Article Text

Abstract
Objective To evaluate the impact of comorbidities and extraintestinal manifestations of inflammatory bowel disease on the response of patients with inflammatory bowel disease to antitumour necrosis factor alpha (anti-TNFα) therapy.
Design Data from 310 patients (194 with Crohn’s disease and 116 with ulcerative colitis) treated consecutively with the first anti-TNFα in 24 Spanish hospitals were retrospectively analysed. Univariate and multivariate logistic regression analyses were performed to assess the associations between inflammatory bowel disease comorbidities and extraintestinal manifestations with anti-TNFα treatment outcomes. Key clinical features, such as type of inflammatory bowel disease and concomitant treatments, were included as fixed factors in the model.
Results Multivariate logistic regression analyses (OR, 95% CI) showed that chronic obstructive pulmonary disease (2.67, 1.33 to 5.35) and hepato-pancreato-biliary diseases (1.87, 1.48 to 2.36) were significantly associated with primary non-response to anti-TNFα, as was the use of corticosteroids and the type of inflammatory bowel disease (ulcerative colitis vs Crohn’s disease). It was also found that myocardial infarction (3.30, 1.48 to 7.35) and skin disease (2.73, 1.42 to 5.25) were significantly associated with loss of response, along with the use of corticosteroids and the type of inflammatory bowel disease (ulcerative colitis vs Crohn’s disease).
Conclusions Our results suggest that the presence of some comorbidities in patients with inflammatory bowel disease, such as chronic obstructive pulmonary disease and myocardial infarction, and of certain extraintestinal manifestations of inflammatory bowel disease, such as hepato-pancreato-biliary conditions and skin diseases, appear to be related to failure to anti-TNFα treatment. Therefore, their presence should be considered when choosing a treatment.
Trial registration number NCT02861118.
- TNF-alpha
- immune response
- Crohn's disease
- ulcerative colitis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known about this subject?
Different real-life studies have investigated factors that might predict response to antitumour necrosis factor alpha (anti-TNFα) drugs in patients with inflammatory bowel disease (IBD); however, none has specifically addressed the impact of comorbidities and extraintestinal manifestation (EIM) profile on the response to these therapies.
What are the new findings?
To the best of our knowledge, this is the first study to assess the association between comorbidities and EIM profile of patients with IBD and the response to the first treatment with an anti-TNFα.
How might it impact on clinical practice in the foreseeable future?
These results may be useful in selecting those patients who most likely can benefit from anti-TNFα therapies.
Specifically, the results suggest that chronic obstructive pulmonary disease, myocardial infarction, hepato-pancreato-biliary conditions and skin diseases may have a negative influence on anti-TNFα treatment outcomes.
Introduction
Inflammatory bowel disease (IBD) describes a group of chronic, progressive disorders that predominantly affect the bowel. Although the pathophysiology is not fully known, it seems that environmental factors and an abnormal immune response to enteric microbes play a role in individuals with a genetic predisposition.1 Crohn’s disease (CD) and ulcerative colitis (UC) are the two main forms of IBD. The disease often has an onset during young adulthood and a course characterised by remission and relapse phases.2 The progressive organ damage results in a negative impact on the patient’s health-related quality of life (HRQoL) and in a major economic burden for both society and health services.3–7
The Spanish incidence of IBD seems to have increased in recent years, similarly to other countries,8 9 and ranges between 8 and 11 cases per 100 000 inhabitants per year.10–12
IBD has been frequently associated with comorbidities that, although not having a direct relationship with bowel inflammation, can modify the course and management outcomes of the disease.13 The prevalence of comorbidities in patients with IBD ranges between 30% and 70%.14–16 The presence of comorbidities in patients with IBD has been shown to negatively affect patients’ HRQoL,16 and importantly to prolong their length of hospital stay and increase the risk of postsurgical mortality. Furthermore, immune-mediated inflammatory disorders associated with IBD have been proven to incur higher healthcare costs.14
In addition, up to 50% of patients with IBD may develop extraintestinal manifestations (EIMs) of the disease,17 involving multiple organ systems throughout the body,17 18 and sometimes being even more debilitating than the intestinal disease itself.19
In recent decades, the objective of IBD treatment has evolved from a symptomatic relief to symptomatic and endoscopic deep remission.20 21 Conventional treatment with corticosteroids and immunosuppressants has not been able to reduce the complications of the disease or modify its course.22–24 Over the last two decades, biologic treatments have been successfully used in patients with moderate to severe CD and UC who failed to respond to corticosteroids.25 Early introduction of biologic agents in patients with more serious disease is probably the most widely accepted management strategy.22–25 Antitumour necrosis factor alpha (anti-TNFα) monoclonal antibodies, such as infliximab and adalimumab, have been rather effective in inducing and maintaining mucosal healing and reducing surgery and hospitalisation rates for over 15 years. Nonetheless, since anti-TNFα therapy failures are not uncommon,26 27 many studies have investigated patient-related, disease-related and treatment-related factors predicting response to anti-TNFα agents in IBD. They have found associations among the response to anti-TNFα medications and disease duration, biomarker levels, genetic polymorphisms and immunopharmacological factors.27–30 However, there have not been studies conducted to determine the impact of comorbidities on anti-TNFα treatment response.
