Article Text

Abstract
Objective We report the only two adult cases of NH4OH ingestion described in literature at the Peradeniya Teaching Hospital in Sri Lanka. Both cases showed clinical evidence of gastrointestinal toxicity and using intestinal fatty acid binding protein (IFABP), a novel biomarker, we attempted to quantify the extent of enterocyte damage. Procalcitonin was also measured as a maker of bacterial sepsis to ascertain whether there was a link between enterocyte damage and infection secondary to bacterial translocation.
Cases A 45-year-old, previously well man was brought in by family with a reduced level of consciousness after ingestion of an unknown quantity of industrial NH4OH (29% solution) with suicidal intent. Peak IFABP and procalcitonin levels were 1274 pg/mL and 2.0 ng/mL, respectively, 7.7 hours following presumed ingestion. A 23-year-old, previously well woman presented 24 hours after consuming 100 mL of NH4OH (5.4% solution) used as a cleaning product. She presented with ongoing vomiting and oropharyngeal pain. Her peak IFABP and procalcitonin levels were 865 pg/mL and 5.8 ng/mL, respectively, 27.2 hours following ingestion.
Conclusion We report the only two adult cases of NH4OH ingestion and describe severe gastrointestinal damage both clinically and biochemically. IFABP, currently only a marker used in research settings, was elevated in both cases but only marginally below that of levels seen in mesenteric ischaemia (levels greater than 1300 pg/mL). The use of a marker for enterocyte damage especially in ingestion of caustic solutions can allow clinicians to monitor progress, predict complications and evaluate the need for further invasive procedures.
- ammonium hydroxide
- intestinal fatty acid binding protein
- caustic ingestion
- epithelial barrier
- gastrointestinal toxicity
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
- ammonium hydroxide
- intestinal fatty acid binding protein
- caustic ingestion
- epithelial barrier
- gastrointestinal toxicity
Introduction
Ammonium hydroxide (NH4OH) is a caustic solution with a pH between 10.1 and 13.8 (depending on concentration) that is used as a cleaning agent but also has industrial uses.1 We report the only two adult cases of NH4OH ingestion described in literature at the Peradeniya Teaching Hospital in Sri Lanka. Although NH4OH ingestion is rare, ingestion of other alkali are common and can acutely present with severe upper gastrointestinal mucosal injury leading to perforation, mediastinitis and peritonitis.2 3 In contrast to acid ingestion which causes coagulative necrosis with eschar formation, alkali ingestion results in liquefactive necrosis of all layers of the gastrointestinal tract.4 5 Through our two cases, we attempted to quantify the extent of enterocyte damage and gastrointestinal toxicity using a novel non-invasive biomarker, plasma intestinal fatty acid binding protein (IFABP). Procalcitonin was also tested as a maker of bacterial sepsis to ascertain whether there was a link between enterocyte damage and infection secondary to bacterial translocation.
Cases
A 45-year-old, previously well man was brought in by family with reduced level of consciousness after ingestion of unknown quantity of industrial NH4OH (29% solution) with suicidal intent. He was last seen well 7 hours prior to presentation. On admission, his pulse was 120 bpm and regular, BP 100/80 mm Hg, respiratory rate (RR) 20, SpO2 98 on room air, febrile T 38.1°C and his Glasgow Coma Scale score was 7 (E2V1M4). He was subsequently intubated due to his lowered level of consciousness and commenced on intravenous cefepime 2 g twice a day and ranitidine infusion. On day 3, he was still intubated and had a haemoglobin (Hb) drop from 123 to 98 g/L and a urea rise from 14.1 to 23.2 mmol/L without clear evidence of melena or haematemesis. A chest X-ray and abdominal X-ray was performed which did not show evidence of perforation. His Hb stabilised with only supportive measures and an upper endoscopy was not performed due to resource limitations. By day 5, he was extubated and reported abdominal pain, dysphagia and odynophagia. He was discharged on day 7 with his symptoms improving and Hb stable.
A 23-year-old, previously well woman presented delayed by 24 hours following self-reported consumption of 100 mL of NH4OH (5.4% solution) used as a cleaning product. Her main symptoms were ongoing vomiting associated with oropharyngeal pain. On presentation, she was alert, with a regular pulse at 110 bpm, tachypnoeic at a RR of 28, blood pressure of 110/70 mm Hg, Hb of 126 g/dL and febrile T 38.2°C. She was given 8 mg of intravenous ondansetron three times a day, commenced on a regular ranitidine infusion and cefuroxime for microbial cover. On day 2 of admission, her vomiting had ceased but she complained of ongoing odynophagia, epigastric pain and low-grade febrile episodes. Her symptoms resolved with conservative management and oral antibiotics while her Hb remained stable throughout admission and she was subsequently discharged on day 5.
Methods
Serial serum samples were collected from patients taken at four different time points from time of admission over 24 hours. IFABP was tested using ELISA from Hycult Biotech, Netherlands. Procalcitonin was tested using enzyme-linked fluorescent assay technique.
