Article Text

Abstract
Objective Hepatitis C virus (HCV) infection is common. Although treatment is effective, with oral antivirals curing >95% of patients, most individuals have comorbidities that persist long term. Therefore, our aim was to determine the prevalence of potentially modifiable health problems in patients with HCV and develop an HCV care bundle to identify and target comorbidities.
Design Cross-sectional, observational single-centre study that recruited consecutive patients with HCV from our viral hepatitis clinics. Data were collected on cardiovascular (CV) risk factors, lifestyle behaviours, anthropometry and health-related quality of life (HRQoL). QRISK 3 was used to predict 10-year CV event risk.
Results 100 patients were recruited (67% male, 93% white, median age 52 years (range 24–80); 71% were treated for HCV; 34% had cirrhosis; 14% had diabetes; 61% had hypertension; 31% had metabolic syndrome; and 54% were smokers). The median 10-year CV event risk was 8.3% (range 0.3%–63%). 45% had a predicted 10-year CV event risk of >10%. Only 10% of individuals were treated with statins and 27% with antihypertensives. 92% had a predicted ‘heart age’ greater than their chronological age (median difference +7 (−4 to +26) years). HRQoL was reduced in all SF36v2 domains in the cohort. Factors independently associated with HRQoL included cirrhosis, metabolic syndrome, history of mental health disorder, sedentary behaviour and HCV viraemia.
Conclusion A large proportion of patients with HCV presented with increased risk of CV events, and rates of smoking and sedentary behaviour were high, while prescribing of primary prophylaxis was infrequent. HRQoL was also reduced in the cohort. A ‘care bundle’ was developed to provide a structured approach to treating potentially modifiable health problems.
- HCV
- quality of life
- diabetes mellitus
- obesity
- cardiovascular disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known about this subject?
Patients with hepatitis C virus (HCV) frequently have comorbidities that persist despite successful antiviral therapy, and this is associated with reduced health-related quality of life (HRQoL). HCV is also an independent risk factor for type 2 diabetes mellitus (T2DM) and cardiovascular (CV) disease.
What are the new findings?
We found that our cohort of patients with HCV were at high risk of CV events, with 92% having a higher risk than expected for someone of their age using QRISK3.
Despite the cohort having high rates of smoking, hypertension, obesity, dyslipidaemia and T2DM, few patients had these risk factors treated.
HRQoL was reduced in all domains of the SF36v2 in this cohort of patients with HCV.
Factors independently associated with HRQoL included cirrhosis, metabolic syndrome, history of mental health disorder, sedentary behaviour and HCV viraemia.
How might it impact on clinical practice in the foreseeable future?
This work has highlighted the need to assess and treat CV risk factors in individuals with HCV.
Our findings suggest that engaging sedentary individuals with HCV in a physical activity/exercise programme may improve their general health and well-being.
A ‘care bundle’ was developed to help clinicians actively look for and treat potentially modifiable health problems, including CV disease, depression, alcohol consumption and substance misuse.
Introduction
Hepatitis C virus (HCV) infection is common, affecting an estimated 71 million people worldwide.1 In England, latest estimates suggest there are 113 000 individuals chronically infected with HCV, with injecting drug use (IDU) accounting for 85% of infections.2 Chronic HCV infection causes persistent hepatic inflammation that progresses to cirrhosis in 10%–20% of infected individuals after 20–30 years.3 4 The development of cirrhosis is associated with a significant risk of developing liver failure, hepatocellular carcinoma and the potential requirement for liver transplantation.3 5
There has been substantial progress in the treatment of HCV and now >95% of patients treated with an oral combination of direct acting antivirals (DAAs) for 8–12 weeks achieve sustained virological response (SVR=cure of the infection).6 Given the wide availability of DAAs, there is an unprecedented opportunity to eliminate this infection worldwide.7 8 Despite progress in antiviral therapy, up to 40% of infected individuals remain undiagnosed, and a large proportion of those previously diagnosed are lost to follow-up.2 9 In order to work towards HCV elimination, viral hepatitis teams have had to invest significant resources on case finding and have streamlined treatment pathways with far fewer clinical contacts in order to upscale treatment rates. Previously, when patients received interferon-based treatment, they were provided with regular holistic care, addressing all of their health needs. As a result of the streamlining of care pathways with DAAs, care of patients with HCV may have become less holistic, reducing opportunities to address non-HCV-related health needs.
Following successful antiviral therapy for HCV, almost all patients (99%) have at least one comorbidity that persists long term.10 This includes neuropsychiatric conditions, such as depression, anxiety and mood disorders.11 HCV is also an independent risk factor for type 2 diabetes mellitus (T2DM) and cardiovascular (CV) disease, and as a result is associated with an increased risk of early CV-related mortality and all-cause mortality.12–14 Successful treatment of HCV may reduce future risk of CV events and the development of T2DM,15 16 but even individuals with treated HCV remain at risk of CV complications.17 Health-related quality of life (HRQoL) is also reduced in patients with HCV compared with the general population.18 Treatment of HCV may lead to sustained improvement in HRQoL, but impaired HRQoL frequently persists despite HCV treatment due to associated comorbidities.19 20
The aim of this study was to assess a cohort of patients with HCV to determine the burden of other health problems that could be targeted to improve their health and well-being and ultimately to improve care pathways for these individuals by addressing their other health needs. Specifically, we aimed to
Characterise the cardiometabolic risk status in individuals with HCV and to identify modifiable factors that can be targeted for improvement.
