Article Text

Abstract
Objective Although sedation improves patient experience during colonoscopy, there is great jurisdictional variability in sedative practices. The objective of this study was to develop practice recommendations for the use of moderate and deep sedation in routine hospital-based colonoscopy to facilitate standardisation of practice.
Design We recruited 32 multidisciplinary panellists to participate in a modified Delphi process to establish consensus-based recommendations for the use of sedation in colonoscopy. Panel members participated in a values assessment survey followed by two rounds of anonymous online voting on preliminary practice recommendations. An inperson meeting was held between voting rounds to facilitate consensus-building. Consensus was defined as >60% agreement/disagreement with recommendation statements; >80% agreement/disagreement was considered indicative of strong consensus.
Results Twenty-nine panellists participated in the values assessment survey. Panellists ranked all factors presented as important to the development of practice recommendations. The factor considered most important was patient safety. Patient satisfaction, procedural efficiency, and cost were considered less important. Strong consensus was achieved for all nine practice recommendations presented to the panel. These recommendations included that all endoscopists be able to perform colonoscopy with moderate sedation, that an endoscopist and a single trained nurse are sufficient for performing colonoscopy with moderate sedation, and that anaesthesia-provided deep sedation be used for select patients.
Conclusion The recommendations presented in this study were agreed on by a multidisciplinary group and provide guidance for the use of sedation in routine hospital-based colonoscopy. Standardised sedation practices will promote safe, effective, and efficient colonoscopy for all patients.
- endoscopy
- colonoscopy
- screening
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known about this subject?
Sedation improves patient experience during endoscopy; however, there is wide variation in sedation practices.
What are the new findings?
Using consensus-based methods, an expert panel established recommendations for the use of sedation in colonoscopy; this study provides nine recommendations for sedation practice in colonoscopy.
These include the recommendation that all endoscopists be capable of performing colonoscopy under moderate sedation, with the assistance of a single trained nurse; and that select patients, such as those with severe comorbidities, may benefit from the presence of an anaesthesia provider during colonoscopy, irrespective of the level of sedation.
Further to this, the panel identified specific patient groups and contexts that should warrant consideration for deep sedation, including patients who are chronic opiate users, those who have previously not tolerated endoscopy under moderate sedation, and when a lengthy or complex procedure is anticipated.
How might it impact on clinical practice in the foreseeable future?
This study provides consensus-based recommendations to guide the use of sedation in colonoscopy.
These recommendations can be used to facilitate standardisation of sedation practices for routine, in-hospital colonoscopy, ensuring high-quality colonoscopy for all patients.
Introduction
Colonoscopy is an essential tool for the diagnosis and treatment of many intestinal conditions, including colorectal cancer. Patient pain and discomfort experienced during colonoscopy can necessitate early termination of the procedure prior to complete colonic visualisation and can lead to reluctance to undergo future procedures.1 Patient anxiety prior to and during the procedure may also be considerable and limit willingness to undergo colonoscopy. Therefore, strategies to optimise patient experience are important.
