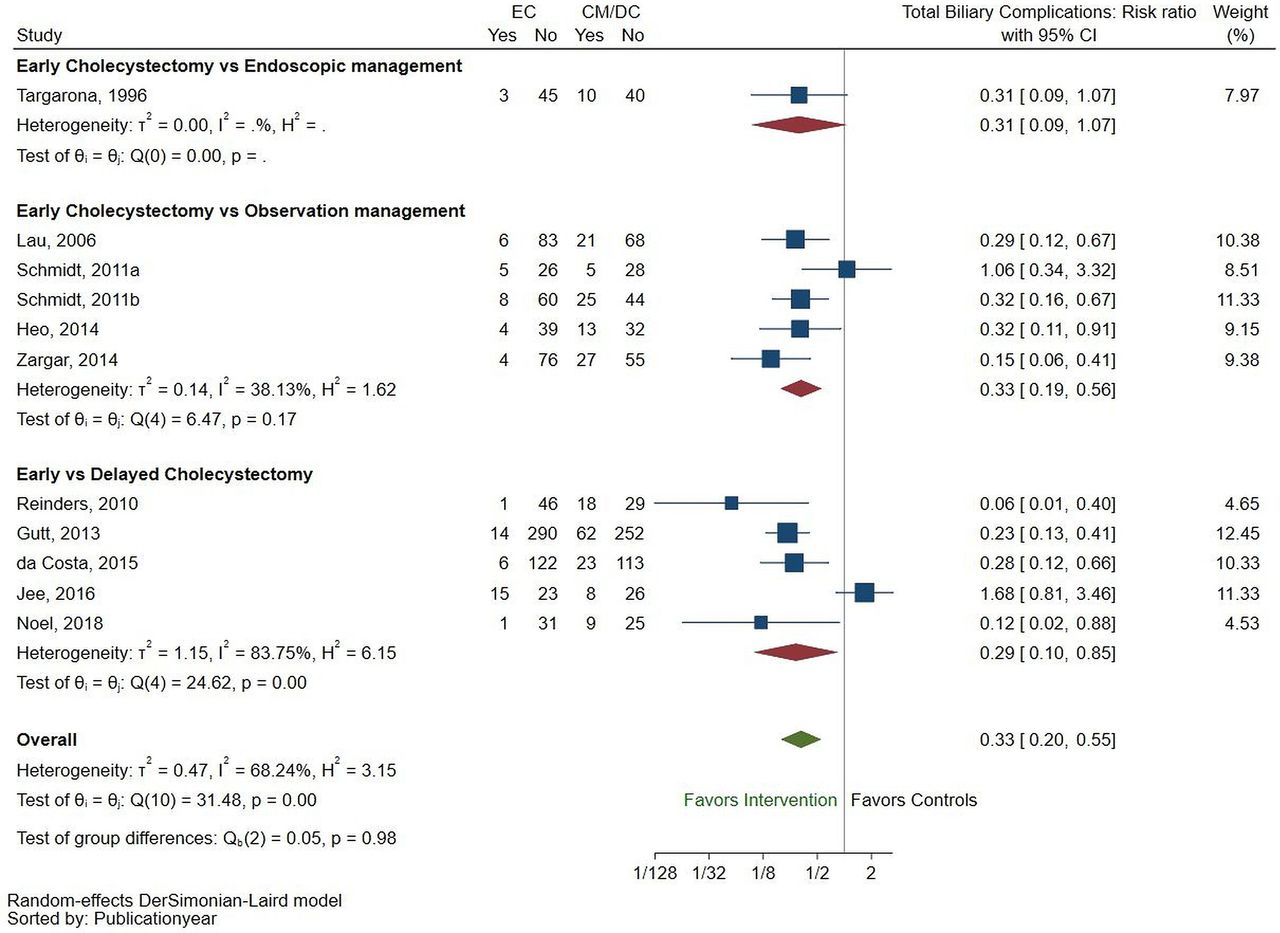
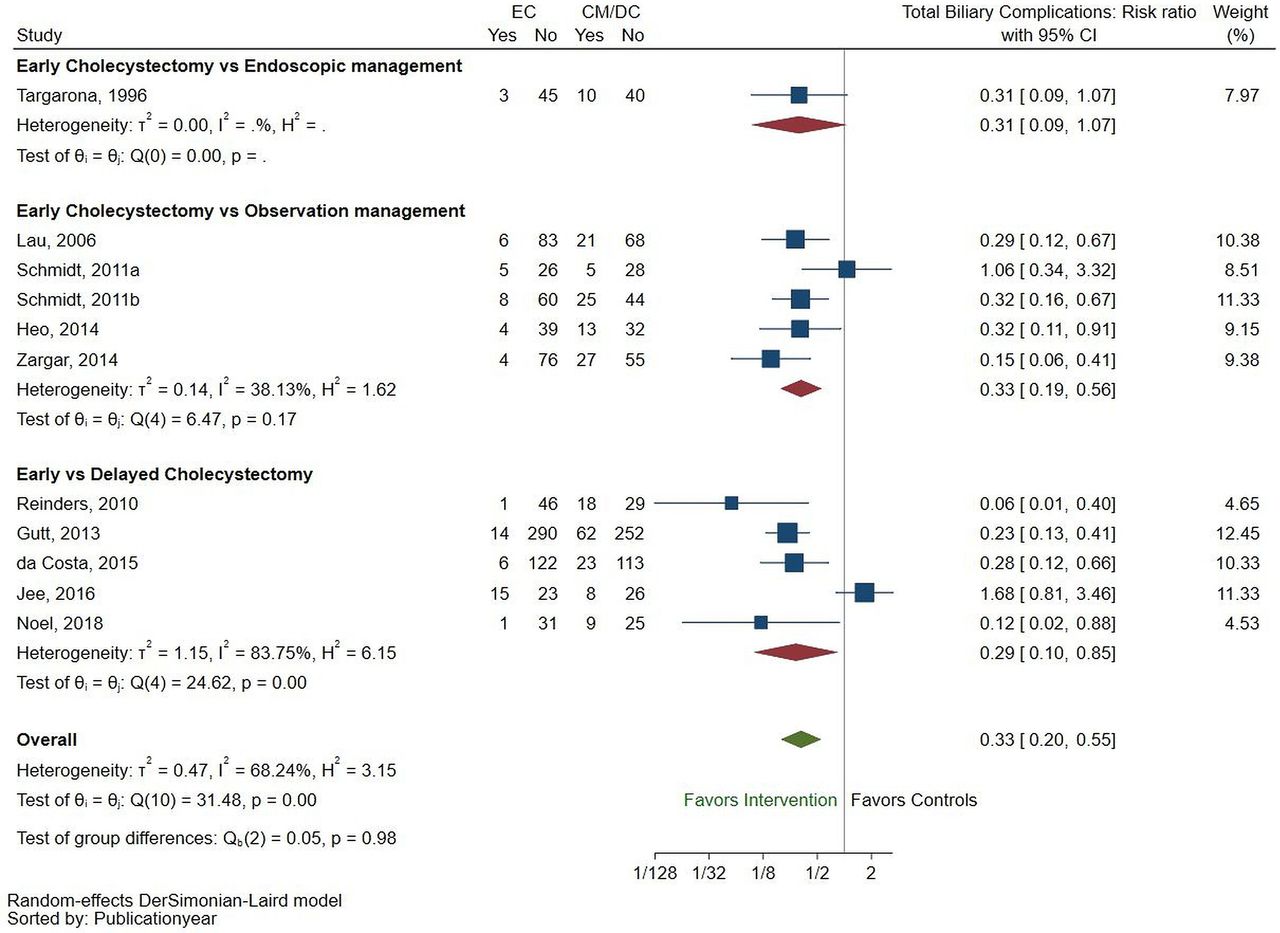
Forest plot showing risk ratio of total biliary complications between early cholecystectomy and conservative management/delayed cholecystectomy with subgroups. CM, conservative management; DC, delayed cholecystectomy; EC, early cholecystectomy.