Characterise HRQoL status in individuals with HCV and identify modifiable factors that could be targeted for improvement.
Develop a simple ‘care bundle’ for individuals with HCV to help their treating teams recognise and address some of their other important health needs during their HCV treatment.
Methods
Study design
This was a cross-sectional, observational study that recruited 100 consecutive patients with HCV (treated or untreated) attending viral hepatitis clinics at The Newcastle upon Tyne Hospitals NHS Foundation Trust.
Patients
Patients over the age of 18 years were included if they had chronic HCV infection (defined as HCV RNA detectable in blood for >6 months) or had achieved SVR (3 months post-treatment) following treatment for chronic HCV infection. Patients were excluded if they were currently on antiviral treatment for HCV or within 3 months post-treatment, were coinfected with hepatitis B or HIV, had a history of hepatocellular carcinoma, had a history of liver transplantation; had decompensated cirrhosis (Child–Pugh Score≥7), or were unable to give informed consent.
Outcomes
The primary outcome of the study was to identify the proportion of patients with one or more cardiometabolic risk factors, including (1) overweight or obesity, (2) insulin resistance/T2DM (fasting glucose>5.6 or diagnosed with T2DM or glycated haemoglobin (HbA1c)>48 mmol/mol), (3) hypertension (blood pressure>130/85 or specific treatment for hypertension), and (4) dyslipidaemia—reduced high-density lipoprotein (HDL) (<1.03 mmol/L for men or <1.29 mmol/L for women) or triglycerides>1.7 mmol/L or specific treatment for lipid disorder.21
Secondary outcomes included (1) individuals’ projected 10-year risk of a CV event as defined by QRISK3, (2) smoking status, (3) patients’ current physical activity levels, (4) prevalence of harmful or hazardous alcohol use, and (5) HRQoL as assessed by the Hepatitis Quality of Life Questionnaire (HQLQv2) and factors associated with impaired HRQoL.
Data collection variables
Clinical and laboratory data were collected prospectively from the time of enrolment. Relevant clinical details, including gender, age, weight, height, body mass index (BMI) and waist circumference were obtained. Smoking history was documented as never smoked, current smoker or previous smoker (for >1 year). History of previous IDU was recorded as never, previous or current (within the last month). Blood tests were taken, including full blood count, urea and electrolytes, liver enzymes, HbA1c, lipids, glucose, vitamin D and HCV RNA using standard techniques. A detailed medical history, including a list of current prescribed medications, was recorded and cross-referenced with information from primary care.
Information was collected on their HCV infection history, including suspected route of infection, previous antiviral treatment and outcomes, and current status (active HCV viraemia or SVR). Stage of liver fibrosis was defined using transient elastography and categorised as minimal or mild fibrosis (liver stiffness measurement (LSM)<8 kPa), moderate-advanced fibrosis (LSM 8–12.4 kPa) or cirrhosis (LSM>12.5 or liver biopsy demonstrating Ishak stage V or VI fibrosis or imaging evidence of cirrhosis with portal hypertension).
The history of current alcohol consumption was evaluated by documenting individuals’ reported current average alcohol consumption in UK units/week over the previous year. Previous ‘heavy’ alcohol consumption was defined as >30units/week for women or >50 units/week for men for >1 year. The Alcohol Use Disorders Identification Test (AUDIT) questionnaire was also completed by each individual.22 An AUDIT score of ≥8 indicates an increased risk of hazardous/harmful alcohol consumption; ≥15 indicates high risk of hazardous/harmful alcohol consumption; and ≥20 indicates possible alcohol dependence.
Data were also collected on history of previous CV disease, including ischaemic heart disease, cerebrovascular disease, peripheral vascular disease or atrial fibrillation. CV risk was determined using QRISK3 (www.qrisk.org). This is a validated online tool used to estimate an individual’s predicted 10-year risk of having a CV event based on a number of readily available clinical variables, such as blood pressure, smoking status, presence of T2DM, BMI, family history, cholesterol:HDL ratio and history of medical conditions associated with increased CV risk. All information required for calculation of QRISK3 was collected. The QRISK3 also calculates a patients’ ‘healthy heart age’, which is the estimated age of a healthy person of the same sex and ethnicity with the same 10-year QRISK3. We compared patients’ chronological age with their estimated biological heart age (estimated heart age–chronological age) to give an assessment of their CV health compared with their peers.
