Article Text

Abstract
Background During COVID-19 pandemic, the safety of medical therapies for inflammatory bowel disease (IBD) in relation to COVID-19 has emerged as an area of concern. This study aimed to evaluate the association between IBD therapies and severe COVID-19 outcomes.
Method We performed a systematic review and meta-analysis of all published studies from December 2019 to August 2021 to identify studies that reported severe COVID-19 outcomes in patients on current IBD therapies including 5-aminosalicylic acid (5-ASA), immunomodulators, corticosteroids, biologics, combination therapy, or tofacitinib.
Results Twenty-two studies were identified. Corticosteroids (risk ratio (RR) 1.91 (95% CI 1.25 to 2.91, p=0.003)) and 5-ASA (RR 1.50 (95% CI 1.17 to 1.93, p=0.001)) were associated with increased risk of severe COVID-19 outcomes in patients with IBD patients. However, possible confounders for 5-ASA use were not controlled for. Sub-analysis showed that corticosteroids increased the risk of intensive care unit (ICU) admission but not mortality. Immunomodulators alone (RR 1.18 (95% CI 0.87 to 1.59, p=0.28)) or in combination with anti-TNFs ((RR 0.96 (95% CI 0.80 to 1.15, p=0.63)), tofacitinib (RR 0.81 (95% CI 0.49 to 1.33, p=0.40)) and vedolizumab ((RR 1.02 (95% CI 0.79 to 1.31, p=0.89)) were not associated with severe disease. Anti-TNFs (RR 0.47 (95% CI 0.40 to 0.54, p<0.00001)) and ustekinumab (RR 0.55 (95% CI 0.43 to 0.72, p<0.00001)) were associated with decreased risk of severe COVID-19.
Conclusion In patients with IBD, the risk of severe COVID-19 is higher among patients receiving corticosteroids. Corticosteroid use was associated with ICU admission but not mortality. The risk is also higher among patients receiving 5-ASAs. However, patient-level data were lacking and insufficient data existed for meta-regression analyses to adjust for confounding. Vedolizumab, tofacitinib, and immunomodulators alone or in combination with anti-TNF were not associated with severe disease. Anti-TNFs, and ustekinumab were associated with favourable outcomes.
- IBD
- COVID-19
- epidemiology
- pharmacotherapy
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) emerged in Wuhan, China in December 2019 and shortly after, it evolved into a global pandemic.1 2 SARS-CoV-2 is primarily transmitted through air droplets and aerosols. Airborne transmission is also a likely source of transmission.2 A significant number of patients develop severe respiratory symptoms requiring hospitalisation, intensive care admission, and death. In addition, vulnerable groups include elderly individuals, those with active malignancy and cardiopulmonary diseases, and immunocompromised individuals.3 4 While gastrointestinal (GI) manifestations of COVID-19 are also common, they are not associated with increased intensive care unit (ICU) admissions or mortality.5 Furthermore, a recent study found that while GI symptoms are common in patients with IBD with COVID-19, they are not associated with an increased risk of death due to COVID-19.6
SARS-CoV-2 enters human cells by binding to ACE2 and other receptors.7 Intestinal ACE2 is involved in the uptake of dietary amino acids, regulating the expression of antimicrobial peptides and promoting the homeostasis of the gut microbiome.7 Inflammatory bowel disease (IBD) is a chronic inflammatory condition of the gastrointestinal tract. Despite the use of gastrointestinal ACE2 receptors by SARS-CoV-2 to infect individuals, current data show patients with IBD were not at higher risk for COVID-19 infection.8
Patients with IBD often require long-term maintenance medical therapy such as 5-aminosalicylic acid (5-ASA), immunomodulators, janus kinase (JAK) inhibitors, biologic therapies, or corticosteroids.8 The effect of these medications on COVID-19 outcome is not fully understood. The Epidemiology of Coronavirus Under Research Exclusion (SECURE-IBD)9 database is an international registry that was established at the beginning of the COVID-19 pandemic, for reporting outcomes of COVID-19 in patients with IBD. To date, it includes outcomes of more than 6000 patients with IBD with COVID-19 infection from 72 countries worldwide. In addition, multiple studies have been performed to evaluate the safety of IBD medications during COVID-19 pandemic with conflicting data.6 10 11 Due to the rapidity of emerging data, up-to-date summary data are lacking. To our knowledge, there was no previous systematic review that looked at individual biologic therapy and risk of severe COVID-19. Moreover, this is the first and largest systematic review to include anti-TNF combination therapy and janus kinase inhibitors.
Methods
This systematic review and meta-analysis were conducted using the methods described in the Cochrane Handbook of Systematic Reviews and reported according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement.12 MOOSE guidelines were also followed.13
Eligibility criteria
Randomised, placebo-controlled, or active comparator-controlled trials, cohort studies, observational studies, and editorial were included. Furthermore, Surveillance Epidemiology of Coronavirus Under Research Exclusion (SECURE-IBD) data were included. Adult patients (age ≥18 years) with IBD and confirmed SARS-CoV-2 infection were included. Specifically, we included any study that reported hospitalisation, ICU admission or mortality data in patients with IBD infected with SARS-CoV-2, and IBD medical therapy taken at the time of the study. Our study analysed outcomes stratified by pharmacological treatments alone or in combination with other agents. We excluded case series, and case reports and any studies that did not have relevant outcome data. In addition, to avoid duplication, any study that reported data from the SECURE-IBD database was excluded. Finally, we also excluded studies that included paediatric patients only (age <18 years).