{kind=link}
{kind=link}
{kind=link}
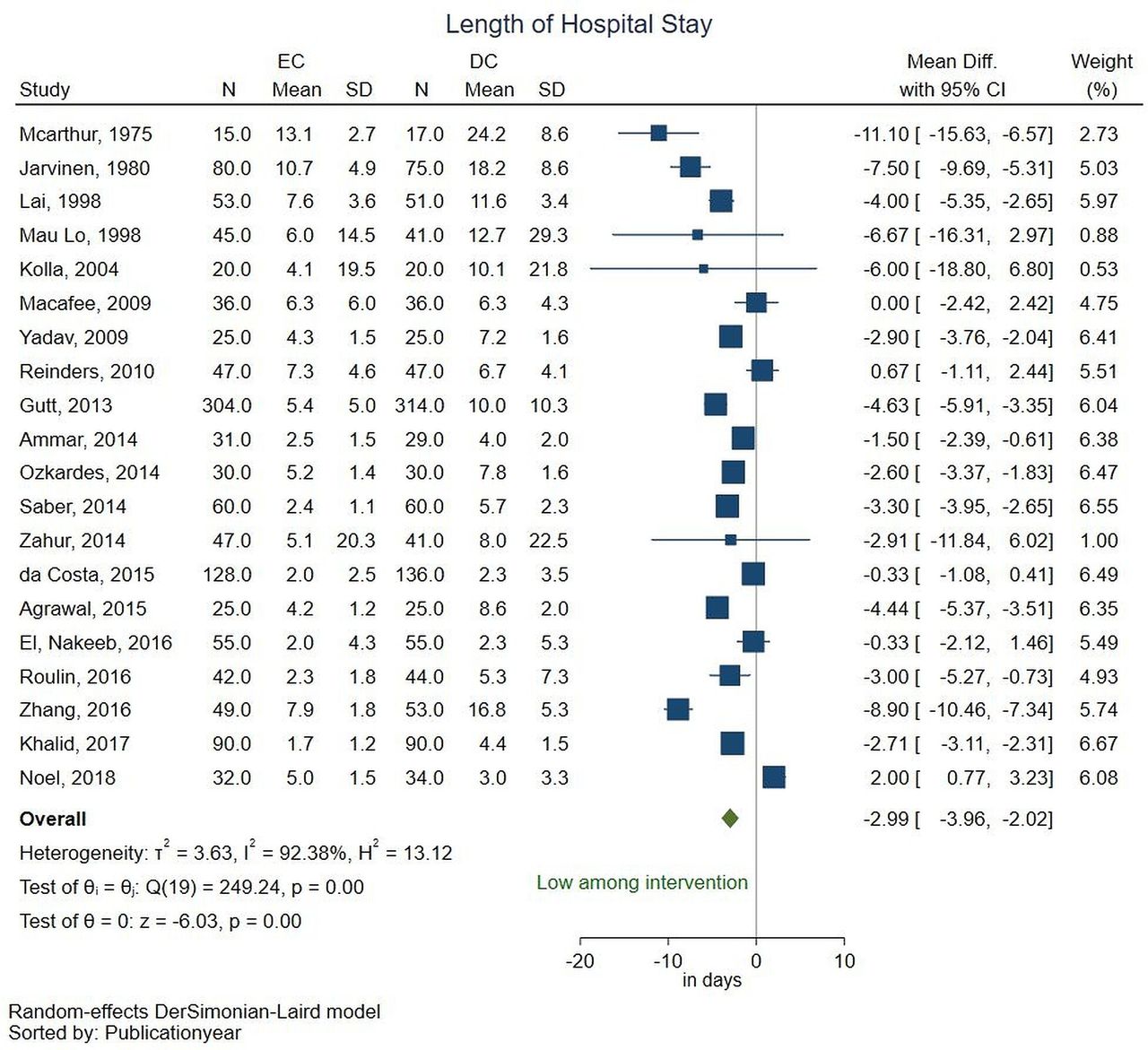
Forest plot showing mean difference in length of hospital stay between early and delayed cholecystectomy. DC, delayed cholecystectomy; EC, early cholecystectomy.