Sedation provides analgesia and anxiolysis during endoscopy and is recommended for most patients undergoing colonoscopy.2 Moderate sedation, commonly provided by a combination of midazolam and fentanyl, is usually administered by an endoscopist and monitored by a nurse, with no additional healthcare providers required. Patients sedated to this level are rousable with minimal tactile stimulation.3 In contrast, deep sedation with propofol can potentially alter cardiorespiratory function and even progress to general anaesthesia. Given this risk, in Ontario, propofol is delivered by individuals qualified to administer general anaesthesia—most commonly a trained anaesthesia professional who is responsible only for monitoring the patient3–6—even if moderate sedation with propofol is intended. Deeply sedated patients require repeated or painful stimulation to be roused.3 Deep sedation can be appealing for endoscopy as propofol has a quick onset and short plasma half-life,7 which can potentially enhance procedural efficiency,8 and is believed to result in greater patient satisfaction than moderate sedation.9 10
There are wide variations in sedation practices globally and regionally.11 In the UK, approximately 10% of colonoscopies are performed without sedation, <1% are performed with propofol, and the remainder are performed with moderate sedation.12 In contrast, in 2009, 12% of Canadian endoscopists reported use of propofol,13 and importantly 50% of gastroenterologists who were not using propofol expressed interest in its routine use,13 portending a rise in its popularity. In Ontario, Canada, the use of propofol has been quickly increasing. Nineteen per cent of colonoscopies performed in Ontario in 2005 included anaesthesia assistance14; by 2015, this estimate had increased to nearly 50%, although there was wide variability across institutions and regions (data available on request). This is important as the method of sedation delivery has potential quality and safety implications. Recent population-based studies report higher complication rates in colonoscopies performed with anaesthesia assistance, particularly aspiration.15 16 Additionally, use of anaesthesia services for colonoscopy comes at a significant monetary cost. In Ontario, colonoscopies performed with anaesthesia cost an additional $152.27 per procedure, translating into a budgetary impact of over $18 million in 2014/2015 (data available on request).
Given the variability in practices and the associated safety, satisfaction, and cost implications, guidance regarding sedation for colonoscopy is needed. The objective of this study was to develop consensus-based practice recommendations for the use of sedation in routine hospital-based colonoscopy to facilitate standardisation of practices.
Methods
Overview
We used a modified Delphi technique17–19 to develop consensus-based practice recommendations guiding the use of sedation for routine hospital-based colonoscopy (figure 1). We chose a consensus-based approach as a review of existing evidence revealed heterogeneous results and because this strategy allowed for incorporation of values from diverse perspectives. The Delphi technique is an iterative approach to gaining consensus from an expert panel. Participants are first asked to assess/rank statements through an anonymous survey. The group’s results are tabulated and presented to the participants, who then rerank the statements. This process of receiving tabulated results and reranking statements is continued until consensus is reached. The anonymity of the Delphi approach attenuates the influence of dominant opinions and feedback promotes convergence to consensus.20 The modified Delphi technique includes an inperson meeting, where additional information can be provided and clarifications can be made.

Consensus-building process.
This study is reported using the CREDES (Conducting and Reporting Delphi Studies) recommendations.21
Multidisciplinary panel recruitment
We used purposive sampling to select a multidisciplinary group of 32 panellists. Our panel size reflects our desire to recruit diverse panellists who represented a range of hospital settings, practitioners, and administrators. We included physicians (gastroenterologists, general surgeons, anaesthesiologists); endoscopy nurses and managers; public representatives; experts in health economics; representatives from Cancer Care Ontario, the College of Physicians and Surgeons of Ontario, and the Ontario Ministry of Health and Long-Term Care; and international experts in endoscopy. All participants were required to disclose conflicts of interest prior to participation.
Evidence reviews
To inform preliminary recommendations, the study team first systematically reviewed existing guidelines to assess the degree of consistency among current recommendations. As there was little consistency found among guidelines, the team next reviewed and summarised published literature in the following areas: (1) whether the presence of an anaesthesiologist influenced the safety and effectiveness of colonoscopy (irrespective of sedative agent used), (2) the incidence of complications in colonoscopy performed with propofol versus traditional sedatives (opioids and/or benzodiazepines), and (3) safety, satisfaction, and efficiency outcomes between colonoscopies performed with propofol versus midazolam and fentanyl (irrespective of sedative provider). The results of a published meta-analysis comparing propofol with traditional sedatives were also reviewed.10 Briefly, there were no statistically significant differences in rates of hospital admission, major complications (death, aspiration, splenic injury, myocardial infarction, stroke), polyp detection, caecal intubation, or patient satisfaction between anaesthesia and non-anaesthesia provider-administered sedation; however, results of studies reporting aspiration and bleeding rates were conflicting. There were no differences in cardiorespiratory events between patients sedated with propofol versus traditional sedatives. There were small improvements in patient satisfaction and recovery time with propofol versus midazolam and fentanyl. Members of the multidisciplinary panel received copies of the evidence summary.