Definitions and outcome measures
The primary outcome measure was the risk of severe COVID-19 in patients taking IBD medications. For the purpose of this study, we defined severe COVID-19 as infection resulting in hospitalisation, ICU admission, or mortality. Mortality was defined as the number of patients who died within the study observation period. In addition, we performed a sub-analysis by exploring the risk of ICU admission and mortality separately with the use of specific IBD medications. Data on current use of IBD medications were extracted for 5-ASA, immunomodulators (thiopurines and methotrexate), calcineurin inhibitors, steroids, biological agents (tumour necrosis factor antagonists (anti-TNF), vedolizumab, ustekinumab), or janus kinase (JAK) inhibitors (tofacitinib). We looked at the association of severe COVID-19 and individual biologic agents when available. If data on individual biologic agent were not available, we grouped tumour necrosis factor antagonists (anti-TNF), vedolizumab, and ustekinumab under biologic agents, whereas methotrexate and thiopurines were grouped under immunomodulators. Data on concurrent use of anti-TNF agents and an immunomodulator (combination therapy) were also extracted.
Search strategy and data extraction
Literature searches were conducted by two authors (FA and IA) using MEDLINE, Embase, Scopus, and Cochrane Central Register of Controlled Trials databases from 1 December 2019 to 10 August 2021, using predefined strategies (online supplemental table 1). Our search strategies were designed with the help of a librarian. The search was restricted to English-language publications involving humans. English conference proceedings were searched (World Congress of Gastroenterology, American College of Gastroenterology, Canadian Digestive Disease Week, Digestive Disease Week, European Crohn’s and Colitis Organization congress, and United European Gastroenterology Week). Furthermore, clinical trials databases (www.clinicaltrials.gov and International Randomized Standard Clinical Trial (IRSCT) Register) were searched. Google Scholar was also searched for unindexed studies. In addition, SECURE-IBD database was searched for relevant data. The bibliographies of included studies and reviews were searched for additional eligible studies. Systematic reviews were also reviewed for relevant studies. The search terms used are outlined in online supplemental material.
Supplemental material
Data extraction and quality control were done independently by two reviewers (FA and IA). Discrepancies were resolved on discussion with a third reviewer (MS). The same two authors extracted information from the studies. Extracted information included baseline characteristics, type of IBD (ulcerative colitis vs Crohn’s disease), study design, country of publication, risk of bias, IBD medications, and outcomes using standardised Excel spreadsheet.