Pooled risk ratios and NNTH of gallstone-related complications with subgroups based on intervention
Biliary pancreatitis
We pooled the risk ratios of biliary pancreatitis from eight studies consisting of subgroups EC versus OM (n=3),8 57 58 EC versus EM (n=2)59 60 and EC versus DC (n=3).27 32 41 The pooled risk ratio was estimated as 0.47 (0.221.03, I2=0%) with low heterogeneity, indicating no significant difference between intervention and comparators (table 1). The adjusted and unadjusted NNTH were 44.9 (30.5 to 793.9) and >1000 (50.0 to 100.0) respectively. Among subgroups, in EC versus DC alone, significantly lower biliary pancreatitis events was observed in EC. Subgroup analysis based on baseline gallstone complications was not performed due to insufficient published literature. Separate analysis of biliary pancreatitis in EC versus CM alone (combining OM and EM) showed no significant difference in biliary pancreatitis between EC and CM (online supplemental table 5).
CBD stones
We pooled the risk ratios of CBD stones from four studies consisting of EC versus OM (n=2)8 57and EC versus DC (n=2).27 45 No studies with EC versus EM were available. The pooled risk ratio was 0.50 (0.14 to 1.78, I2=0%) with low heterogeneity, indicating no significant difference between intervention and comparator. Results were found similar within each of the subgroups (see table 1). The adjusted and unadjusted NNTH were 81.4 (47.3 to 52.2) and 100.0 (33.3 to 100.0), respectively. Subgroup analysis based on baseline gallstone complications was not performed due to insufficient published studies. Separate analysis of CBD stones in EC versus CM alone (combining OM and EM) showed no significant difference in CBD stones between EC and CM (online supplemental table 5).
Cholangitis
We pooled the risk ratios of cholangitis from six studies consisting of EC versus OM (n=4)54–56 58 and EC versus EM (n=2).60 61 No studies with EC versus DC were available, the pooled risk ratio was 0.52 (0.28 to 0.97, I2=0%) with no heterogeneity, indicating significantly lower cholangitis events with intervention (see table 1). The adjusted and unadjusted NNTH were 21.6 (14.4 to 345.7) and 100.0 (25.0 to 100.0), respectively. Among subgroups, in EC versus OM, significantly lower cholangitis events were observed in the EC group (RR=0.46, 0.230.91, I2=0%) (table 1). Subgroup analysis based on baseline gallstone complications was not performed due to insufficient published studies. Separate analysis of cholangitis in EC versus CM alone (combining OM and EM) showed significantly lower cholangitis events in EC (online supplemental table 5).
Total biliary complications
We pooled the risk ratios of total biliary complications from 11 studies, including subgroups EC versus OM (n=5), EC versus EM (n=1) and EC versus DC (n=5) (see table 1). The pooled risk ratio was 0.33 (0.20 to 0.55, I2=68.24%) with moderate heterogeneity indicating significantly lower total biliary complications with EC (figure 2). The adjusted and unadjusted NNTH was 6.3 (5.2 to 9.3) and 5.9 (4.3 to 9.1), respectively. Among the subgroups, in EC versus OM and EC versus DC, there were significantly lower biliary complications with EC, but, not in EC versus EM subgroup. On subgroup analysis based on baseline gallstone complications, EC versus OM showed significantly lower total biliary complications in the EC for CBD stones and cholelithiasis (online supplemental figure 5). In EC versus DC, only one study each for acute cholecystitis30 and CBD stones45 was identified, showing significantly lower total biliary complications in EC than DC. For gallstone pancreatitis, three studies27 32 41 were included, which showed no significant difference between EC and DC (online supplemental figure 6). The funnel plot showed asymmetry (p=0.476), indicating publication bias (online supplemental figure 7). Separate analysis of total biliary complications in EC versus CM alone (combining OM and EM) showed significantly lower total biliary complications in EC (online supplemental table 5).