Webinars and values assessment survey
Members of the multidisciplinary panel participated in 1.5-hour webinars where the evidence summary was discussed in detail. Additionally, the webinars were used to generate a list of factors and outcomes that panellists felt were important to consider in the development of practice recommendations for the use of sedation. Following the webinars, panellists received a link to an online, anonymous values assessment survey, where they were asked to indicate the importance, on a scale from 1 to 10, of each of 20 factors/outcomes that had emerged from the webinars.
Delphi process: round 1
Based on the results of the systematic reviews and values assessment survey, the study team drafted a set of nine preliminary practice recommendations. In the first round of the Delphi process, panellists were asked to indicate their level of agreement with and provide feedback on the nine recommendations through an online survey using a 5-point Likert scale; response frequencies were grouped into three categories: (1) agreement (strongly agree and agree), (2) unsure, and (3) disagreement (strongly disagree and disagree). A priori, consensus for agreement or disagreement was set at 60%17; >80% agreement or disagreement was considered indicative of strong consensus.
Consensus-building meeting
Panellists attended a 1-day consensus-building meeting to review the results of the values assessment survey and the first round of the Delphi process. Panellists were presented with data on the level of agreement/disagreement for each preliminary recommendation. Wording of recommendations was then refined through large group discussions. The meeting also included presentations by visiting experts, covering topics of discussion that had arisen during the webinars, and small group breakout sessions. The purpose of the small group sessions was to discuss (1) patients for whom deep sedation would be beneficial and (2) how to enhance the experience for patients undergoing routine colonoscopy with moderate sedation. Notes were taken during the small group and large group sessions to facilitate modifications to the practice recommendations based on the inperson discussion.
Delphi process: round 2
Following the consensus-building meeting, the practice recommendations were reworded and definitions of terms used were clarified. The multidisciplinary panel participated in a second round of online voting on the reworded practice recommendations, after which a set of final recommendations was drafted by the study team.
Patient and public involvement
We included public representatives in the expert panel to provide patient and public perspectives. These individuals participated in all aspects of the study involving the expert panel, including values assessment, webinars, Delphi process, and consensus-building meeting. We incorporated feedback received from these representatives into the recommendations provided.
Results
Panel composition
The multidisciplinary panel consisted of 32 members (online supplementary table 1), including 5 (16%) anaesthesiologists, 9 (28%) endoscopists (7 gastroenterologists, 2 surgeons), 4 (13%) Cancer Care Ontario representatives, 3 (9%) public representatives, 3 (9%) administrators/funders, 2 (6%) health economics experts, 3 (9%) endoscopy nurses, 2 (6%) hospital endoscopy programme managers, and 1 (3%) individual from the College of Physicians and Surgeons of Ontario. Two of the endoscopists were international experts.