Risk of bias and study quality
To assess risk of bias and quality of the included studies, two authors (MS and FA) independently used the Cochrane risk of bias tool for randomised controlled trial (RoB 2)14 and ROBINS-I for assessing risk of bias in non-randomised studies of interventions.15 By using these assessment tools, studies were classified as being of unclear or low or high risk of bias. Seven domains—random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and other potential sources of bias—are included in this tool.
The quality of all included studies was assessed using the modified Newcastle-Ottawa Scale (mNOS).16 Three domains were assessed by using mNOS: selection, compatibility, and outcome. Study quality was defined as low (score of 0–3), moderate (score of 4–6), and high (score of 7 and 8).
Statistical analysis
The risk ratio (RR) was calculated to compare outcomes in patients taking specific IBD medications to those who were not receiving those medications at the time of the study. Statistical analysis was conducted using Review Manager (RevMan) V.5.3.5 (The Cochrane Collaboration). Prevalence and 95% CI were estimated using random-effects models assuming between and within study variability. I2 statistic, which ranges from 0% to 100%, was used to quantify the relative amount of observed heterogeneity. An I2 value less than 30% indicates low heterogeneity, whereas a range of 30%–75% indicates moderate heterogeneity and high heterogeneity was defined as I2 >75%.
Results
Search results
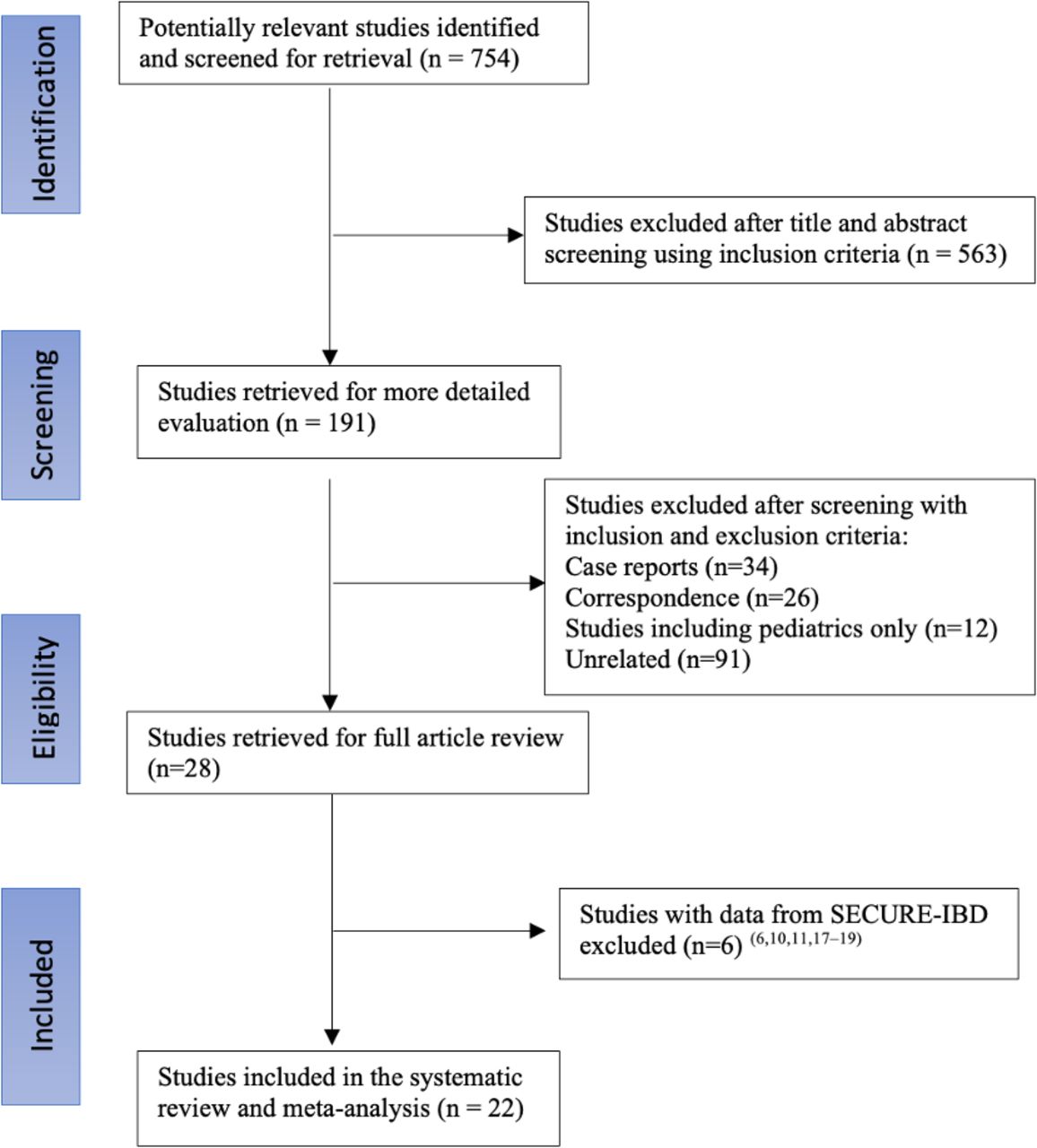
From the initial 754 studies identified in the search, 22 studies met criteria for inclusion (figure 1). This also includes the data extracted from the SECURE-IBD database. All included studies were observational, except for one study that was a randomised controlled trial. Six studies were conducted in Italy and the USA, three were done in the UK, and the rest were done in multiple countries including France, Spain, and Denmark. Table 1 provides details of the included studies and patients’ demographics. To avoid duplication of the same population, six studies were excluded as these studies reported data from SECURE-IBD only.6 10 11 17–19 In total, 10 391 patients with IBD and confirmed COVID-19 diagnosis were included in the main analysis. Mean age was 48.7 (±11.7) and 3864 (36%) were male. Among these patients, 4284 (30.5%) had ulcerative colitis, 5217 (48.6%) had Crohn’s disease, and the remainder did not specify IBD type.
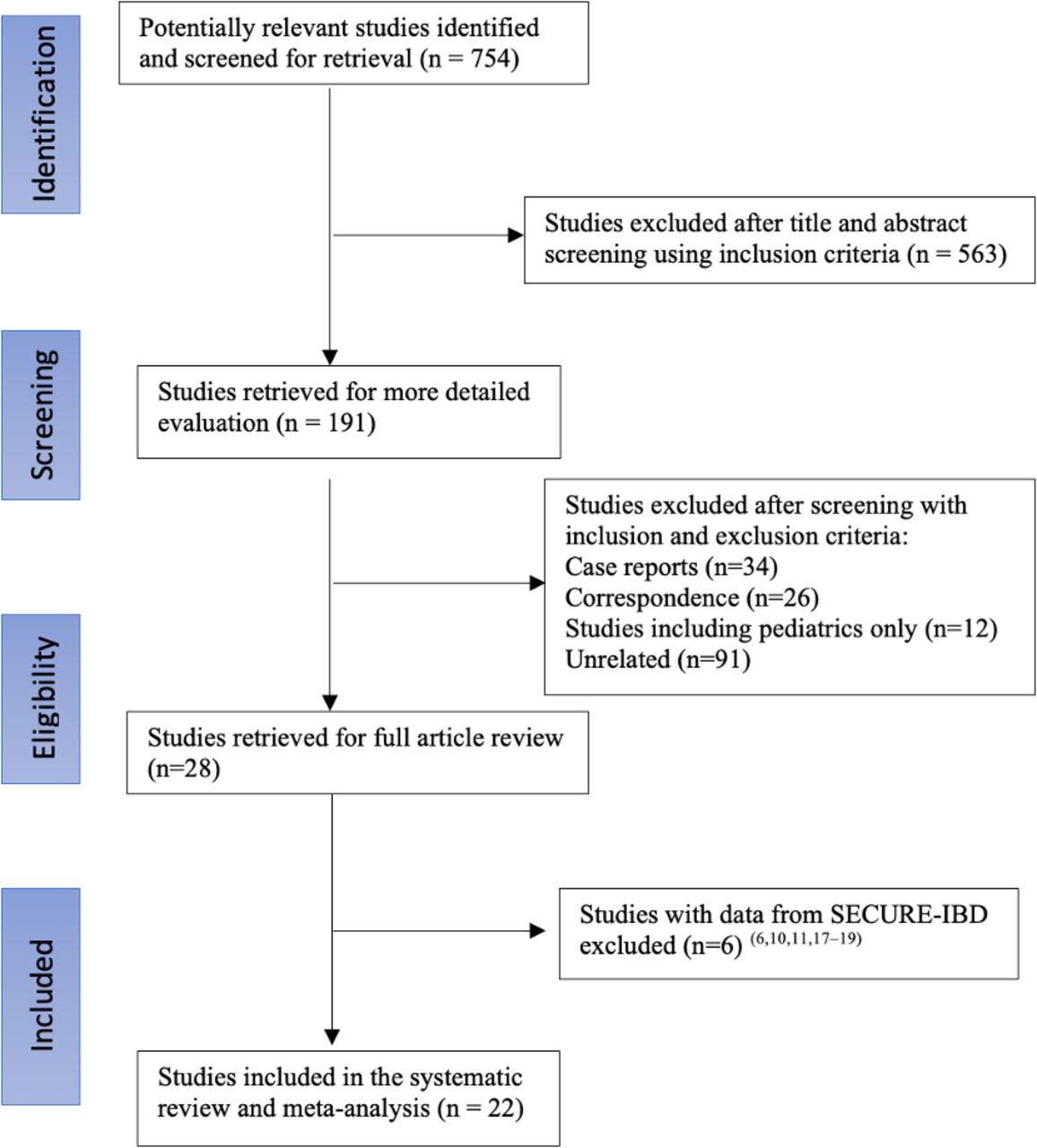
PRISMA flow chart outlining the search process for selecting the studies included in this systematic review with meta-analysis.