Mortality
We pooled the risk ratios of mortality from 15 studies, including subgroups EC versus OM (n=4),54 55 57 58 EC versus EM (n=2)60 61 and EC versus DC (n=9)24 27 30 32 34 35 42 45 49 (see table 1). The pooled risk ratio was 0.74 (0.48 to 1.15, I2=0%) with no heterogeneity, showing no significant difference between intervention and comparator. Similar results were found within each of the subgroups. The adjusted and unadjusted NNTH were 118.3 (59.16205.1) and >1000 (100.0->1000), respectively. Furthermore, subgroup analysis based on baseline gallstone complication showed no significant difference in mortality between EC and OM (online supplemental figure 8). Similarly, in EC versus DC, no significant difference in mortality was observed between the subgroups (online supplemental figure 9). The funnel plot showed asymmetry (p=0.553), indicating publication bias (online supplemental figure 10). Separate analysis of mortality in EC versus CM alone (combining OM and EM) showed no significant difference in mortality between EC and CM (online supplemental table 5).
Conversion to laparotomy
We pooled the risk ratios of conversion to laparotomy from 19 studies comparing EC and DC25–29 32 34 36 37 41 43 44 46–48 50–53 (see table 1). The pooled risk ratio was 1.08 (0.18 to 1.43, I2=2.01%) with low heterogeneity showing no significant difference between the intervention and comparator. The adjusted and unadjusted NNTH was >1000 (100.0≥1000). Subgroup analysis based on baseline gallstone complication showed no significant difference between subgroups (online supplemental figure 11). The funnel plot showed asymmetry (p=0.553), indicating publication bias (online supplemental figure 12).
Surgical complications
All surgical complications, including perioperative, intraoperative and postoperative complications, were compared between EC versus DC groups (see table 2). The perioperative and intraoperative complications including a requirement of decompression, use of endoscopic pouches to retrieve specimen, enlargement of sub umbilical incision events were significantly found higher in EC, indicating complexity. In contrast, adhesion events were lower in EC significantly. Other complications such as drain placement, bile leak, CBD injury, bleeding and total operative complications reported in the studies did not differ between EC and DC. On subgroup analysis, based on baseline gallstone complications, the events of perioperative and intraoperative complications did not differ between subgroups (data not shown). Subgroup analysis on the timing of surgery had shown similar results within the subgroups (online supplemental table 6).
Pooled risk ratios and NNTH of surgical complications in early versus delayed cholecystectomy
The postoperative complications included as reported by the studies were wound infection, sepsis, postoperative bleeding, cystic duct leakage, chest infection, pneumonia, retained CBD stones, reoperation due to bile leak, pulmonary embolus, subphrenic abscess and readmission rate. Among the postoperative complications reported, only the readmission rate was significantly lower in the EC group. All other complications had shown no significant difference between EC versus DC groups. Subgroup analysis had also shown similar results between subgroups based on baseline gallstone complications (data not shown) and timing of surgery (online supplemental table 6).
The length of hospital stay was significantly lower in the EC group with a mean difference of −3.00 (−3.99 to −2.02) days with high heterogeneity (I2=92.61%) (figure 3). However, operative time (in minutes) did not differ between EC versus DC groups, with a mean difference of −4.84 (−12.35 to 2.66) with high heterogeneity (I2=90.34%).
