Article Text

Abstract
Background and aims Inflammatory bowel diseases (IBDs) and colorectal cancer have an increased impact on the Lebanese population’s morbidity and mortality. This study evaluated the situation of IBD and colorectal cancer at a tertiary hospital centre in Lebanon.
Methods 1007 patients underwent colonoscopy over a period of 12 months by qualified physicians. 91 patients were excluded from the study. Biopsy results were divided into normal versus abnormal colonic tissue. The abnormal section was further subdivided into number of polyps, IBD, dysplasia and cancer.
Results Out of 916 individuals included, 61 cases of Crohn’s colitis (CC) (6.7%) and 24 cases of ulcerative colitis (UC) (2.7%) were identified. A total of 92 cases of colorectal cancer (10.04%) were also identified. There was a slight male predominance in both groups of IBD without any statistical significance. One statistical significance was reported in favour to age<50 years in both IBD groups with a mean age of 37.9±9.7 years and 34.4±6.4 years for CC and UC, respectively. The incidence of granuloma in the CC group was 8.9% without any correlation compared with age or gender. No correlation was made between colorectal cancer and the existence of any IBD type. The data showed that age >50 years and male gender significantly correlate with an increased incidence of precancerous and cancerous polyps in the colon. They significantly correlate with adenocarcinoma. The estimated incidence of colorectal cancer, CC and UC was 54.1, 35.8 and 14.1 per 100 000, respectively, with a denominator of 169 959 patients per year.
Conclusion Within the limitations of this study, the incidence of colorectal cancer and IBD falls in the high range compared with similar European and American studies. Our data are biased because of the tertiary centre setting but they can be considered as base for further investigations.
- adenocarcinoma
- colonic diseases
- ibd
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Colorectal cancer is considered among the three main causes of mortality and morbidity in Lebanon based on the Lebanese cancer registry.1 Studies have shown that appropriate screening has led to a significant decrease in the incidence of colorectal cancer and its mortality over the last 25 years in developed countries.2 Studies have demonstrated the capacity of screening to detect precancerous lesions before they become cancerous and spread in other tissues. 2–4 It led to significant reduction in mortality, morbidity and economic burden of the disease in those countries. These facts are backed by data showing an increase in 5-year survival rate when cancer is discovered at early stages, showing up to 95% survival when it is diagnosed at stage I and just above 10% when diagnosed at stage IV.5 6
Moreover, it would be of great importance to mention that the Lebanese society is at increased risk to develop colorectal cancer.1 This high risk is linked to many factors such as high-fat diet, sedentary lifestyle, smoking habits and relatively high alcohol use.7 The high rate of interfamilial marriage also poses an increased risk factor to develop colorectal cancer in this population, especially that many genes have been implemented with the occurrence of the disease.
On the other hand, inflammatory bowel diseases (IBDs), mainly Crohn’s colitis (CC) and ulcerative colitis (UC), are linked to an increased risk for development of colorectal cancer compared with the general population.8 Actually, death related to colorectal cancer in patients with IBD accounts for >10%. It would be also of high importance to note the diphasic age peak for IBD presentation (15–30 years of age; 50–80 years of age), which eventually leads to lower the mean age of colorectal cancer associated to IBD.9 Thus, the surveillance and management of dysplasia in IBD is highly recommended in order to reduce future development into colorectal cancer especially that most of them are resected endoscopically. A cohort study conducted in 2007 in Lebanon, reported that the prevalence of IBD in a representative sample is similar to that found in an intermediate prevalence range compared with studies conducted in developed countries.1 Therefore, the need to evaluate and monitor this entity is of high importance in order to properly evaluate the incidence of colonic disease in the Lebanese population.