Summary of included studies and patients’ characteristics
Primary outcome
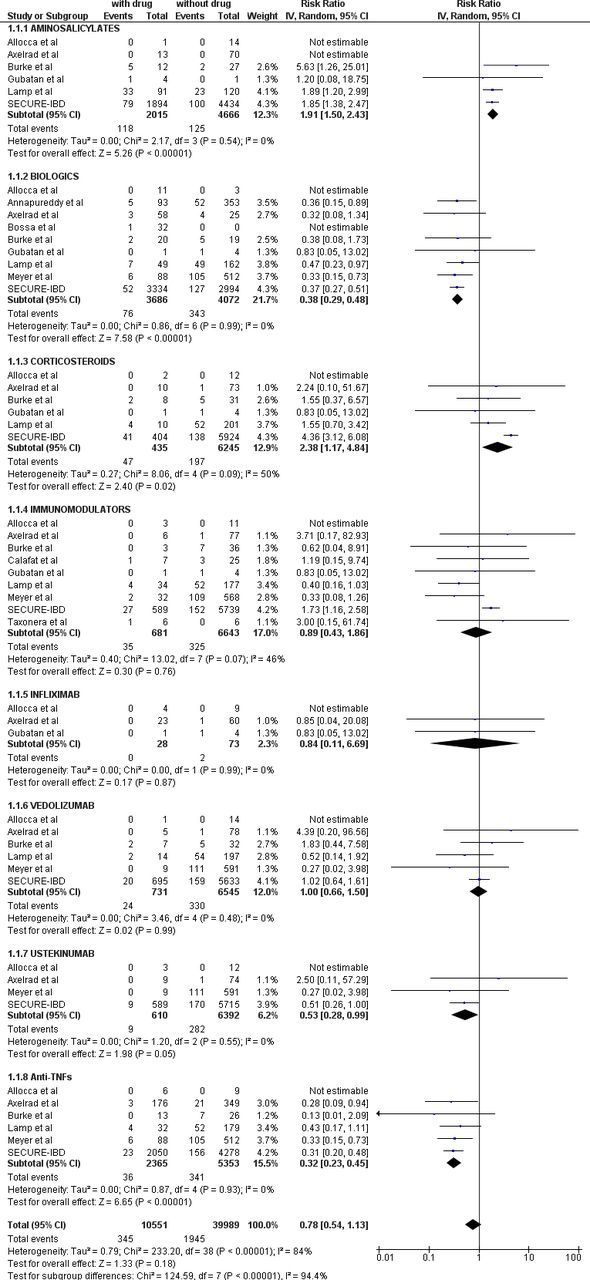
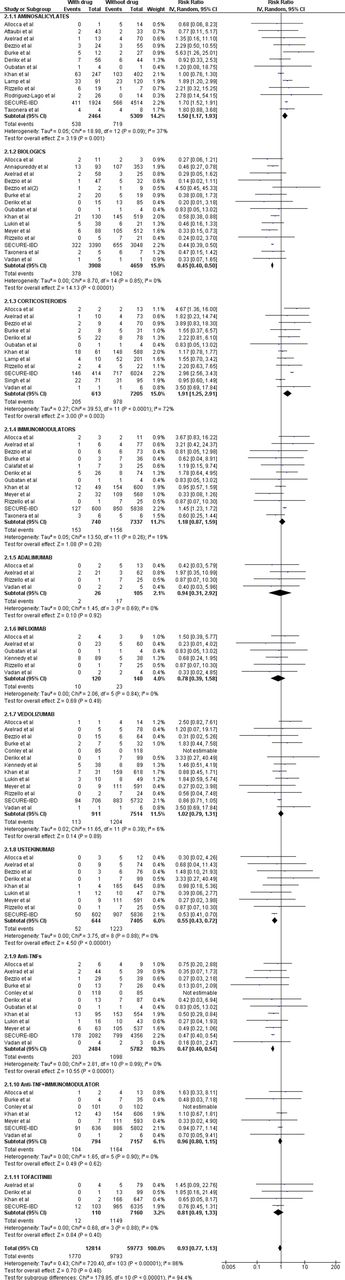
When comparing patients with IBD infected with SARS CoV-2 receiving corticosteroids with patients who did not receive corticosteroids, the analysis showed significantly higher risk of severe COVID-19 with a RR of 1.91 (95% CI 1.25 to 2.91, p=0.003). Patients receiving 5-ASA had increased risk of severe COVID-19 compared with those not receiving 5-ASA (RR 1.50 (95% CI 1.17 to 1.93, p=0.001)). Whereas immunomodulators alone (RR 1.18 (95% CI 0.87 to 1.59, p=0.28)) or in combination with anti-TNFs ((RR 0.96 (95% CI 0.80 to 1.15, p=0.63)), were not associated with severe outcomes. Similarly, in patients using adalimumab ((RR 0.94 (95% CI 0.31 to 2.92, p=0.92)), infliximab ((RR 0.78 (95% CI 0.39 to 1.58, p=0.49)), vedolizumab ((RR 1.02 (95% CI 0.79 to 1.30, p=0.90)), or tofacitinib (RR 0.81 (95% CI 0.49 to 1.33, p=0.40)), no significant association was observed between their use and severe outcomes. Interestingly, the use of biologics (RR 0.45 (95% CI 0.40 to 0.50, p<0.00001)) was associated with favourable outcomes. Specifically, anti-TNFs (RR 0.47 (95% CI 0.40 to 0.54, p<0.00001)) and ustekinumab (RR 0.55 (95% CI 0.43 to 0.72, p<0.00001)) were associated with significantly lower risk of severe COVID-19 (figure 2).