Patients’ current self-reported physical activity level was recorded as sedentary, engaging in regular moderate physical activity (≥150 min/week of activity that leads to faster breathing, increased heart rate and feeling warmer) or regular vigorous physical activity (≥75 min/week of activity that leads to very hard breathing, shortness of breath, rapid heartbeat and should leave a person unable to maintain a conversation comfortably). Body composition was measured using 8-point Bioelectrical Impedance Analysis (BIA) (SECA BIA mBCA 525 Machine, SECA, UK).
Information on history of mental health disorders was also collected. We defined a ‘significant’ mental health disorder as one where pharmacological treatment was used for its treatment. HRQoL was determined using the HQLQv2, a survey to assess the functional health and well-being of patients with HCV, using a combination of the Short-Form 36v2 (SF36v2) Health Survey and 15 additional questions that measure other generic heath concepts relevant in assessing the impact of hepatitis. The SF36v2 consists of a survey of questions that are used to construct scores for eight domains (0–100 scale) and from these two, summary scores reflecting physical health (physical health component summary (PCS) score) and mental health (mental health component summary (MCS) score) are generated. SF36v2 scores presented in this study for the eight domains, the PCS and MCS were normalised to the US general population to have a mean of 50 and and SD of 10.23 Therefore, SF36v2 scores below 50 were considered reduced HRQoL. For the hepatitis-specific scores, the Hepatitis Distress Scale (HD), positive well-being (PWB), Hepatitis-specific Limitations Scale (HLIM) and Hepatitis-specific Health Distress Scale (HHD) scores ranged from 0 to 100 (not normalised to the US population), with higher scores indicating better HRQoL.
Measure of deprivation