The primary objective of this study was to evaluate the impact of the comorbidity profile of patients with IBD on treatment response to the first anti-TNFα therapy. Secondarily, the impact of the EIM profile in patients with IBD on treatment response to the first anti-TNFα was assessed, the percentage of patients with IBD exhibiting comorbidities was described, and the comorbidity profile at each level of IBD severity was determined.
Methods
Study population
This study was a retrospective, non-interventional, observational, multicentre study involving 24 gastroenterology sites from Spain. The study included patients diagnosed with UC or CD who started their first anti-TNFα between June 2011 and June 2013. To minimise selection bias, patients were recruited consecutively.
Patients had to be diagnosed with UC or CD according to the ‘World Gastroenterology Organization Practice Guidelines for the Diagnosis and Management of IBD in 2010’.31 All patients must have been prescribed anti-TNFα treatment according to daily clinical practice and have given written informed consent.
Investigators collected data from medical charts, including sociodemographic information (age, gender, race, level of education, smoking habits and alcohol intake) and clinical information (concomitant diseases, EIM of IBD, date of diagnosis, previous treatments, current treatments, disease activity when starting treatment with anti-TNFα). When data were not properly recorded in the medical charts, particularly demographic information, they were obtained directly from patients during a routine visit.
Clinical outcome evaluation
Disease activity at the beginning of the reference period and at the study visit was assessed through the following variables: (1) for patients with UC, the Partial Mayo Score (PMS)32 for general disease activity, disease anatomical extent, and endoscopy findings; (2) for patients with CD, the Harvey-Bradshaw Index (HBI)33 for general disease activity, disease behaviour, and disease location; and (3) for patients with UC and CD, stool frequency, rectal bleeding, urgency, nocturnal stools, need for antidiarrhoeal drugs, constipation, abdominal tenderness, abdominal pain or cramping, anorexia, nausea, vomiting, fever, appetite loss, weight loss, fatigue, night sweats, stunted growth, primary amenorrhoea, general well-being, physician’s global assessment, and other complications.
The reference period of the study was defined as the interval between the start of anti-TNFα until either the study visit or lack or loss of treatment response or until treatment discontinuation. To assess the main outcome, non-responders were defined as those patients not achieving either a reduction in HBI of at least two points from baseline for CD,32 or a decrease in PMS of at least two points for UC.33 In the cases where these indexes were not available, clinical response was evaluated according to physician criteria as recorded in medical charts. In both cases, response was assessed after induction treatment (10 weeks after starting anti-TNFα) and after maintenance treatment (at least 6 months after starting anti-TNFα). Primary non-response (PNR) was defined as lack of response after induction treatment (weeks 0–10). Loss of response (LOR) was defined as loss of the effect of the drug along the follow-up in a patient with an initial response.34 Reasons to stop the drug were classified as PNR, LOR, side effect, remission or other.34
IBD comorbidities in patients with UC and CD (defined as the coexistence of another medical condition alongside IBD that did not imply causation) at the time of diagnosis and at the study visit were listed according to the Charlson index35 (table 1). EIMs in patients with UC and CD were chosen from a list from the European Crohn’s and Colitis Organisation guidelines.18
Charlson index
Statistical analysis
With an estimated 50% of non-responders to the first anti-TNFα treatment and considering a minimum sample of 10 patients who presented with the event of interest per independent variable included in the logistic regression model and a maximum of 10 independent variables per model, a sample of 200 patients with UC and 200 patients with CD were estimated.