Forest plot showing the risk of severe COVID-19 in patients taking 5-ASA, immunomodulators, steroids, tofacitinib, and biological agents.
Sub-analyses
ICU admissions
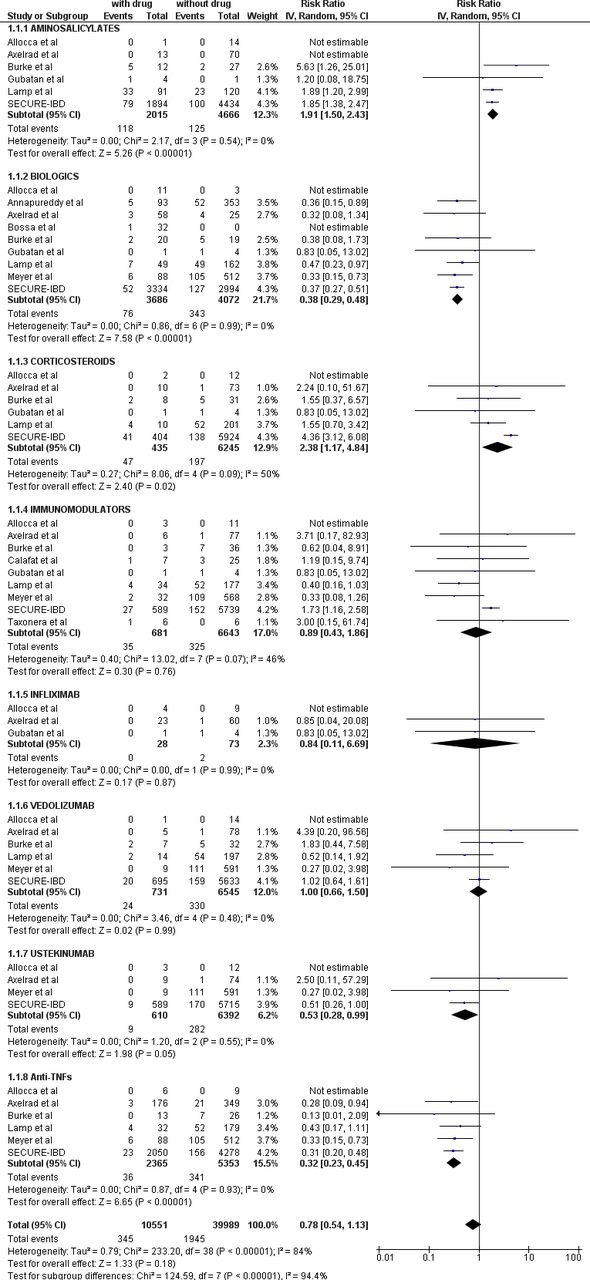
The number of patients in the sub-analyses was different among the drug groups. The number of patients included in this sub-analysis who were receiving 5-ASA was 2015, whereas the numbers of patients receiving corticosteroids and immunomodulators were 435 and 681, respectively. The total number of patients receiving biologic therapies was 3686. Specifically, 2365 patients were taking anti-TNF monotherapy; 28 patients were taking infliximab. Finally, the numbers of patients receiving vedolizumab and ustekinumab included in this sub-analysis were 731 and 610, respectively. The risk of ICU admission was significantly higher in patients with IBD taking corticosteroids compared with patients who did not (RR 2.38 (95% CI 1.17 to 4.84, p=0.02; I2=50%)). The risk was also higher in patients taking 5-ASA (RR 1.91 (95% CI 1.50 to 2.43, p<0.00001; I2=0%)). Conversely, the use of biologics (RR 0.38 (95% CI 0.29 to 0.48, p<0.00001; I2=0%)) was associated with lower risk of ICU admission. Specifically, anti-TNFs (RR 0.32 (95% CI 0.23 to 0.45, p<0.00001; I2=0%)) and ustekinumab (RR 0.53 (95% CI 0.28 to 0.99, p=0.05; I2=0%)) were protective against severe COVID-19 outcomes. No difference was observed in the risk of ICU admission in patients receiving immunomodulators (RR 0.89 (95% CI 0.43 to 1.86, p=0.76; I2=46%)), infliximab (RR 0.84 (95% CI 0.11 to 6.69, p=0.87; I2=0%)), or vedolizumab (RR 1.00 (95% CI 0.66 to 1.50, p=0.99; I2=0%)) (figure 3).