The home postcode for each patient was mapped onto the English Indices of Deprivation using the Index of Multiple Deprivation (IMD).24 The lower layer super output area (LSOA) was calculated for each individual patient postcode. Deciles (1–10) for the IMD are calculated by ranking the 32 844 LSOAS in England from most deprived to least deprived and dividing into 10 equal groups (1 being the most deprived area decile and 10 the least deprived).
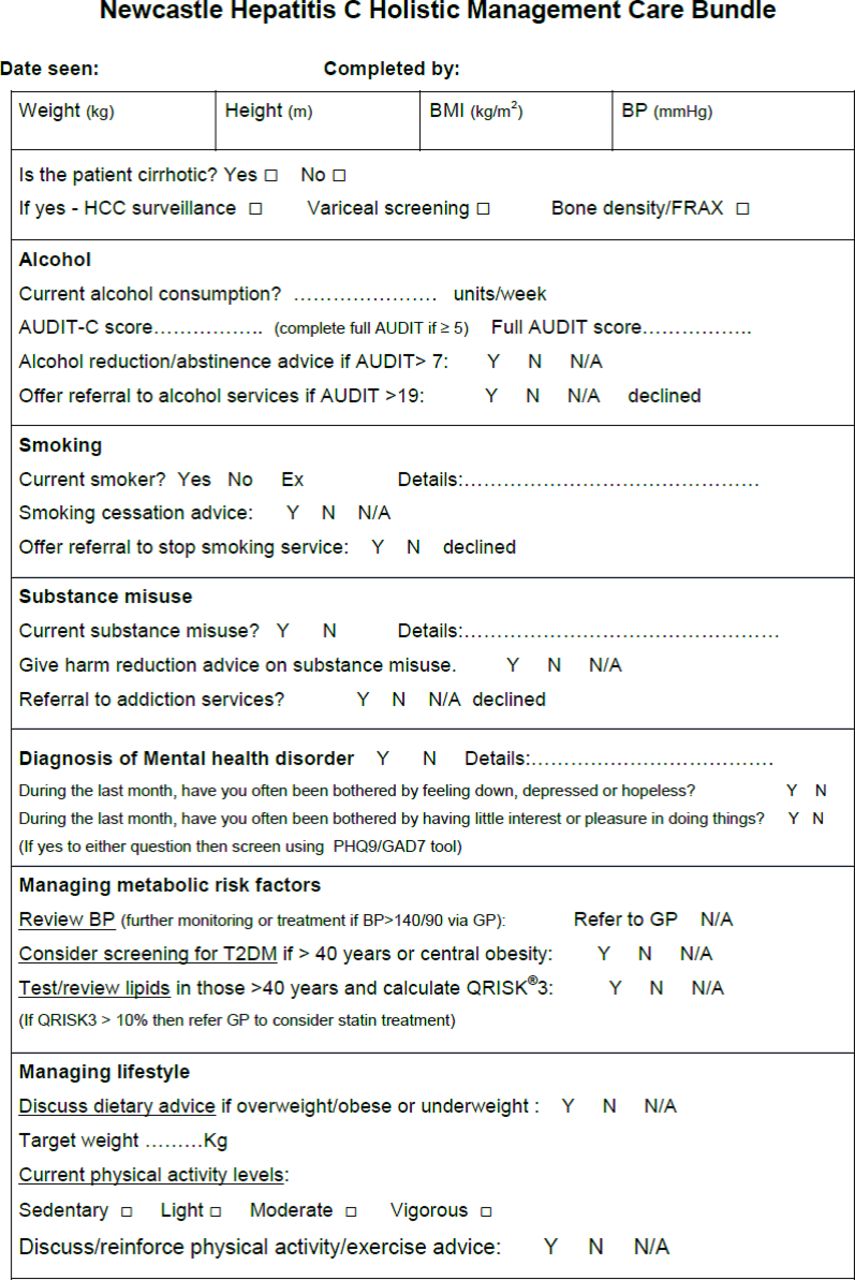
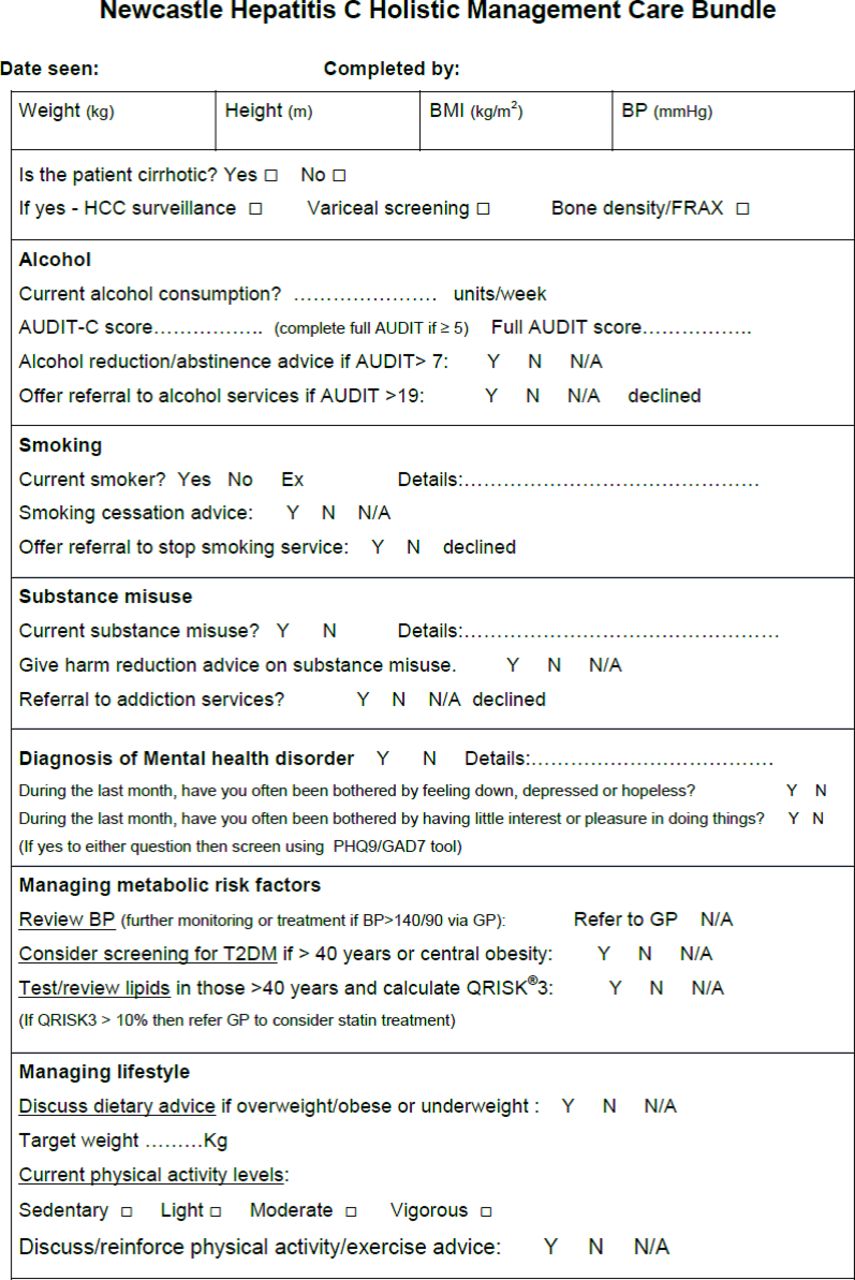
Development of the care bundle
A care bundle was developed to address general health needs of patients based on the findings from this study. Recommendations within the bundle are based on National Institute of Health and Care Excellence (NICE) guidelines.25–30 The bundle was initially developed by KH, PP and SMcP and then revised in response to critical review by a panel of experts, including hepatologists, specialist nurses, lifestyle specialists, addiction specialists and patients.
Statistical analysis
All statistical analyses were performed using the SPSS software V.24.0. Continuous normally distributed variables are represented as mean and ±SD. Categorical and non-normal variables are summarised as median and IQR. χ2 tests were used to determine the distribution of categorical variables between groups. To compare the means of normally distributed variables between groups, Student’s t-test or analysis of variance test was performed. To determine differences between groups for continuous non-normally distributed variables, medians were compared using the Mann-Whitney U-test. The strength of association between clinical variables was assessed by Pearson or Spearman correlations. To identify factors independently associated with PCS and MCS, a backward stepwise binary logistic regression was conducted, including variables associated with the outcome on univariate analysis with a p value of <0.2. Backward stepwise linear regression was used to identify factors independently associated with the hepatitis-specific HRQoL scores (HD, PWB, HLIM and HHD), including all variables associated with a univariate analysis p value of <0.2. Gender and index of deprivation were included in all models. A p value of <0.05 was considered significant.