Based on the American College of Physicians (ACP), colonoscopy is considered to be the gold standard method for colonic diseases surveillance.2 3 It can detect IBDs, precancerous and cancerous polyps, non-polypoid cancer in addition to other pathologies.10 11 Consequently and for the above-mentioned reason, colonoscopy guidelines were developed and used worldwide in an attempt to have an adequate surveillance and decrease the incidence and prevalence of many colonic diseases.9–11
The importance of colonoscopy is highlighted in the surveillance and early detection of colonic diseases.9–11 In Lebanon, such as in many developed countries, colonoscopy is used as a tool to assess colonic diseases.1 To the extent of our knowledge and at the time of writing, studies are yet to be performed that analyse data retrieved from colonoscopies in Lebanon. The present study evaluates the current situation of colonic diseases at a private practice in a tertiary hospital centre in Lebanon over a period of 12 months. Furthermore, the study correlates and compares its results with national as well as international data.
Materials and methods
Sampling
Data were retrospectively collected from a private practice at a tertiary hospital centre in Lebanon. A total of 1007 patients underwent colonoscopy with biopsy (random vs polyp removal biopsy) by qualified physicians over a period of 12 months (figure 1).
Inclusion criteria
The ACP guidelines were followed as indication for colonoscopy. The criteria followed were any of the following findings: age>50 years, history of hematochezia or melena, change in bowel habits and family history of IBD or colorectal cancer.
Exclusion criteria
Patients being already diagnosed with IBD or any colorectal cancer were excluded from the study. Control colonoscopies were excluded also from the analysis of data. Colonoscopies without caecal intubation were also excluded from the study in addition to those with an Aronchick scale grade higher than 2 over 5. The final number included in the study is 916 patients.
Informed consent
All patients participating in this study signed an informed consent allowing the using and analysis of the data retrieved from their colonoscopy with anonymity done by translation of names into binary techniques for scientific purposes
Colonoscopy preparation
The evaluation of colonoscopy preparation was recorded based on the Aronchick scale with 1 over 5 considered as adequate and 5/5 as inappropriate for evaluation. All patients were prepared using the alpha PEG agent as osmotic agent 24 hours prior to the onset of colonoscopy.
Colonoscopy procedure
Colonoscopy took place in a tertiary hospital centre with highly trained staff. The average withdrawal time was 7.5 min with the shortest at 6 min. All patients were sedated, put in lateral decubitus position with flexed knees. No complications were noted during all the procedures done. No post-colonoscopy complications were faced also. During the colonoscopy, random biopsies (total of 20) were taken from the colon with a systematic approach from the rectum, sigmoid, left colon, transverse, right colon and ileocecal valve if no polyps were identified. Polypectomy was performed for polyps below the size of 10 mm and then sent to pathology. Polyp’s biopsy was done for those >10 mm in size. Biopsy was taken from erythematous or edematous area in the colon. All biopsies were put in 10% formaldehyde and sent to the pathology department for further analysis.
Pathology analysis
Biopsy samples taken during colonoscopy were processed in blocks, and multiple micro-cut were taken from each block for the same patient and stained with H&E stain. Two different pathologists looked at the slides and results were agreed on before writing the final report.
Age, gender and results of biopsy from pathological reports were retrieved. Results were divided based on normal colonic tissue versus abnormal colonic tissue. The abnormal section was further subdivided into number of polyps, IBD (CC vs UC), dysplasia (low and high grade) and cancer.
Statistical analysis
All data were analysed using a statistical software package (SPSS V.13.0). Student’s t-tests and χ2 analysis were performed in order to compare independent variables in question between each other and depend ones. The study protocol was reviewed and approved by the institutional review board of Saint George University Medical Center.