Supplemental material
Values assessment
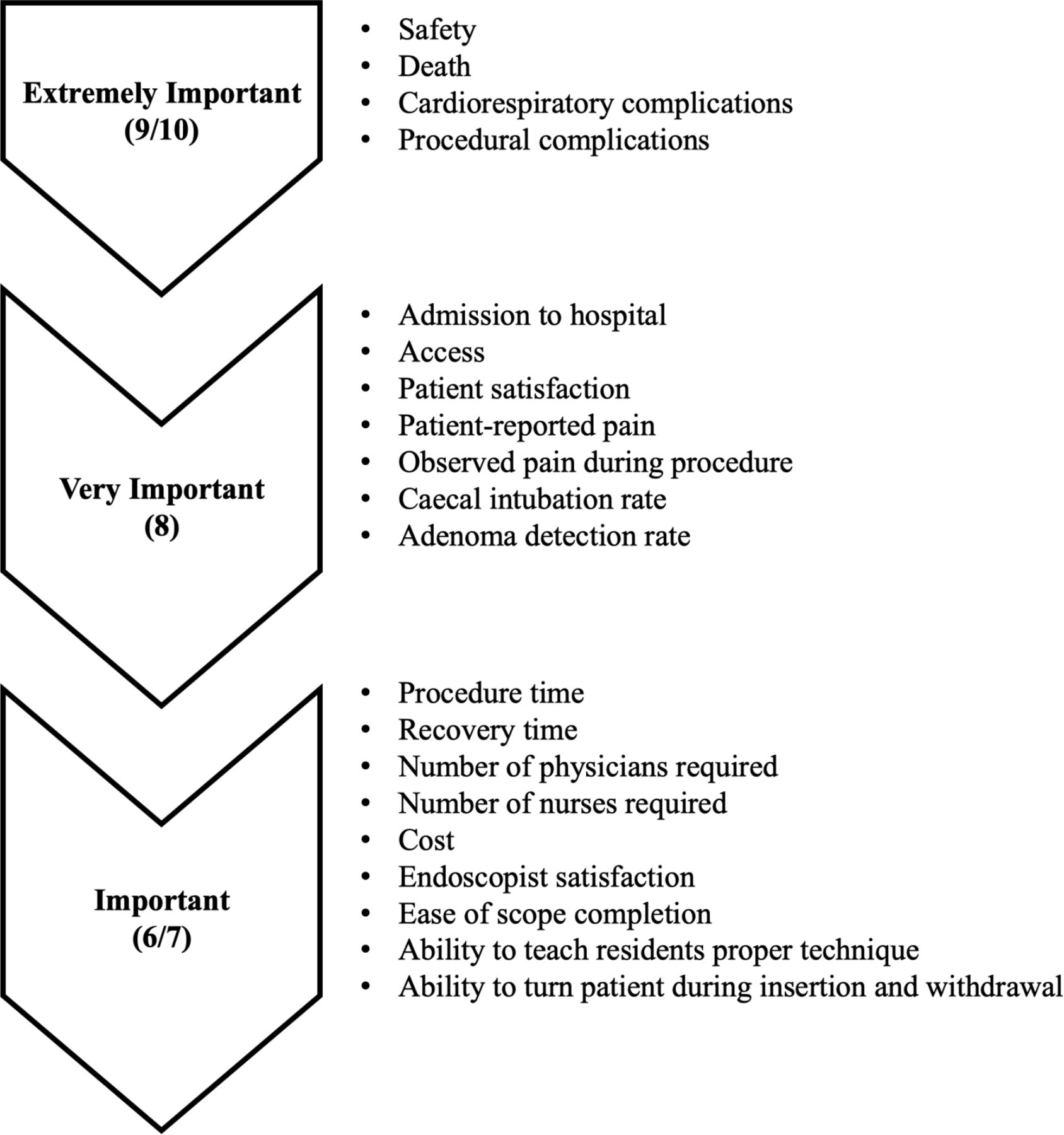
Twenty-nine panellists participated in the values assessment survey. The multidisciplinary panel deemed all 20 factors/outcomes included in the values assessment survey to be important considerations for the development of practice recommendations (figure 2). Factors judged as the most important (mean scores of 9–10 on a 10-point scale) were related to the safety of sedatives, including the outcomes of death, cardiorespiratory complications, and procedural complications. Patient-reported pain and factors related to colonoscopy quality (eg, caecal intubation rate, adenoma detection rate) were considered very important (mean score of 8); factors related to procedural efficiency and cost were considered less important (mean scores of 6–7).

{kind=link}
{kind=link}
Results of values assessment survey. Twenty-nine members of the expert panel participated in the values assessment survey. Panel members were provided with a list of 20 factors/outcomes and were asked to provide a score (1–10) indicating the importance of the factor in the generation of practice recommendations.
Delphi process round 1: preliminary practice recommendations
Based on the evidence review and results of the values assessment survey, nine preliminary practice recommendations were developed (online supplementary table 2) and presented to the multidisciplinary panel for ranking and comments. Although the safety of sedatives was considered the most important factor in the values assessment survey, preliminary practice recommendations did not include a statement favouring particular sedatives as the evidence review did not find any significant differences in safety outcomes between sedatives. Twenty-nine panellists participated in the first round of the Delphi process. Consensus was reached for all recommendations; strong consensus was observed for six of the nine recommendations (online supplementary table 2).