Results
Patients
One hundred patients with HCV (viraemic or successfully treated) were recruited to this study. The patient characteristics are shown in table 1. Overall, two-thirds of the cohort was male and the majority (93%) was of white ethnicity. The mean age was 51±13 years (range 24–80 years). Overall, 71% had treated HCV and 29% were viraemic (5% of these had failed antiviral treatment). Thirty-four per cent of the cohort had cirrhosis (LSM>12.5 kPa) and 54% had minimal or mild liver fibrosis (LSM<8 kPa).
Overview of the clinical and demographic features of the cohort
The main risk factor for HCV acquisition was IDU in 60% of cases. Seven per cent of the cohort were regularly engaging in IDU and 24% regularly engaged in substance misuse. The overall median alcohol consumption was 0 unit/week (IQR 0–10), but this ranged up to 280 units/week. A total of 23% of the cohort consumed >14 units of alcohol per week and 44% had a history of previous ‘heavy’ alcohol consumption (>30 units/week for women and >50 units/week for men for >1 year). The median AUDIT score was 3 (IQR 0–10) and 29% had an AUDIT ≥8, suggestive of increased risk of hazardous/harmful drinking, while 7% had an AUDIT ≥20 indicating possible dependence. Overall, 76% of the cohort were in the lower 5 deciles of the IMD (indicating higher deprivation) and 59% were in the lowest three deciles.
Cardiometabolic risk factors
The mean BMI was 27.9±6 kg/m2 with 28% and 38% of individuals classified as overweight or obese, respectively. Thirty-seven per cent of patients had central obesity as defined by International Diabetes Federation waist circumference criteria.21 A total of 14% had diagnosed T2DM and two patients had undiagnosed T2DM. Sixty-one per cent had hypertension and 27% (44% of those with hypertension) were treated with antihypertensive medications. Thirty-nine per cent had dyslipidaemia (reduced HDL, triglycerides>1.7 mmol/L or specific treatment for lipid disorder), and 10% were treated with lipid-lowering drugs. Thirty-one per cent of the patients had metabolic syndrome, and 80% had one or more metabolic risk factors.21 Remarkably, 79% had a history of smoking, and 54% were current smokers.
Fifty-nine per cent of the patients self-reported being sedentary, while 26% reported regular moderate physical activity and 15% regular vigorous physical activity. Body composition was assessed in 58 individuals using bioimpedance, and the median fat mass in men was 28.7% (IQR 21.8%–33.1%) and that in women was 39% (IQR 26.9–41.6). Of these individuals, 65% of women and 58% of men had body fat levels above normal (25%+ for men and 32%+ for women). There were strong relationships between total fat mass and both BMI (rs=0.64, p=0.006 for women and rs=0.67, p<0.001 for men) and waist circumference (rs=0.56 p=0.02 for women and rs=0.71 p<0.001 for men). Overall, there was a relationship between fat mass and the number of features of the metabolic syndrome (rs=0.37, p=0.006). There were no relationships between fat mass and activity levels (p>0.05).
Projected 10-year CV event risk
In total, 9% of patients had a formal diagnosis of CV disease. The median 10-year CV event risk estimated by QRISK3 was 8.2% (range 0.3%–63%, IQR 3.1–16.2). Overall, 45% of individuals had a predicted 10-year CV event risk of >10%, all of which were aged over 45 years. Despite presenting with a CV event risk indicative of statin treatment,29 only 10% of these individuals were treated with lipid-lowering drugs. Remarkably, 92% had a predicted biological ‘heart age’ greater than their chronological age (median difference +7 (−4 to +26) years). There was no significant difference between the predicted biological heart age and chronological age for individuals with treated HCV and those with active HCV (p=0.92). Patients with cirrhosis had a significantly higher median predicted 10-year CV event risk than patients without cirrhosis (11.1% (IQR 7.7–19.2) vs 5.3% (IQR 1.6–14.5), p=0.002).
Psychological comorbidity and HRQoL
This cohort had a very high prevalence of mental health disorders with 53% having a history of treatment for a mental health disorder, such as depression, anxiety or other psychiatric disorders. HRQoL was reduced in the cohort with mean scores for all domains of the SF36v2 being below that of the general population (figure 1A). Table 2 shows the relationship between clinical factors and both the PCS and the MCS scores for the whole cohort. Overall, the PCS score were significantly associated with the age, presence of cirrhosis, the metabolic syndrome, history of a mental health disorder, regular physical activity level and index of deprivation. Factors associated with the MCS were the presence of the metabolic syndrome, history of a mental health disorder, current smoking, IDU history, regular physical activity level and index of deprivation.