All patients participating in the study who fulfilled the inclusion criteria and did not have a major deviation from the study protocol were included in the final analysis. Continuous variables were described as the number of patients with valid/missing observations, mean, and SD, or the median and IQR if required. Categorical variables were described by absolute and relative frequencies.
Pairwise comparisons were performed by t-tests, Mann-Whitney tests, analyses of variance or Kruskal-Wallis tests when comparing quantitative variables between study groups or categories and categorical variables, and with χ2 tests or Fisher’s exact tests when comparing categorical variables.
To analyse the factors associated with PNR or LOR, a univariate analysis was performed including the sociodemographic variables, comorbidities, EIM, and other clinical variables as factors. Afterwards, a stepwise (backward and forward) multiple logistic regression analysis was performed using as the dependent variable either PNR or LOR and as independent variables those considered potential factors in the univariate analysis (p<0.100). In addition, given the potential relevance of the type of IBD (CD or UC) and of concomitant treatments on the response to anti-TNFα medications, the type of IBD and the concomitant administration of immunosuppressants and corticosteroids were included as fixed factors in the models.
An additional analysis to evaluate the impact of the EIM profile on treatment response to the first anti-TNFα therapy was conducted. It was based on two stepwise multiple logistic regression analyses with PNR or LOR as dependent variables and all EIMs (arthropathy and arthritis, metabolic bone disease, eye disease, oral, aural and nasal disease, skin disease, hepato-pancreato-biliary disease, neurological disease, and cardiovascular, pulmonary and genitourinary manifestations) as independent variables. Again, type of IBD, treatment with immunosuppressants, and treatment with corticosteroids were included as fixed factors in the models.
Additionally, we analysed the associations among comorbidities and IBD severity at baseline. Patients were categorised as having a severe disease if HBI was >16 or PMS was 8–9. We performed a univariate analysis considering severity as the dependent variable and type of IBD and comorbidities as independent variables. Afterwards, a stepwise multiple logistic regression analysis was performed using non-severe disease as the dependent variable and as independent variables those that were significant at p<0.10 in the univariate analysis.
All data analyses were performed using IBM SPSS Statistics V.22.0 Statistical Package for Windows.
Results
Patient characteristics
A total of 357 patients with IBD were included in this study. Forty-seven patients were eventually excluded from the analysis due to screening failure. Of the 310 analysed patients, 194 were diagnosed with CD and 116 were diagnosed with UC. Subjects’ characteristics are shown in table 2. The mean age (SD) at the time of anti-TNFα treatment initiation was 38.8 (12.7) years for CD and 41.8 (13.3) years for UC. Men comprised 53.5% of the whole analysed population. There was a higher prevalence of non-smokers among patients with UC (60.3%) compared with patients with CD (44.3%). Likewise, there was a higher prevalence of ex-smokers in the UC subpopulation (32.0%) compared with patients with CD (26.8%). The median (IQR) time from diagnosis of IBD to anti-TNFα treatment initiation was 45.5 (11.6–156.0) and 43.8 (10.8–143.8) months for CD and UC, respectively. Eighty-two per cent of patients reported having been previously treated with corticosteroids, and 33.3% were still receiving concomitant corticosteroid therapy during the maintenance phase. In addition, 78.4% of the study patients had been previously treated with immunosuppressants, and 65% were still under immunosuppressant therapy during the maintenance phase.