Discussion
In this systematic review and meta-analysis of RCTs, we compared clinical effectiveness of EC with CM/DC in terms of reducing recurrence of gallstone symptoms and occurrence of related complications. We also compared the surgical complications between EC and DC. Meta-analysis results showed that the gallstone-related complications, particularly pain/biliary colic, acute cholecystitis and cholangitis, were significantly lower among EC compared with CM/DC. The total biliary complications reported in the studies were significantly lower with EC in the EC versus OM subgroup, whereas no significant difference was observed in the EC versus EM and EC versus DC subgroups. The perioperative and intraoperative complications, including the requirement of decompression, use of endoscopic pouches to retrieve specimen, enlargement of subumbilical incision except for adhesion, were found to be significantly higher in EC, indicating the complexity of the procedure. Other perioperative and major postoperative complications, such as wound infection and bile leak, did not differ between EC versus DC groups.
Previous systematic review and meta-analysis, comparing EC versus DC, had focused mainly on surgical complications, length of hospital stays and operative time with no/less emphasis on gallstone-related complications.9 But, this review mainly focused on recurrent gallstone complications, thereby observing lower effectiveness of CM/DC from the pooled analysis. However, only fewer number of RCTs had reported these outcomes.27 30 32 41 45 We also included few additional studies comparing EC versus DC, which were not included in any previous systematic review and meta-analysis.25 31 33 35 42 52
We also compared surgical outcomes in EC and DC groups to assess the impact of delayed surgery on surgical complications. Although studies involving CM reported surgical outcomes, not all the patients in the conservative arm underwent surgery. Therefore, we considered it appropriate to compare the surgical complications between EC and DC alone. Even though many previously published observational studies reported a higher risk for bile duct injury with EC in acute cholecystitis,62 63this meta-analysis suggests that there is no significant difference in terms of major postoperative complications such as bile duct injury, wound infection and bile leak between EC and DC. Our meta-analysis observed a higher risk for perioperative and intraoperative complications in EC similar to previous systematic review and meta-analysis.9 Although there was no significant difference in major surgical complications, this meta-analysis results revealed the recurrence or aggravation of gallstone symptoms during the waiting period of DC. Thus, EC seems to be a safer option based on existing pieces of evidence.
Our meta-analysis has also reported both adjusted and unadjusted NNTH, a beneficial measure to arrive at appropriate clinical decisions,64 65 which is an added strength to our systematic review and meta-analysis. From this meta-analysis, it was clear that 12.5, >1000, 100, 100, 5.9 and >1000 patients need to undergo EC for one additional patient to have pain, biliary pancreatitis, CBD stones, cholangitis, total biliary complications and mortality, respectively, as compared with CM/DC. The review findings are in favour of EC, as a better treatment option, compared with CM/DC.
This systematic review and meta-analysis have some limitations. We compared EC with CM (including both OM and EM) and DC, which might have contributed some heterogeneity in data.
However, we have tried to address it through subgroup analysis. Few RCTs included in this study had a high risk of bias in the domains of randomisation and deviation from intended intervention. In most of the outcomes analysed, publication bias was also observed. We could not collect all the evidences, since full texts of some published studies that met with the inclusion criteria were not available even after requesting the corresponding authors. The presence of many zero cells indicates rare events, which were statically handled through zero correction in our meta-analysis. We found that there are insufficient studies in many subgroups. Particularly, there was only one study that compared EC with OM for acute cholecystitis. Therefore, it is recommended to conduct further RCTs in future, which may bridge this knowledge gap.
In conclusion, EC is more effective in gallstone disease management, as it results in fewer biliary complications and a reduction in reported abdominal pain than DC/CM.
Data availability statement
No data are available. All the data is available in the online supplementary material.
Ethics statements
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors BSB: conceptualisation, data curation, formal analysis, inputs on original draft Investigation, methodology, software, review and editing. MH: conceptualisation, data curation, formal analysis, original draft. AS: data curation, review and editing. KVJ: data curation, review and editing. NKO: critical review and editing.
Funding The HTA resource centre ICMR-NIE is funded by the Department of Health Research Government of India.
Disclaimer Funders had no role in the conceptualisation, study conduction and manuscript preparation.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.