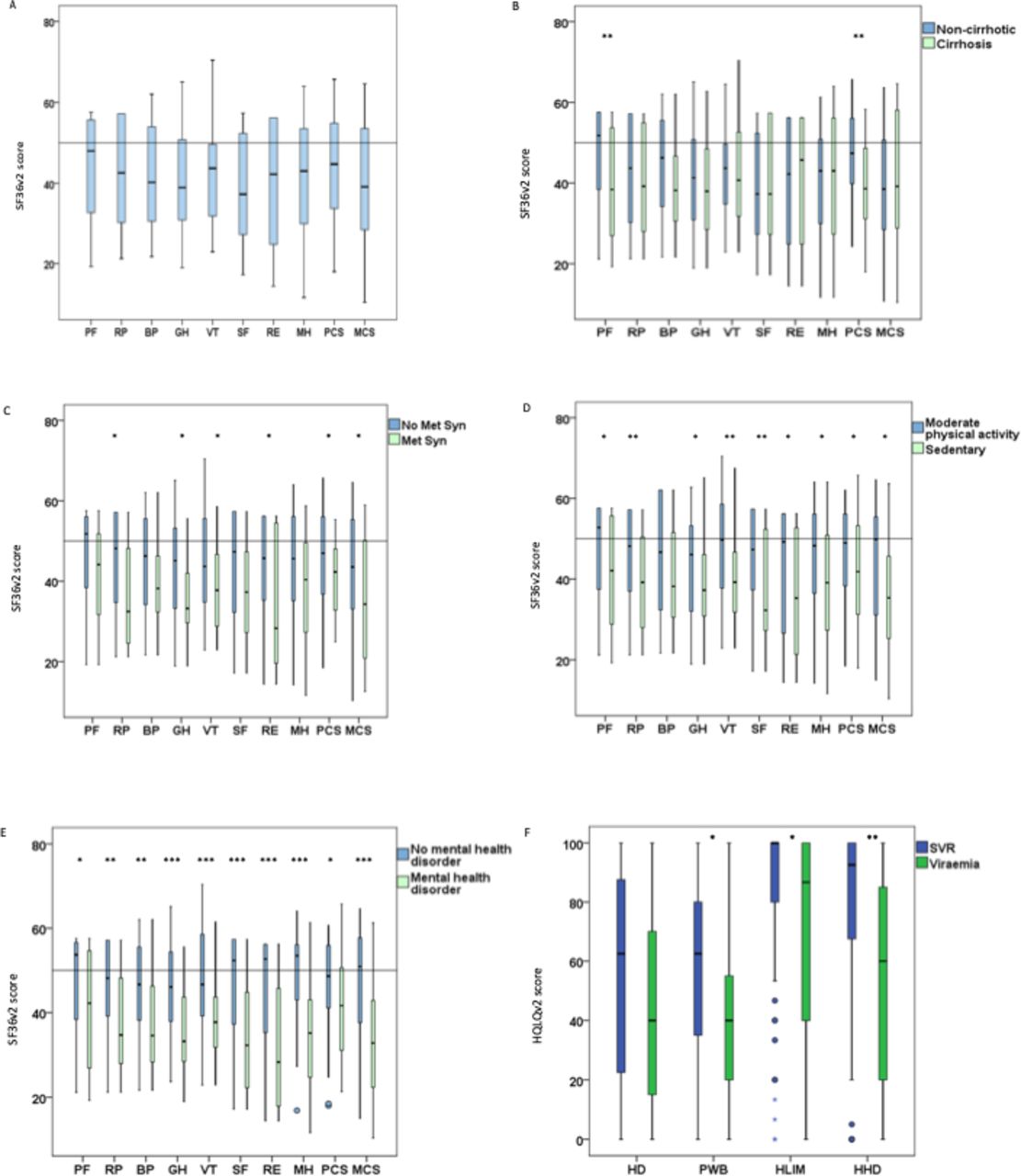
(A) HRQoL measured using the SF36v2 for the cohort. (B) A comparison between SF36v2 scores for HRQoL between individuals with and without cirrhosis. (C) Comparison between SF36v2 scores for HRQoL between individuals with and without metabolic syndrome. (D) Comparison between SF36v2 scores for HRQoL between individuals, depending on engagement in regular moderate physical activity. (E) Comparison between SF36v2 scores for HRQoL between individuals with and without a diagnosis of a mental health disorder. (F) Comparison of scores for the hepatitis-specific domains of HRQoL between individuals with active viraemia and those who achieved SVR. (A–E) Data are displayed for the eight domains and the two composite summary scores (physical health component summary and mental health component summary). SF36v2 scores for the domains and summary scores were normalised to the US general population. Scores below 50 (horizontal black line) indicate reduced HRQoL. (F) These scores were non-normalised. Conditional differences between groups and were assessed by t-test (B–E) and Mann–Whitney U -test (F). * denotes <0.05; ** denotes <0.01 and *** denotes <0.001. BP, bodily pain; GH, general health; HD, Hepatitis Distress Scale; HHD, Hepatitis-specific Health Distress Scale; HLIM, Hepatitis-specific Limitations Scale; HRQoL, health-related quality of life; MCS, mental health component; Met syn, metabolic syndrome; MH, mental health; PF, physical functioning; PHC, physical health component; PWB, positive well-being; RE, role—emotional; RP, role—physical; SF36v2, Short-Form 36v2; SF, social functioning; SVR, sustained virological response; VT, vitality.