Results and discussion
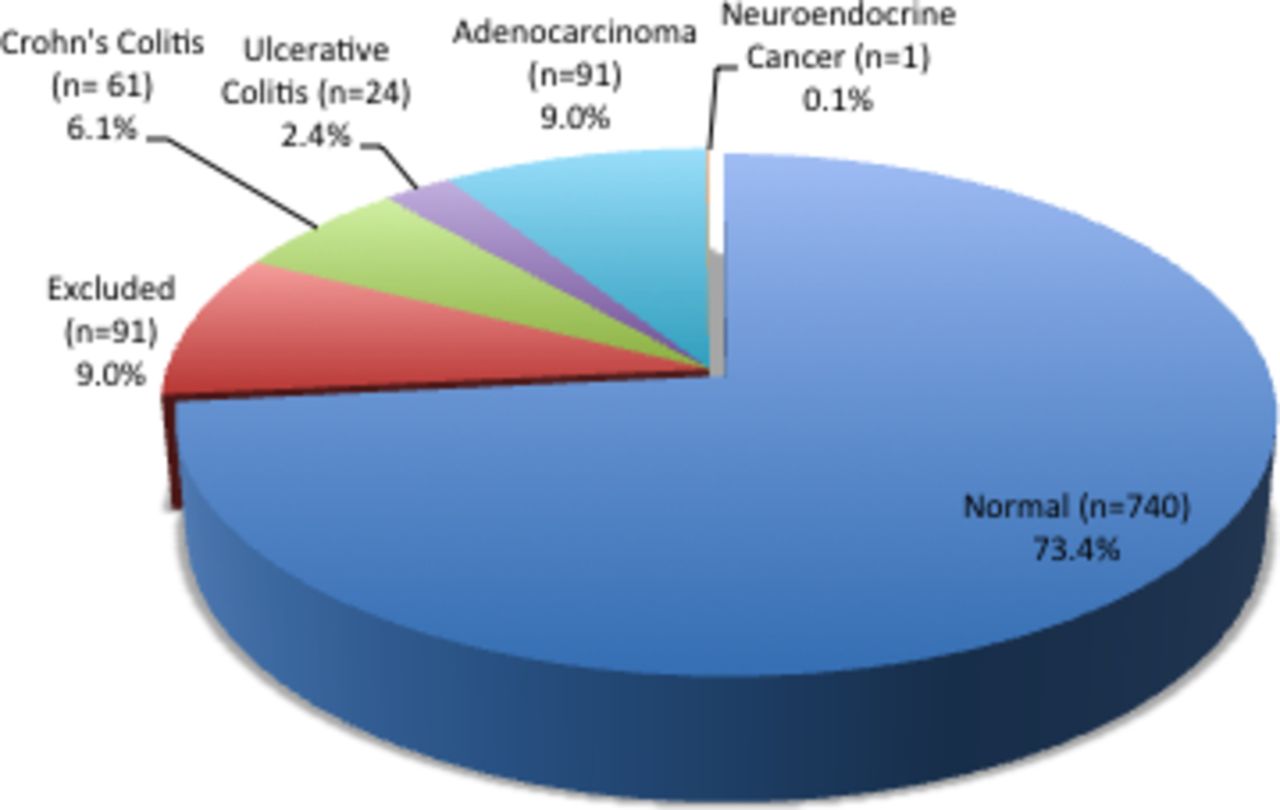
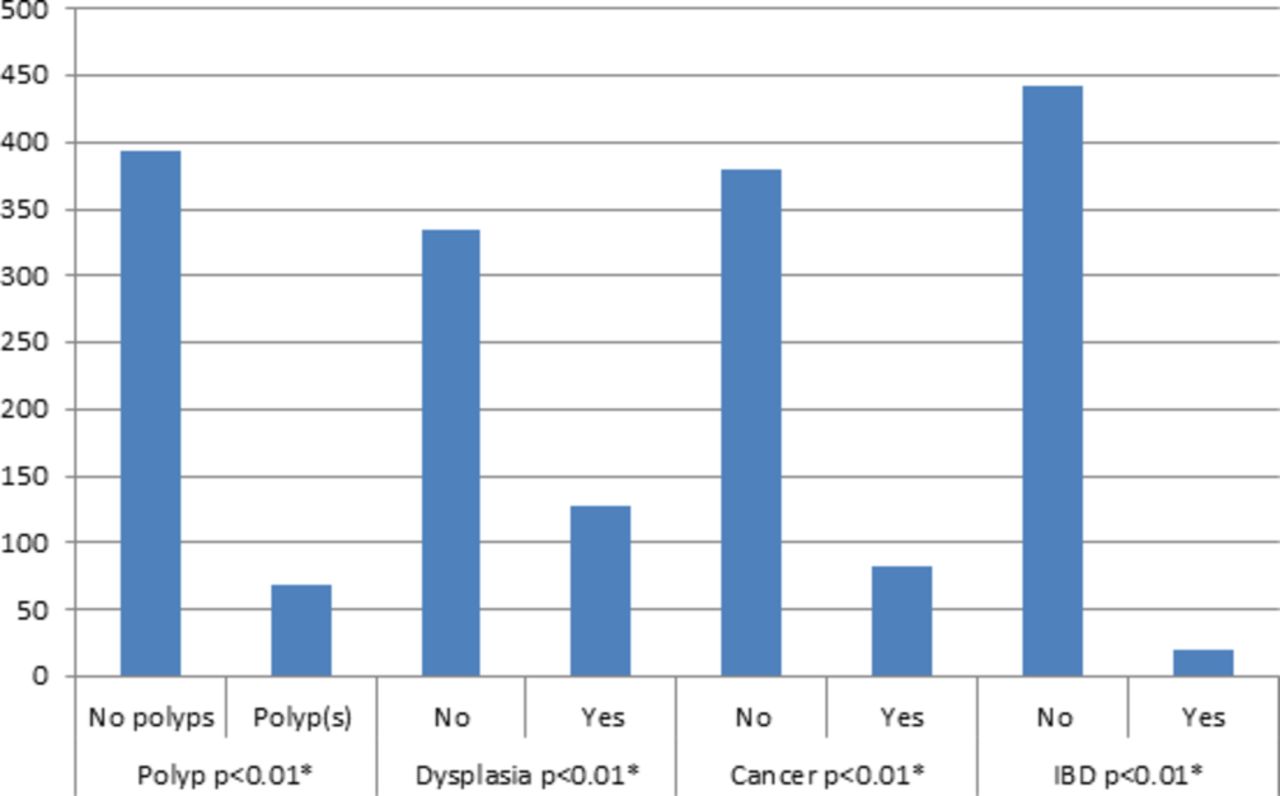
The total number of patients was 1007; 91 patients were excluded from the study (exclusion criteria, figure 1). The analysis of the results retrieved from the 916 individuals selected in the study reported a total of 91 cases of adenocarcinoma leading to an incidence of 9.9% (table 1). The total number of all cancer types including one case of neuroendocrine was 92 cases, leading to a total of 92 cases of colorectal cancer reflecting 10.04%. No gender predominance was noted in this group (table 1). The data showed that age >50 years significantly correlate with an increased incidence of precancerous and cancerous polyps in the colon (p < 0.01). Polyps are more frequent in male gender with a significant correlation (p < 0.01). The occurrence of polyps notably correlates with adenocarcinoma (p <0.01) (table 3). Just one case of neuroendocrine tumour was identified in our sample.
No correlation was made when comparing the incidence of colorectal cancer in the group of patients with or without IBD (p=0.871). Recent data have supported the regular surveillance for colorectal cancer in patients with pre-existing IBD.12 13 These data also show that the majority of dysplasia in those patients correlates with a polypoid feature.12 13 In addition, they show no increase in the risk of transformation into malignancies compared with the general population. However, Sungupta et al concluded that frequent colonoscopy is recommended in patients with IBD in order to reduce the risk of malignant transformation of dysplasia.9 The question remains in the frequency of surveillance that should be followed.11 14

Distribution of colonoscopy results.
The results show 61 cases of CC and 24 cases of UC (table 1). There was a slight male predominance in both groups of IBD without any statistical significance (p=0.741). One statistical significance (p <0.01) was noted in favour to age<50 years in both IBD groups with a mean age of 37.9 ± 9.7 years and 34.4 ± 6.4 years for CC and UC, respectively (table 2). The incidence of granuloma in the CC group was 8.9% without any correlation compared with age or gender (table 3).