Consensus-building meeting
Thirty-one panellists attended the 1-day inperson meeting. As consensus was reached for all recommendations presented in the first round of online voting, the inperson meeting was used to present and discuss the results of voting, clarify wording of recommendations, discuss the recommendations for which strong consensus had not been achieved, and facilitate small group breakout sessions.
Small group session 1: deep sedation for routine colonoscopy
In the first small group session, participants identified patient groups that may warrant consideration for the use of deep sedation in specific circumstances, although it was recognised that these patient and clinical contexts do not necessarily mandate the use of deep sedation, that is, use should be considered on a case-by-case basis. Patient factors identified by panellists that may warrant consideration for use of deep selection in select cases included chronic opiate users, those who could not previously tolerate colonoscopy under moderate sedation due to discomfort, paediatric patients, and patients with hypersensitivities to traditional sedative agents, a history of sexual abuse, irritable bowel syndrome, fibromyalgia, cognitive disabilities (eg, dementia), or a history of diverticulitis. Contextual factors that could be considered when weighing the use of deep sedation included complex procedures (eg, endoscopic mucosal resection), lengthy procedures, and performance of colonoscopy at small centres where revenue generated for anaesthesiologists through endoscopy is required to maintain the anaesthesiologist workforce in the region (table 1).
Results of small group sessions
Small group session 2: enhancing patient experience under moderate sedation
Several strategies for enhancing patient experience under moderate sedation were identified by panellists (table 1). Methods suggested to be undertaken prior to the procedure included skills enhancement courses and setting patient expectations surrounding pain/discomfort. Suggested methods to be used during the procedure included appropriate titration of sedatives, use of abdominal pressure, variation in patient positioning, and use of carbon dioxide rather than air for insufflation. Postprocedure methods included follow-up phone calls or appointments for solicitation of feedback on the experience.
Delphi process round 2: final practice recommendations
Twenty-eight panellists participated in the second round of the Delphi, where they were presented with the nine reworded practice recommendations (box 1, online supplementary table 3). Strong consensus was achieved for all recommendations.
Final practice recommendations
Definitions
Routine colonoscopy: colonoscopy provided in the elective, ambulatory setting to stable patients (ASA category I–III). Routine colonoscopy can include procedures such as biopsy and polypectomy, but does not include interventions such as planned resection of large polyps, placement of colonic stents and so on.
Levels of sedation: we have defined moderate and deep sedation using categories from the ASA. Of note, the level of sedation refers to the targeted level of sedation, acknowledging that occasionally patients will become more deeply sedated than intended. Such occasions must be recognised and managed, and the patient returned to the intended level of sedation. In general, when ‘traditional agents’ such as midazolam and fentanyl are used, a moderate level of sedation is targeted. In general, when propofol is used, a deep level of sedation is targeted.
Moderate sedation is a drug-induced depression of consciousness during which patients respond purposefully to verbal commands, either alone or accompanied by light tactile stimulation. No interventions are required to maintain a patent airway, and spontaneous ventilation is adequate. Cardiovascular function is usually maintained.
Deep sedation is a drug-induced depression of consciousness during which patients cannot be easily roused but respond purposefully following repeated or painful stimulation. The ability to independently maintain ventilator function may be impaired. Patients may require assistance in maintaining a patent airway, and spontaneous ventilation may be inadequate. Cardiovascular function is usually maintained.
Endoscopist: for these statements, an endoscopist is considered a practitioner (gastroenterologist, surgeon and so on) with sufficient training and skill to perform routine colonoscopy.
Anaesthesia provider: the term ‘anaesthesia provider’ is used to denote a practitioner with additional training in the delivery of anaesthesia and airway management. Non-physician anaesthesia providers (anaesthesia assistants) provide care under the authority of medical directives with the direct supervision of an anaesthesiologist certified by the Royal College of Physicians and Surgeons of Canada.