Demographics and clinical characteristics
Comorbidities and EIMs
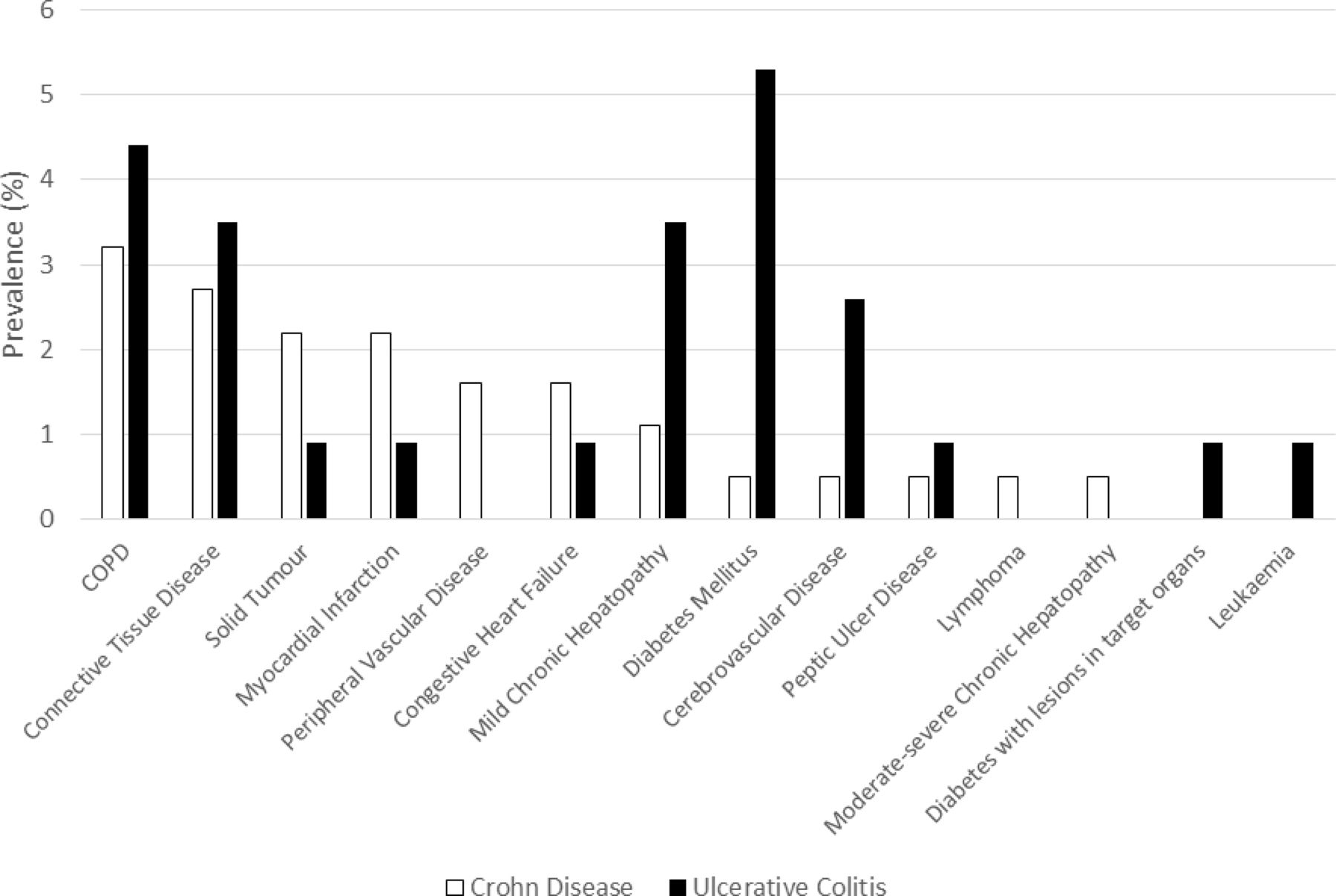
The Charlson comorbidity index mean values for CD were 0.21 (SD: 0.57), and 0.27 (SD: 0.72) for patients with UC. The prevalence of all individual comorbidities identified was below 6% (figure 1). Diabetes mellitus (5.3%) was the most prevalent comorbidity for UC, and chronic obstructive pulmonary disease (COPD) was the most prevalent among patients with CD (3.2%).

{kind=link}
Prevalence of comorbidities. The following comorbidities presented a prevalence of 0%: dementia, hemiplegia, moderate-severe chronic kidney disease, solid tumours with metastases, and AIDS. COPD, chronic obstructive pulmonary disease.