Descriptive table of the study
Testing-depended variables of polyp, dysplasia, cancer and inflammatory bowel disease (IBD)with the independent variable of age >50 years (n= 462 patients > 50 years)
Comparison by gender
Age is the factor mostly linked and studied to colonic diseases.5 14 Previous studies and meta-analysis have shown a significant increase in the rate of colorectal cancer after the age of 50 with at the highest one reached after the age of 85.15 This factors plays an important role in the development of colorectal caner after the age of 50 as seen also with our population showing a p<0.01, making our data in accordance with other published data, but when it comes to the IBDs, age factor has less implications on our population. This has been also reported by Abdul-Baki et al in 2007 on the Lebanese population at another tertiary centre.1 They show no correlation between age and CC and between age and UC. Our data fall also in that same prospect and show no correlation between age and any of the IBD diseases. But it is important to highlight the change of prevalence among CC and UC when our study is compared with Abdul-Baki’s study and notice an increased prevalence of CC; this shift is also noticed in other international studies where the prevalence of CC is increasing compared with a moderate decrease to the prevalence of UC.12 13 A small percentage of our population shows polyposis features or colorectal cancer before the age of 50 without significance (p>0.1); this fact can be linked more to genetic factors and mutated genes, which predispose to early manifestation of the disease (figure 2). All these data when gathered highlighted the importance of systemic colonoscopy for people above the age of 50 years and for those with alarming feature (diarrhoea, hematochezia and alternation of bowel movement) before the age of 50 years for an early detection of colonic disease.

Comparison between age >50 years and presence of polyps, dysplasia, cancer and inflammatory bowel disease (IBD). Note that all four parameters significantly correlate with the independent variable of age>50 years. *Statistically significant results.
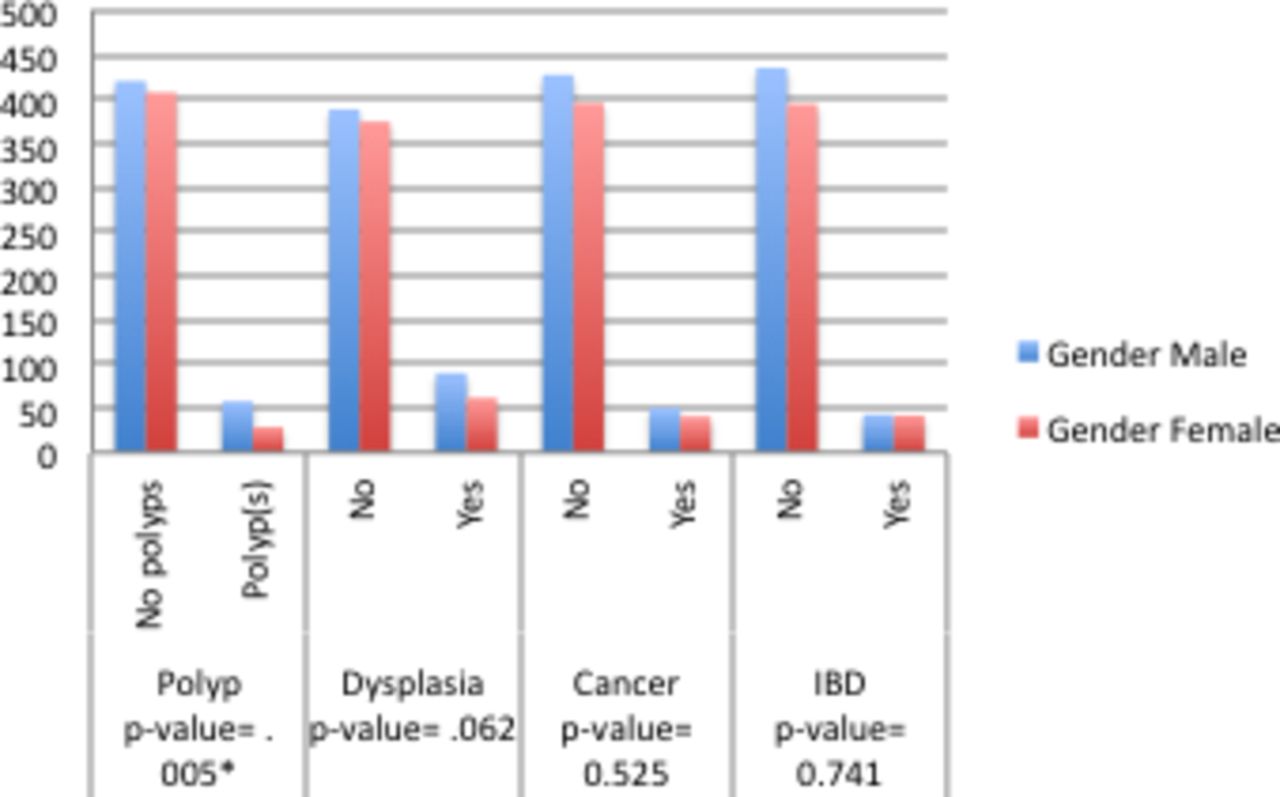
Gender comparison is also helpful because studies have shown that men are at an increased risk to develop colorectal cancer compared with women. A previous meta-analysis (total of 924 932 cases) found a relative risk of 1.83 with a CI lying between 1.69 and 1.97.16 Our data are also in accordance with the stated data; male gender was found to be significantly associated with presence of polyps with a p value <0.001 (figure 3). Knowing that polyploidy features predispose to colorectal cancer, links and correlation can be drawn between age and development of colorectal cancer in the future.12 16 This link between gender and IBD was not found in our sample, and this is also compatible with most of the published data, which found non-consistent results for this topic. This was also the same case in the