Brief interruptible task: for colonoscopy, brief interruptible tasks would include charting, providing pressure, as well as assistance with biopsies and simple polypectomies. If more technical assistance is required, a second assistant should be available to assist during the more demanding portion of the procedure.
Final practice recommendations
All endoscopists performing colonoscopy should be able to complete colonoscopy safely and effectively (per accepted benchmarks) using moderate sedation or less. (93%)
Endoscopists unable to complete colonoscopy safely and effectively (per accepted benchmarks) using moderate sedation should undergo additional training. (89%)
For patients undergoing routine colonoscopy, endoscopists can safely administer moderate sedation with the assistance of a trained nurse. (89%)
For routine in-hospital colonoscopy under moderate sedation, a single RN* can both monitor the patient and perform brief interruptible tasks. (86%)
Select patients undergoing routine colonoscopy may benefit from deep sedation. (93%)
Institutions will not mandate the use of deep sedation for routine colonoscopy. (93%)
Deep sedation for colonoscopy should only be administered by an anaesthesia provider. (82%)
For routine colonoscopy under deep sedation, an anaesthesia provider will be responsible for monitoring the patient and should not be responsible for additional tasks. (93%)
Select patients undergoing colonoscopy, such as those with severe comorbidities, may benefit from having sedation administered and monitored by an anaesthesia provider, irrespective of level of sedation. (96%)
Level of agreement (agree/strongly agree) with each practice recommendation in the final round of voting is indicated in parentheses.
*Assumes this RN is an experienced, trained endoscopy nurse.
ASA, American Society of Anesthesiologists; RN, registered nurse.
Interpretation
Using a multidisciplinary panel and modified Delphi methodology, we developed nine consensus-based practice recommendations for the use of sedation in routine hospital-based colonoscopy. Participants agreed that all endoscopists should be able to perform colonoscopy under moderate sedation with the assistance of a single trained nurse. Select patients, including those with severe comorbidities, may benefit from deep sedation and monitoring by an anaesthesia provider; however, deep sedation should not be mandated by hospitals.
The recommendations developed in our study largely align with recent guidelines put forth by the American Society for Gastrointestinal Endoscopy (ASGE) (table 2).2 These guidelines reinforce that moderate sedation can be administered by an endoscopist for most patients and that a trained nurse can both monitor a moderately sedated patient and perform brief, interruptible tasks. However, our recommendations differ from those of the ASGE in several key areas (table 2). Unique to our recommendations, participants agreed that endoscopists who are unable to perform colonoscopy with moderate sedation should undergo further training. Due to the high use of propofol at some hospitals, there may be endoscopists who have not performed colonoscopy under moderate sedation at all or for some time who would feel uncomfortable doing so. For these individuals, skills enhancement courses can be beneficial by providing strategies to minimise patient discomfort and improve caecal intubation and adenoma detection rates, such as by teaching torque steering and loop reduction, varying patient positioning to facilitate passage of the colonoscope,22–26 and use of carbon dioxide insufflation27–29 and water infusion techniques.30–32 Further recommendations made by the expert panel for improving patient experience under moderate sedation are provided in table 1. The ASGE document recommended that propofol be considered if it is expected to improve patient safety, comfort, procedural efficiency, or success, but suggested that whether an anaesthesiologist is involved in administration of deep sedation for low-risk cases be determined by state, regional, and local regulations. In contrast, the expert panel recommended that deep sedation only be administered by anaesthesia personnel, and identified specific patient and clinical contexts, not discussed in the ASGE document, that warrant consideration for use of propofol. These include select patients with irritable bowel syndrome, fibromyalgia, or previous diverticulitis, as well as smaller hospitals where revenue from providing endoscopic sedation is required to maintain the anaesthesiologist workforce. Both groups agreed that when deep sedation is used, an individual dedicated to administering and monitoring deep sedation, without any other responsibilities, is required.