Results
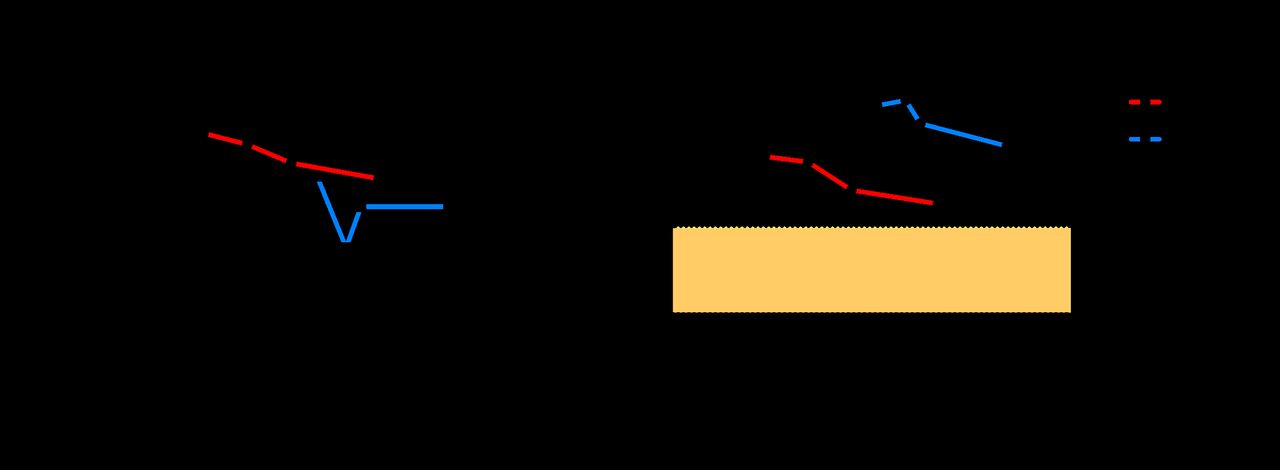
IFABP was raised in both cases following oral exposure to ammonium hydroxide (refer to figure 1). Patient 1, following ingestion of an unknown quantity of higher concentration industrial-grade ammonium hydroxide, had a peak IFABP of 1274 pg/mL after 7.7 hours following presumed ingestion. Patient 2 had a peak IFABP of 865 pg/mL after 27.2 hours of ingestion. Procalcitonin levels, a marker of sepsis, was raised in patient 2 with a peak of 5.8 ng/mL taken 27.2 hours following ingestion and was also raised in patient 1 with a peak of 2.0 ng/mL taken 7.7 hours after ingestion (refer to figure 1).
{kind=link}
Intestinal fatty acid binding protein (IFABP) (pg/mL) and procalcitonin (ng/mL) levels following time after ingestion (h).
Conclusion
We report the only two adult cases of NH4OH ingestion in literature and describe severe gastrointestinal damage both clinically and biochemically. IFABP, currently a marker used in research settings, was elevated in both cases but only marginally below that of levels seen in mesenteric ischaemia (levels greater than 1300 pg/mL).6 Unfortunately, gastrointestinal endoscopy and upper gastrointestinal contrast studies were not able to be done due to resource limitations which would have been helpful in comparing endoscopic/radiological with biochemical damage. The use of a marker for enterocyte damage especially in alkali ingestion can allow clinicians to monitor progress, predict complications and evaluate the need for invasive procedures. The cause of raised procalcitonin levels is however multifactorial and is partly due to liquefactive necrosis resulting in intestinal bacterial translocation.7 Correlation between enterocyte damage and intestinal bacterial translocation requires further research with a larger cohort. We report two unique cases not previously described in the literature and offer a novel non-invasive method to monitor gastrointestinal toxicity and enterocyte damage using IFABP.
Acknowledgments
We acknowledge Fahim Mohamed and Chathura Palanasinghe for their contribution to the study.
Footnotes
Contributors VP is the corresponding author with substantial contribution to the conception of the study, acquisition of data, analysis of data and interpretation of data. Also heavily involved in drafting the intellectual content. Also involved in the final approval of current version. Also accountable for all aspects of the work. TW had substantial contribution to the acquisition of data and analysis of data. Also heavily involved in drafting the intellectual content. Also involved in the final approval of current version. Also accountable for all aspects of the work. AN had substantial contribution to the acquisition of data. Also heavily involved in drafting the intellectual content. Also involved in the final approval of current version. Also accountable for all aspects of the work. IG had substantial contribution to the conception of the study. Also heavily involved in drafting the intellectual content. Also involved in the final approval of current version. Also accountable for all aspects of the work. AD had substantial contribution to the conception of the study and interpretation of data. Also heavily involved in drafting the intellectual content. Also involved in the final approval of current version. Also accountable for all aspects of the work. NB had substantial contribution to the conception of the study and interpretation of data. Also heavily involved in drafting the intellectual content. Also involved in the final approval of current version. Also accountable for all aspects of the work.
Funding Translational Australian Clinical Toxicology Program Pilot Grant—University of Sydney.
Competing Interests None declared.
Patient consent Obtained.
Ethics approval University of Peradeniya Ethics Review Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional unpublished data are only available to the corresponding author and the second author TW.