study performed by Abdul-Baki et al in Lebanon in 2007 where they were not able to find any link between age and IBD. This study concludes that the prevalence of IBD is not linked to age-specific determinant and it falls in the intermediate range of that reported in North America and Europe.9 12 13 These data can be used to backup argument that a systemic approach for colonoscopy is needed specifically in the male gender in order to allow early detection of colonic diseases and abnormal features.

{kind=link}
{kind=link}
{kind=link}
Gender comparison in polyps, dysplasia, cancer and inflammatory bowel disease (IBD). Note the significance of male gender for polypoid feature (p<0.01).
Environmental factors such as diet, alcohol and smoking have been studied and linked to increased risk of colonic diseases.17–19 Low fibre, low green vegetables and high red meat diet intake have been correlated with increase incidence of colorectal cancer.20 A meta-analysis of 24 prospective studies found the relative risk of colorectal cancer for the highest versus the lowest intake of red or processed meat in the pooled cohort was 1.22 (95% CI 1.11 to 1.34). In addition, Parkin et al demonstrated in their study ‘Cancers attributable to overweight and obesity in the UK in 2010’ that around 15% of bowel cancer has been linked to obesity.21 They found a relative risk of 1.33 (1.25 –1.42) in obese patients (body mass index (BMI)>30) compared with patients having a normal BMI (BMI<30). In a previous meta-analysis, smoking has been linked to increase risk of colorectal cancer and flares of IBD.22 23 Tsoi et al demonstrate that active smokers have 20% higher risk (CI 1.1–1.3) to develop colorectal cancer than those who have never smoked.18 Fedirko et al. found an overall increase in colorectal cancer of 7% per unit of alcohol consumption daily.17 The Mediterranean diet and mainly the Lebanese one is based on high consumption of red meat; moreover, the Lebanese population tends to be overweight and even obese; this makes the prevalence and incidence of colonic diseases, mainly colorectal cancer and IBD, at the highest range. In a closer view to patients diagnosed with colorectal cancer from our sample, we note that none of our patients follows a vegetarian diet. Furthermore, it is estimated that >50% of the Lebanese population are smokers and this goes up to 80% for secondhand smokers. Taking the factor of diet, alcohol consumption and smoking into consideration, we can draw some reflection related to the risk of colorectal caner and IBD in the Lebanese population. Our population ranges in the high-risk range for colorectal cancer and IBD when it comes to environmental factors. The development of a regular surveillance for those entities is of high value. Thus, regular colonoscopy is highly recommended in our population in a systemic approach in order to avoid the complications of those diseases. Colonoscopies allow diagnosis of colonic disease at an early stage, which will favour better prognosis.