Relationship between PCS and MCS and clinical factors
Following multivariate analysis (table 3) correcting for gender and index of deprivation, presence of cirrhosis and the metabolic syndrome were independently associated with reduced PCS (<50). Reduced MCS (<50) was independently associated with regular moderate physical activity and a history of mental health disorder after correcting for gender and index of deprivation (table 3). A comparison of the individual components of the SF36v2 between individuals with and without the factors independently associated with PCS and MCS is shown in figure 1B–E.
Independent factors associated with unfavourable PCS, MCS and the hepatitis-specific HRQoL scores
Relationship between clinical factors and hepatitis-specific HRQoL domains
Relationships between clinical factors and the hepatitis-specific HRQoL domains for the entire cohort are shown in online supplementary table 1. History of depression, current substance misuse and a sedentary lifestyle were associated with a lower (worse) HD score (p<0.001, p=0.02 and p=0.02, respectively). Achieving SVR and engaging in regular physical activity were associated with a higher PWB score (p=0.04 and p=0.01, respectively), whereas a diagnosis of depression was associated with a significantly lower score (p<0.001). Patients with viraemia had a significantly lower (more limitation) HLIM score (p=0.03). A lower (more distress) HHD score was associated with the presence of HCV viraemia and a diagnosis of depression (p=0.004 and p<0.001, respectively).
Supplemental material
To determine factors independently associated with the hepatitis-specific HRQoL domains, multivariable linear regression correcting for gender and index of deprivation was performed (table 3). This identified that a sedentary lifestyle, the presence of a psychiatric disorder and current substance misuse were independently associated with the HD score. The PWB score was independently associated with a sedentary lifestyle and a history of mental health disorder. The presence of viraemia and current substance misuse were independently associated with the HLIM score. The HHD score was independently associated with achieving SVR, exercising more frequently and a diagnosis of depression. Figure 2F shows scores for the hepatitis-specific HRQoL domains for individuals who were viraemic and those who had achieved SVR.
{kind=link}
{kind=link}
Care bundle. AUDIT, Alcohol Use Disorders Identification Test; BMI, body mass index; BP, blood pressure; FRAX, fracture risk assessment tool; GAD7, General anxiety disorder 7; GP, general practitioner; HCC, hepatocellular carcinoma; N, no; N/A, not applicable; PHQ9, patient health questionaire - 9; T2DM, type 2 diabetes mellitus; Y, yes.
Discussion
HCV is one of the major causes of cirrhosis worldwide. In addition to causing hepatic complications, HCV is associated with extrahepatic manifestations, including an increased risk of T2DM, CV disease and neuropsychiatric conditions.11–14 The aim of this study was to assess a cohort of patients with HCV to determine the burden of health problems that could be targeted to improve their health and well-being, specifically cardiometabolic risk factors and HRQoL, and to develop a care bundle to improve the holistic care of these patients. One of the most striking findings from this study was that the cohort had a very high estimated CV event risk. Remarkably, 92% of the cohort had an estimated heart age, using QRISK3, greater than their chronological age. Overall, 45% of individuals in the cohort had a predicted 10-year CV event risk of greater than 10%, a rate at which NICE guidelines recommend primary prevention with statin treatment.29 Unfortunately, rates of statin and antihypertensive prescribing were low at 10% and 27%, respectively, meaning many of these individuals were not receiving treatments known to extend life and reduce CV risk. Moreover, statins may have other benefits to patients with HCV, including potentially slowing progression to cirrhosis, reducing risk of hepatic decompensation and reducing incidence of hepatocellular carcinoma.31 32 This high overall CV risk in the cohort is most likely due to the very high rates of smoking in the cohort (54% current smokers vs 14% in the UK general population)33 and the high prevalence of metabolic risk factors, with 80% having one metabolic risk factor and 31% having full metabolic syndrome. HCV is well known to have complex interactions with glucose and lipid metabolism that may impact on CV risk.34 Recent data have suggested that successful treatment with DAAs improves glycaemia and reduces incidence of T2DM.35 36 However, serum cholesterol and low-density lipoprotein levels may increase post-treatment,36 emphasising the importance of assessing individual CV risk. It is not clear from our study why rates of prescribing drugs for primary prevention of CV risk were low in this cohort. This could be due to patient factors, such as individuals not attending for annual medical reviews or patients declining treatment with these drugs. It is also possible that some patients may not be offered regular CV reviews or treatment due to discrimination because stigma about HCV still exists in healthcare systems.37
Another important finding in this study was the overall high prevalence of reduced HRQoL in the cohort, with mean values for all domains of the SF36v2 being lower than the average for the US general population.23 This is probably due to a number of factors including the high prevalence of deprivation, mental health disorders, cirrhosis and the metabolic syndrome in the cohort. In this study, the presence of both cirrhosis and metabolic syndrome were independently associated with reduced overall physical health (PCS). Both of these factors have been shown to be associated with reduced HRQoL in other populations (both HCV and non-HCV).18 38 Factors independently associated with reduced overall mental health (MCS) in our cohort were a history of a mental health disorder and sedentary behaviour. A sedentary lifestyle and a history of a mental health disorder were also independently associated with lower scores in the hepatitis-specific scores: HD, PWB and HHD. We were not able to determine whether the association between engagement in regular moderate physical activity and better mental health was ‘cause’ or ‘effect’. The fact that we found associations between both presence of the metabolic syndrome and history of a mental health disorder and reduced HRQoL and found a positive impact of physical activity on HRQoL suggests that engaging sedentary individuals with HCV in a physical activity/exercise programme may improve their general health. Formal assessment of a physical activity/exercise programme as a treatment strategy for reduced HRQoL in patients with HCV is worthy of a trial.