The prevalence of EIMs was higher in the UC subpopulation (32.8% vs 26.3%). The most frequent EIMs (table 3) were arthropathy and arthritis (17% for CD and 25% for UC), skin disease (8.8% for CD and 6% for UC), and metabolic bone disease (6.9% for UC).
Prevalence of extraintestinal manifestations of IBD
Factors associated with PNR and LOR to anti-TNFα
In the univariate analysis of comorbidities, COPD and solid tumours were identified as potential factors (p<0.10) associated with PNR. Multivariate logistic regression analysis showed that COPD (OR 2.67, 95% CI 1.33 to 5.35) was significantly associated with PNR to anti-TNFα, as was the use of corticosteroids and the type of IBD (UC vs CD) (table 4).
Multivariate logistic regression analysis of factors influencing efficacy
In the univariate analysis, myocardial infarction and skin disease were identified as potential factors (p<0.10) of LOR to anti-TNFα during the maintenance phase. Multivariate logistic regression analysis confirmed the association of myocardial infarction (OR 3.30, 95% CI 1.48 to 7.35) and skin disease (OR 2.73, 95% CI 1.42 to 5.25), along with the use of corticosteroids and the type of IBD (UC vs CD) (table 4), with LOR.
The additional analysis to evaluate the impact of the EIM profile in patients with IBD on treatment response to the first anti-TNFα therapy showed that the only EIM significantly associated with PNR was hepato-pancreato-biliary disease (OR 1.87, 95% CI 1.48 to 2.36), and the only EIM associated with LOR was skin disease (OR 2.58, 95% CI 1.98 to 3.35) (table 4).
Factors associated with IBD severity
In the univariate analysis, IBD type, cerebrovascular disease, leukaemia, diabetes mellitus, and diabetes with injuries to target organs were potential factors associated with IBD severity (p<0.1). UC, compared with CD, was significantly associated with more severe disease severity (OR 18.26, 95% CI 2.32 to 143.62).
Discussion
Although several studies have investigated the clinical and demographic factors that might predict PNR or LOR to anti-TNFα drugs in IBD, to the best of our knowledge, this is the first study to assess the association between the comorbidity profile in patients with IBD and PNR or LOR to anti-TNFα drugs.
The advent of anti-TNFα drugs supposed a substantial improvement in the management of IBD. However, up to 30% of patients do not respond to anti-TNFα therapy during the treatment induction phase (PNR), and 13%–20% lose the initial response over time (LOR).25 Consequently, personalised medicine approaches need to be developed to avoid the risk of non-response to a drug, identify those patients most likely to benefit from specific therapies and choose the best treatment for each individual patient either at the initiation of the therapy or at the eventual LOR.26 Some studies conducted in other autoimmune diseases, such as rheumatoid arthritis, have shown the negative impact of the presence of comorbidities on therapeutic response to biologics.36 37 In contrast, even though there have been a number of epidemiological studies assessing the prevalence of comorbidities associated with IBD,14–16 31 none has addressed the impact of the entire clinical profile of comorbidities and EIMs on the response to biologic therapy.
We found a statistically significant association among a few comorbidities and EIMs and both PNR to anti-TNFα during the induction phase (COPD) and LOR during the maintenance phase (myocardial infarction and skin diseases). As COPD, myocardial infarction and some skin diseases can aetiopathogenically be connected with smoking, it is plausible that the true factor behind the increased risk of PNR and LOR to anti-TNFα is smoking habit, in such a manner that COPD, myocardial infarction and skin diseases could be mere surrogates of smoking behaviour. However, this does not appear to be the case, as smoking habit was not identified under univariate analysis as a potential predictor of PNR (p=0.670) or LOR (p=0.677). In any case, in order to test this hypothesis more in depth, additional multivariate analyses were conducted, forcing three different variables related with smoking behaviour as independent variables: current smoker, ex-smoker and ever smoker. Interestingly, whereas none of these three variables was identified as an independent predictor of PNR or LOR, COPD, myocardial infarction and skin diseases kept significance as independent predictors of PNR or LOR (data not shown). This reinforces that the determinants of failure to anti-TNFα therapy are the identified comorbidities/EIMs, rather than smoking habits.