Forest plot showing the risk of intensive care unit (ICU) admission in patients taking 5-ASA, immunomodulators, steroids, and biological agents.
Mortality
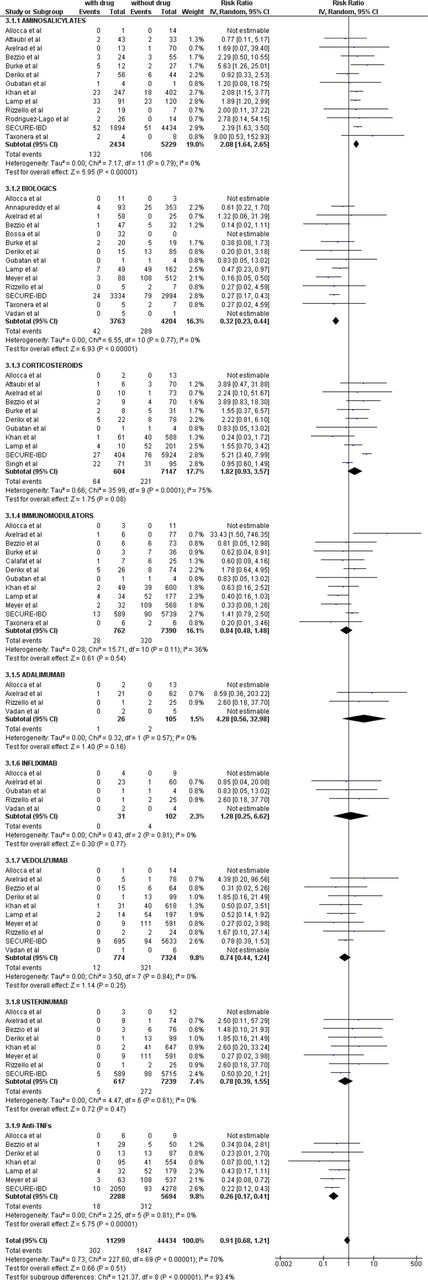
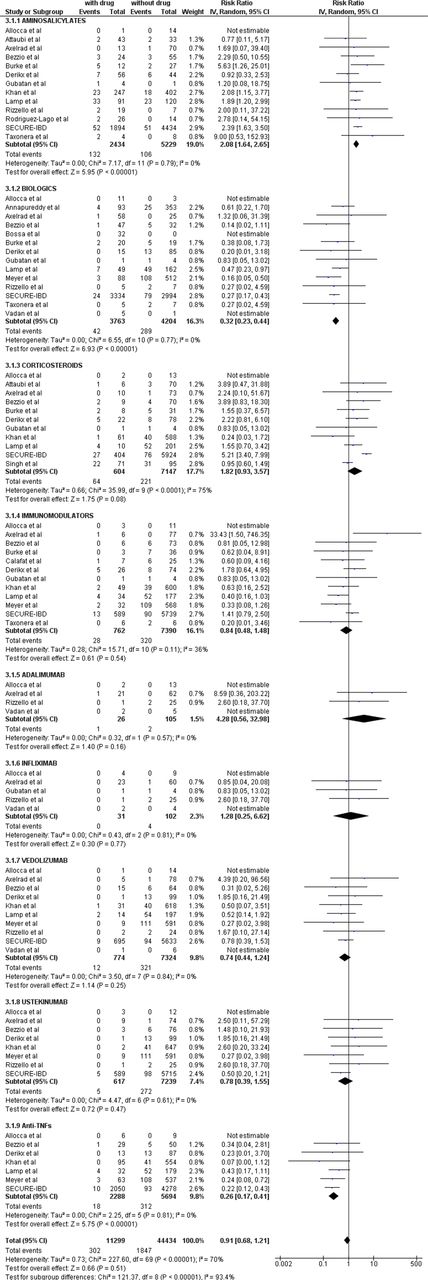
The number of patients who were eligible to be included in this sub-analysis was different among the drug groups. The number of patients included in this sub-analysis who were receiving 5-ASA was 2434, whereas the numbers of patients receiving corticosteroids and immunomodulators were 604 and 762, respectively. The total number of patients who were receiving biologic was 3763. Specifically, 2288 patients were taking anti-TNF monotherapy, 26 patients were taking adalimumab and 31 patients were taking infliximab. Finally, the numbers of patients receiving vedolizumab and ustekinumab included in this sub-analysis were 774 and 617, respectively. The risk of mortality in patients with IBD taking 5-ASA was significantly higher than patients not taking 5-ASA (RR 2.08 (95% CI 1.64 to 2.65, p<0.00001; I2=0%)). No difference was observed in risk of mortality between patients with IBD who received immunomodulators and those patients who did not (RR 0.84 (95% CI 0.48 to 1.48, p=0.54; I2=36%)). Furthermore, corticosteroid use was not associated with mortality (RR 1.82 (95% CI 0.93 to 3.57, p=0.08; I2=75%)). Mortality was significantly lower in patients taking biologics (RR 0.32 (95% CI 0.23 to 0.44, p<0.00001; I2=0%)); specifically, in patients taking anti-TNFs the RR was 0.26 (95% CI 0.17 to 0.41, p<0.00001; I2=0%). Finally, neither the use of vedolizumab nor ustekinumab were associated with mortality. (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot showing risk of mortality in patients taking 5-ASA, immunomodulators, steroids, and biological agents.