Our data illustrated that the presence of HCV viraemia was associated with reduced scores in the hepatitis-specific HRQoL domains; HLIM and HHD. Previous studies have shown that successful treatment of HCV infection is associated with reduced risk of liver-related complications, overall mortality, improved HRQoL, reduced risk of CV events and reduced incidence of T2DM, so treating HCV in infected individuals is a priority.15 16 However, as shown in the current study and others, despite successful clearance of HCV, the majority of individuals have comorbidity that persists, which may impact on health and well-being.19 20 With recent advances in antiviral treatment for HCV, nearly all patients can achieve SVR (cure) with a short course of DAAs.6 Given the simplicity of DAA treatment, patients with HCV now have far fewer clinical contacts with viral hepatitis teams than they did when treated with interferon-based treatment in the past. Moreover, many clinical teams are now focussing resources on trying to ‘eliminate’ HCV and are treating many more patients than previously.2 As a result, the care of individuals with HCV may have become less holistic. Given that we have demonstrated a high burden of potentially modifiable health problems in this cohort, this suggests we should incorporate more holistic care in our HCV treatment pathways. Care bundles have been shown to improve care in patients with liver disease in other settings.39 40 We therefore developed a clinical care bundle (figure 2) to address some non-HCV-related health problems. This bundle provides a checklist to ensure that patients are offered appropriate surveillance of cirrhosis-related complications; an assessment of CV risk; advice on smoking cessation, alcohol consumption and substance misuse; screening for depression and advice on physical activity and lifestyle in line with NICE guidelines. There is some evidence in the qualitative literature that treating HCV in infected individuals can be a ‘turning point’ in their lives, helping them focus on their general health.41 We hope that use of this bundle will help improve the general health and well-being of our patients. This bundle could be adapted for use in different settings specifically indicating who is responsible for managing specific aspects of the bundle (eg, primary care for initiating and monitoring the CV management and addiction services for managing substance/alcohol misuse). Formal evaluation of the impact of the care bundle is planned.
This study has some limitations. First, patients were recruited from hospital HCV clinics, which is likely to have a selection bias. A large proportion of our patients are now treated in community or prison clinics, so the prevalence of specific comorbidities addressed may be different in these settings. This cohort was older and had a higher prevalence of cirrhosis than patients seen our community outreach clinics.42 However, mental health disorders (up to 71%), excessive alcohol consumption (up to 29%) and other comorbidities were very prevalent in our community clinics, so patients are likely to benefit from a holistic, care bundle approach irrespective of their treatment setting. Second, the SF36v2 data were normalised to the US general population because UK data were not available to us. There may therefore be differences between the UK and US general populations for the SF36v2 that we were unable to account for in this study. Third, this was a relatively small study with relatively few HCV viraemic individuals limiting its power to assess some outcomes.
In conclusion, we have demonstrated that patients with HCV are at high risk of CV events, and potentially modifiable risk factors are not being addressed adequately. In addition, HRQoL is reduced in all domains of the SF36v2 compared with the general population, and this is associated with the presence of cirrhosis, HCV viraemia, the metabolic syndrome, history of mental health disorder and sedentary behaviour. A care bundle has been developed with the aim of improving the general health and well-being of individuals with HCV.
Acknowledgments
We thank the LIVErNORTH charity for funding this study.
References
Footnotes
Twitter @stumcp
Contributors Study design and concept: SMcP, KH and MC; funding acquisition: SMcP and MC; data collection: SMcP, SG, SH and RW; data analysis: SMcP, PP, AW, KH and MC; writing and approval of the final manuscript: all authors; development of the care bundle; SMcP, KH, PP, AW and MC; guarantor SMcP.
Funding LIVErNORTH Charity.
Competing interests SMcP: consultancy/speakers fees from Abbvie, Allergan, BMS, Cambwick, Gilead, Intercept, MSD, Novartis and Sequana.
Patient consent for publication Not required.
Ethics approval This study was approved by North East–Tyne and Wear South Research Ethics Committee (16/NE/0239) and all participants provided written informed consent before enrolment.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Data are available on request from stuart.mcpherson2@nhs.net.