Comparison of ASGE guidelines2 and consensus-based practice recommendations
The systematic reviews that informed our consensus-building process also identified multiple areas in which evidence is currently lacking or conflicting. We found many discrepancies among current guidelines relating to the administration of sedation. Our review of the safety of non-anaesthesia provider-administered sedation found conflicting results for the outcomes of aspiration and bleeding. Additionally, we found that propofol was associated with small improvements in patient satisfaction, but it was unclear whether differences of this magnitude were clinically meaningful. Further research in these areas will be important to providing evidence-based guidance for sedation.
Although our study focused on the Ontario hospital context, high use of deep sedation and variability in practices are a growing issue in other jurisdictions as well. These increases cannot be attributed to a changing patient demographic or case complexity. In a study of the use of monitored anaesthesia care (MAC) in the Veterans Health Administration, facility-level factors had stronger associations with MAC use than patient-level factors.33 34 Similarly, in Canada, an analysis by Cancer Care Ontario found that large endoscopy units, where complex procedures are most likely to be performed, had high variability in the use of anaesthesia, indicating that procedural complexity was not the main driver of anaesthesia use (data available on request).
Our study has limitations. Although we selected a diverse panel, sedation practices vary considerably by jurisdiction and members of our panel may not reflect the breadth of practice in all clinical settings, although they do adequately reflect a range of hospital-based practice models. Additionally, as recommended by the Guidelines International Network,35 the US Institute of Medicine/National Academy of Medicine,36 and the UK National Institute for Health and Care Excellence,37 we included public representatives in our panel to ensure incorporation of patient priorities and preferences. As most of our panellists were from Ontario, the recommendations developed in this study may be less applicable elsewhere; however, the panellists from outside of Ontario found the recommendations to be reflective of their experiences as well. Importantly, our reviews and recommendations did not evaluate long-term outcomes related to the effectiveness of colonoscopy.
Although our recommendations focused on hospital-based colonoscopy, the use of deep sedation has increased for other endoscopic procedures, including gastroscopy and flexible sigmoidoscopy performed in hospitals over the same period.38 39 Given that the role of deep sedation for these procedures is even more controversial,40 41 recommendations pertaining to other endoscopic procedures may also be helpful. Additionally, as consensus was built for our recommendations in the context of hospital-based colonoscopies, our recommendations may not be generalisable to endoscopy performed in the clinic-based setting, where other factors may necessitate the use of anaesthesia services. Further work will be required to create recommendations for sedation practices for colonoscopy performed in clinic-based facilities.
In conclusion, using a diverse panel and modified Delphi process, we developed nine consensus-based practice recommendations to guide use of sedation for routine hospital-based colonoscopy. The results can be used to inform hospital policy with respect to the use of sedation for in-hospital colonoscopy and can help facilitate the standardisation of sedation practices.
Acknowledgments
The authors would like to thank the members of the multidisciplinary panel for their time and contributions to this work. Additionally, the authors thank Anna Gagliardi for her work in planning and facilitating the multidisciplinary panel meeting, and Michelle Helm, Zahrah Khalid, Melissa Coulson, and Shamara Baidoobonso for their involvement in the meeting.
References
Footnotes
Twitter @fdossa, @enenbee
Contributors Conception and design: FD, CD, JT, AS, LR, BM, NB. Analysis and interpretation of data: FD, AS, JAD, NB. Drafting of the article: FD. Critical revision of the article for important intellectual content: FD, CD, JT, AS, LR, BM, JAD, NB. Final approval of the article: FD, CD, JT, AS, LR, BM, JAD, NB.
Funding This study was funded by the Canadian Institutes of Health Research (CIHR) Foundation Grant (no 148470) and with the support of Cancer Care Ontario (CCO) through funding provided by the Government of Ontario. The opinions, results, view, and conclusions reported in this publication are those of the authors and do not necessarily reflect those of Cancer Care Ontario.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the Research Ethics Board at St Michael’s Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.