Heterogeneity assessment, risk of bias, and quality of studies
Median mNOS score was 4, with scores ranging from 4 to 6 (see online supplemental table 2). In terms of risk of bias, most studies were judged to have low risk of bias using the Risk of Bias in Non-Randomized Studies – of Interventions (ROBINS-I) tool, while three studies had moderate risk of bias (see online supplemental table 3). Using random-effect model, heterogeneity I2 ranged from 0% to 72%. In all studied medications, heterogeneity was low (less than 30%) except for corticosteroids where it was medium (72%).
Publication bias
Online supplemental figure 1 shows a funnel plot of publication bias. Based on visual examination of the plot, symmetrical distribution of the studies on the funnel plot suggests low risk of publication bias.
Discussion
In this systematic review and meta-analysis, we analysed the risk of severe COVID-19 in patients with IBD who are receiving different medical therapies. Our analysis showed that the risk of severe disease significantly increases in patients taking 5-ASA and corticosteroids. Conversely, tofacitinib, vedolizumab, immunomodulators alone or in combination with anti-TNFs were not associated with any negative outcomes. In addition, anti-TNFs and ustekinumab were associated with favourable outcomes.
Surprisingly, the current study demonstrated an increased risk of severe COVID-19 in patients taking 5-ASA. As 5-ASA has very mild immunosuppressive activity, further studies are required to explore this association. One study found that compared with methotrexate monotherapy, sulfasalazine was associated with higher risk of death (OR 3.60, 95% CI 1.66 to 7.78) in patients with rheumatic diseases.20 Recent data from the SECURE-IBD registry demonstrated that 5-ASA use was associated with severe COVID-19 outcomes in univariable but not in multivariable analyses.17 However, individual patient-level data were lacking. Factors controlled for in multivariable analyses were age, sex, race, disease type, medications used, disease activity, comorbidities, and when patients were enrolled in the registry. Although it is unclear if any specific factor explained the finding, the use of these together provide a possible explanation for this surprising finding. Not being an immunosuppressive drug, and being widely available and less costly than biologics, 5-ASA might be used more often in more vulnerable populations, such as the elderly, patients with low socioeconomic status, or patients with multiple comorbidities. In addition, patients using 5-ASA may have been under-treated, resulting in more active intestinal inflammation. For example, a significant proportion of patients with CD were on 5-ASA, despite data demonstrating similar efficacy to placebo.21 22 Furthermore, 5-ASA use in moderate to severe ulcerative colitis or Crohn’s disease is less likely to control luminal inflammation and active IBD could be the driver of the observed adverse outcomes in patients on 5-ASA. Finally, patients on biologic therapies are usually followed more often by their treating physicians and get tested for SARS-CoV-2 more frequently than those on 5-ASAs leading to reporting bias.23 Some of the included studies cited few other reasons for the increased risk of severe COVID-19 in patients with IBD taking 5-ASA. Meyer et al24 postulated that closer follow-up of patients taking other therapies such as biologics by physicians and over-reporting of most serious outcomes led to the introduction of several biases. It is important to recognise that some studies found that the risk of severe COVID-19 is associated with older age (>65 years), cardiovascular, pulmonary, and renal diseases.25–27 It is likely that these factors are associated with severe COVID-19 more than 5-ASA use itself.
Another finding of this meta-analysis was that corticosteroids use was associated with an increased risk of severe COVID-19, while the use of biologics was associated with a reduction in these outcomes. This finding has been described in the literature before with other types of infection.28 29 The strong positive association between systemic corticosteroid use and our severe COVID-19 outcomes is consistent with extensive prior literature in IBD. Brenner et al found that corticosteroids use but not anti-TNFs were associated with severe COVID-19.11 It is important to note that in our sub-analysis, we found that corticosteroids use was associated with ICU admission but not mortality.
The RECOVERY trial30 reported mortality benefits in patients with severe COVID-19 treated with dexamethasone. It is important to understand that the impact of corticosteroids depends on the stage of infection.28 It is likely that the degree of the benefit of corticosteroid treatment is related to the level of disease severity. At the onset of infection, corticosteroids may weaken the immune response and delay viral clearance; however, during the advanced stage of severe COVID-19, the blunting of the hyperimmune response by corticosteroids improves prognosis and reduces mortality.31 Furthermore, available evidence suggest that the benefits of corticosteroids depends on other factors such as level of respiratory support.32 Results from different studies31–33 indicate that among patients requiring low-flow oxygen, corticosteroid use did not lower mortality or ICU admission. However, patients with advance level of respiratory support requirement, such as invasive mechanical ventilation, benefited the most in terms of reduction in mortality.34 In addition, one study found that critically ill patients with COVID-19 were five times more likely to get corticosteroids compared with non-ICU patients.35 Therefore, the aforementioned reasons present a possible explanation of the association of corticosteroid use with ICU admission but not mortality.
Finally, the level of heterogeneity found among the studies in the corticosteroid group can be explained by the inclusion of large, heterogenous, and diverse group of patients receiving corticosteroids. It is unlikely that all patients will benefit from corticosteroid use, for some receiving corticosteroids might lead to harmful effects. The duration of corticosteroids use could also have a considerable impact on heterogeneity. Other circumstances that may give rise to clinical heterogeneity include differences in selection of patients, severity of disease, and management.36 For example, patients with acute exacerbations of their IBD may have got infected with COVID-19 while being on corticosteroids for couple of weeks leading to worse COVID-19 outcome. On the other hand, patients with IBD who were not on corticosteroids and were admitted to ICU with severe COVID-19 were given steroids for a shorter period of time to improve their outcome. Therefore, the diversity of the included patients who received corticosteroids can contribute to the level of heterogeneity observed.