These comorbidities/EIMs had increased prevalence in many epidemiological IBD studies, and some aetiopathogenic explanations have been hypothesised.38–40 Overexpression of inflammatory factors and abnormal immune responses have been postulated as the common pathogenetic mechanisms underlying IBD and comorbidities. In some epidemiological studies, a strong association between COPD and IBD was found. Compared with healthy controls, the risk of COPD in patients with CD was 2.7-fold higher, and in UC it was 1.8-fold higher.38
In our study, COPD was among the most frequently reported comorbidities in both patients with CD (3.2%) and patients with UC (4.4%). Likewise, acute myocardial infarction was found to be almost three times as likely in patients with IBD as in matched controls in a population-based study.38 On the other hand, major skin involvement has also been described in 2%–34% of patients with IBD.39 However, it is difficult to diagnose these skin manifestations as EIMs because they can also arise as paradoxical reactions to anti-TNFα drugs.40 For example, some reports have suggested that inhibition of TNFα induces overexpression of cutaneous interferon-α, which in turn causes a predisposition to psoriasis.40 Hence, in light of the present results, when selecting an anti-TNFα for the treatment of patients with IBD, the identified comorbidities and EIMs predicting a possible drug response failure should be taken into consideration.
The prevalence of comorbidities in our study was relatively low compared with other studies.14–16 A plausible explanation might be that the median age of study patients was relatively young (approximately 44 years old). Another reason could be that many IBD specialists or even patients are reluctant to use biologic therapy, and we cannot discard a possible overlap between comorbidities and EIMs due to the retrospective study design. We also found an unusual distribution of comorbidities in the subpopulations of patients with CD and UC. Unlike most of the epidemiological data, we found higher prevalence of comorbidities and EIMs in UC than in CD. Interestingly, patients with UC in our study showed a significant association with a more severe disease compared with patients with CD, and also showed a significant association with PNR or LOR compared with patients with CD. Therefore, the higher disease severity in patients with UC included in our study may explain the higher occurrence of EIMs in this group. These findings are nonetheless in line with other published results.41–43 Park et al found disease severity to be a strong predictor of non-response to infliximab in patients with UC.43 The authors hypothesised that, unlike CD, UC seems to result from an immune response of type 2 helper T cells in the colonic mucosa, suggesting that TNFα would play no important role in the pathogenesis of UC.
We also found a significant association between the use of corticosteroids and both PNR and LOR. Some published studies have reported the early use of corticosteroids as an independent predictor of a disabling disease,44 of the need for anti-TNFα treatment dose intensification, and of an increased risk of anti-TNFα treatment failure.45 All these findings together appear to suggest that the early need for corticosteroids may be a proxy for disease severity or hard-to-treat disease.
Some of the limitations of the present study were the retrospective design and the lack of a control group. On the other hand, a requirement to a successful logistic regression model is to select appropriate variables to be entered into the model. While it is tempting to include as many input variables as possible, this can dilute true associations, or conversely identify spurious associations. In order to limit these risks, the conventional technique was followed, meaning to first run the univariate analyses to identify potential predictor variables, and then to use only those variables which meet a preset cut-off for significance to run a multivariate model.
Another limitation was the low frequency of comorbidities and EIMs observed, which may have reduced the statistical power to detect some other comorbidities or EIMs as predictors of PNR or LOR to anti-TNFα treatment in patients with IBD. In any case, the fact that some comorbidities or EIMs were identified as predictors of treatment failure, despite their low prevalence in the studied population, indicates that they show a strong association with PNR or LOR to anti-TNFα treatment. Furthermore, even though the UC patient sample was smaller than planned, which was probably because many patients with UC successfully responded to conventional therapies, both the final study sample size and the patient distribution were appropriate for meeting the study objectives.
Nonetheless, larger prospective controlled and preferably randomised studies are needed to confirm our results. In addition, a study assessing the impact of comorbidities on response to other biologics in the IBD population should be conducted to compare the study results with the results of the present study.