Interfamilial marriage is another factor to take into consideration in the Lebanese population, even if the exact percentage is not known and differs between urban and rural area, but basic demographic visualisations conclude that it is very common. This process increases the incidence of receive genes, which can play a role in the appearance of IBD and colorectal cancer.24 Koss et al have linked the occurrence of IBD to gene mutations in CARD-15 and the polymorphism of the following cytokines: interleukin-10 or tumour necrosis factor-alpha.5 24 25 Moreover, the high prevalence of familial polyposis in the Mediterranean countries as demonstrated in the previous studies compared with other non-Mediterranean countries shows that interfamilial marriage plays an important role in increasing the incidence of colorectal cancer in those countries. Thus, Lebanon being a Mediterranean country falls in this category of countries with high incidence of multitude of identified mutated genes, which predispose to colonic polyps and diseases. In our sample, the data have shown that out of the 91 cases of colorectal cancer 34.3% had a family history (first-degree or second-degree relatives) of various colonic diseases like colonic polyps, colorectal cancer and IBD. In addition, family history of colonic diseases is not important when looked deeply in the category of patients diagnosed with IBD (5.8% and 4.6% for CC and UC, respectively). No genetic studies have been performed on patients with IBD and colorectal cancer in Lebanon for identification of mutated genes such as MLH1 and 6 and CARD-15, thus any effort in this area will give a great understanding of the disease in the Lebanese population and will help improve quality of surveillance in families which are more affected. The development of personalised approach of surveillance in families that are more susceptible for developing IBD and colorectal cancer emerges to be of high importance in the control and surveillance of those diseases.
It will be also helpful to note that we identified up to 20 cases of melanosis coli which when looked back to their history we found a significant high-dose usage of laxatives. Furthermore, 47 cases of abnormal colonic findings were found in our study; the pathology reports of these cases correlate with enteritis or unspecific infection which cannot be classified neither as colorectal cancer nor as any of the IBDs.
Finally, in our study we were able to estimate the incidence of colorectal cancer, CC and UC is 54.1, 35.8 and 14.1 per 100 000, respectively, with a denominator of 169 959 patients per year, representing the total number of patients coming to our tertiary centre. This is an estimate due to tertiary hospital setting mainly and because no data were retrieved from peripheral areas. Thus our data can only be used as a pillar for future studies in order to find the exact incidence of colonic disease in the Lebanese population. Needless to say, the necessity to establish a national survey and national registry is a necessity, which allows better monitoring and surveillance of colonic diseases. Our estimated incidences compared with incidences of colonic disease in Europe and North America are found to be in correlation with them, thus putting the Lebanese population at a relatively high risk for developing colonic diseases.11
We as well found a doubling in the incidence of colorectal cancer compared with one Lebanese projection study by Shamseddine et al 26 (54.1 in our study to 21.5—colon and rectum).
Conclusion
Within the limitations of this study, colonic diseases are found in the Lebanese population with a relatively high incidence. Our study, which was conducted in a tertiary hospital centre, reported high-range prevalence of colonic diseases (IBD and colorectal cancer) compared with similar European and American studies. Our data are biased because of the tertiary centre setting but they can be used as base for further prospective investigations regarding risk factors, national epidemiology and genotypes in both colorectal cancer and IBD. Both entities are being linked to increased psychological, social and economic burden in the Lebanese community.
Acknowledgments
Thanks to Ziad Salameh.
References
Footnotes
Handling editor Joseph Lim
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.