The present data are consistent with previous data showing immunomodulators are not associated with an increased risk of severe infection. For example, data reported on 1099 patients from China did not observe immunomodulator use as a risk factor for severe disease.37 Consistent with this, an Italian prospective observational cohort of 79 patients with a diagnosis of IBD and COVID-19 found no association between thiopurine and COVID-19–related pneumonia.38 This might be explained by the cytokine storm syndrome, which predisposes patients to a severe form of COVID-19.39 Patients with IBD on immunomodulatory treatments, particularly those who directly interfere with cytokine action and production, may be protected even against the severe forms of COVID-19.
Our study also showed that biologics, without immunomodulators, have a protective effect against severe COVID-19 in IBD. Previous studies11 40 41 suggested possible rationale for the benefits of biologic therapies, particularly anti-TNFs, in COVID-19. This can be explained by the mechanism of action of these medications. Anti-TNFs inactivate the proinflammatory cytokine TNF by direct neutralisation, thus resulting in suppression of inflammation.42 This suppression interferes with the cytokine storm mentioned previously and prevents need for hospitalisation or ICU admission.43 Importantly, this was consistent with anti-TNF agents, and ustekinumab but not vedolizumab. Ustekinumab binds to the p40 subunit of interleukin (IL)−12 and IL-23, which ultimately prevents cell signalling and cytokine production. This again interferes with systemic inflammation and prevents severe disease by stopping multiorgan failure that can lead to death in patients infected with SARS-CoV-2.44 On the other hand, vedolizumab is gut specific and does not significantly affect systemic immune reaction.18 Finally, as disease activity is associated with worse COVID-19 outcomes,38 it is possible that use of effective agents, such as biologic therapy, reduces risk by reducing intestinal disease activity.
With regards to tofacitinib use in patients with IBD infected with SARS-CoV-2, we found that tofacitinib was not associated with severe disease. A recent randomised controlled trial found that tofacitinib reduces the incidence of death.45 Another study, which included 86 patients with COVID-19 in the USA, suggests that being on tofacitinib did not appear to increase the risk of developing SARS-CoV-2 features that led to serious infection or death.46 Finally, a study by Agrawal et al reported no significant differences between tofacitinib-treated patients and other patients in the occurrence of hospitalisation or admission to the ICU.10
Finally, the most recently published studies recruited patients up to March 2021 and did not report vaccination status among the included patients. It would be interesting to know if vaccination would alter the outcomes of COVID-19 in relation to IBD medications.
This systematic review has several clinical implications. It provides guidance regarding the continuation of most IBD medications in the setting of the COVID-19 pandemic. Our study showed that continuing biologic therapies, small molecule inhibitors, and immunomodulators, alone or in combination with anti-TNFs, are safe and should not be discouraged. Furthermore, initiation of corticosteroids should be minimised in areas with high prevalence of SARS-CoV-2 infection. If needed, it should be continued and tapered down in the shortest period, weighing benefits and risks. This practice is also recommended by both the British Society of Gastroenterology and the International Organization for the Study of Inflammatory Bowel Diseases guidelines.47 48 Finally, as discussed previously, active IBD disease has been shown to worsen COVID-19 outcome; therefore, clinicians should continue to treat patients targeting clinical and endoscopic remission. Clinicians should also encourage patients to comply with their medications and clarify any misgivings patients may have regarding the safety of their IBD medications.
This study is the first to include summary data on individual biological therapies, anti-TNF combination therapy, and small molecule inhibitors. The current study summarises significantly increased available data overall and for individual medications. A previous systematic review and meta-analysis earlier in the pandemic,49 which included studies up to July 2020, also found that both 5-ASA and corticosteroids, but not immunomodulators, increased the risk of severe disease in patients infected with SARS-CoV-2. With a larger sample size, our study found that corticosteroids were associated with ICU admission, but not mortality. Furthermore, the inclusion of more than 10 000 patients with IBD infected with SARS-CoV-2 gives more precise estimation of the risk of severe COVID-19 in this patient population. Our study limitations include the observational nature of included studies with risk of confounding and selection bias. Furthermore, the majority of patients included in our study were extracted from the SECURE-IBD database. Even though the validity of the data is reinforced by the physician-reported nature of this database, it is still subject to reporting bias, which may lead to documentation of the more severe cases that come to the attention of healthcare providers, while the milder cases may remain undiagnosed or underreported. In addition, patient-level data were lacking, and insufficient data existed for meta-regression analyses to adjust for confounding. Larger prospective studies are necessary to validate the findings of our study, to ascertain which risk factors play significant roles in causing severe COVID-19 outcomes, and to stratify patients by different factors, including age, disease activity, and socio-economic assessments of the patients.
Conclusion
In patients with IBD, the risk of severe COVID-19 is higher among patients receiving corticosteroids. Corticosteroid use was associated with ICU admission but not mortality. The risk is also higher among patients receiving 5-ASAs. However, patient-level data were lacking and insufficient data existed for meta-regression analyses to adjust for confounding. In contrast, tofacitinib, vedolizumab, immunomodulators alone or in combination with anti-TNFs were not associated with severe disease. Finally, anti-TNFs, and ustekinumab were associated with favourable outcomes.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
FA and RB are joint first authors.
Twitter @drmohamadshehab
Contributors FA: acquisition, analysis, and interpretation of data, drafting the article. RB: analysis and interpretation of data, drafting the article. IA: acquisition and analysis of data. AC: interpretation of data, drafting the article and revising it critically for important intellectual content. MS: conception and design of the study, analysis and interpretation of data, drafting the article and revising it critically for important intellectual content. He is also responsible for the overall work as a guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.