In conclusion, our results suggest that the presence of some comorbidities, such as COPD and myocardial infarction, and of certain EIMs of IBD, such as hepato-pancreato-biliary conditions and skin diseases, seems to be connected to the lower probability of therapeutic success with anti-TNFα. Therefore, the presence of these conditions in patients with IBD should guide clinicians when selecting the most appropriate treatment.
Acknowledgments
We would like to thank Ana Sánchez-Gabriel (Takeda Farmacéutica España), Tamara Pozo (Takeda Farmacéutica España), Teresa Letosa (Takeda Farmacéutica España), Yaiza Gimeno (Takeda Farmacéutica España), Silvia Vives (Takeda Farmacéutica España), Susana Vara (Apices) and Juan Luis Sanz (Apices) for their support in design, set-up, coordination, operation, monitoring, statistical analysis and medical writing. The following investigators contributed to patient recruitment and data collection: Dra Montserrat Rivero Tirado (H Marqués de Valdecilla), Dr Oscar Roncero (H La Mancha Centro), Dra Yolanda Ber (H San Jorge), Dr Fernando Bermejo (H Fuenlabrada), Dra Cristina Verdejo (H Ciudad Real), Dra Cristina Rodríguez Gutierrez (H Navarra), Dra Belén Botella (H Infanta Cristina), Dra Pilar López Serrano (H Alcorcón), Dra Silvia Chacón (H Morales Meseguer), Dr Daniel Ceballos (H Dr Negrín) and Dra Pilar Varela (H Cabueñes).
References
Footnotes
Contributors All authors have contributed to and agreed on the content of the manuscript: IM-J, GB, AF, EG-P, FA-A, MA, JS-F, MMB-W, RF, OM, XA, XC, BS, FM, and MB-A contributed to study design, patient recruitment, data collection and results interpretation. IT, AF-N, PS, and CM contributed to data analysis and interpretation, drafting of the report, and reviewed it critically. All authors approved the final version of the manuscript.
Funding The VERNE study was funded by Takeda Farmacéutica España SA.
Competing interests IM-J has served as a consultant, advisory member, speaker, or has received research funding from MSD, AbbVie, Takeda, Tillotts, Ferring, Falk Pharma, Faes Farma, UCB Pharma, Otsuka Pharmaceutical, Shire, Gebro Pharma, and Chiesi. GB has received a speaker honorarium from AbbVie, Pfizer, Janssen, FAES, Takeda, Tillotts and Abbott. Also, GB has participated in the scientific advisory committees of Takeda, Janssen and AbbVie. EG-P has served as a speaker or received research or educational funding or advisory fees from MSD, AbbVie, Janssen, Ferring, Shire, Tillotts, and FAES. FA-A has served as a speaker, a consultant and as an advisory member for or have received research funding from Janssen, MSD, AbbVie, Pfizer, Kern Pharma, Biogen, Sandoz, Takeda, Ferring, Faes Farma, Shire Pharmaceuticals, Dr Falk Pharma, Tillotts Pharma, Gebro Pharma, Amgen and Vifor Pharma. IT, AF-N, and CM are full employees of Takeda Farmacéutica España. PS was a Takeda Farmacéutica España employee at the moment this work was conducted. MA has served as a speaker for MSD, AbbVie, Janssen, Takeda and Tillotts, and received educational grants from Janssen, MSD and AbbVie. JS-F has nothing to declare. MMB-W declares educational activities, research projects, scientific meetings and advisory boards sponsored by MSD, Ferring, AbbVie, Janssen and Takeda. RF has served as a speaker for or has received research funding from Takeda, MSD, AbbVie, Janssen, Palex, Shire Pharmaceuticals, Tillotts Pharma and Casen Recordati. OM has nothing to declare. MB-A has served as a speaker, a consultant and advisory board member for, or has received research funding from, MSD, AbbVie, Janssen, Pfizer, Kern Pharma, Biogen, Takeda, Ferring, Faes Farma, Shire Pharmaceuticals, Dr Falk Pharma, Tillotts Pharma, Chiesi, Gebro Pharma, Otsuka Pharmaceutical and Vifor Pharma.
Patient consent for publication Not required.
Ethics approval The study was reviewed and approved by the corresponding ethics committees.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. The data that support the findings of this study are available from the sponsor upon request.