Article Text

Abstract
Objectives Segmented filamentous bacteria (SFB) have been detected in a wide range of different animal. Recently, the presence of SFB-like bacteria was shown in biopsies of the terminal ileum and ileocecal valve of both patients with ulcerative colitis and control subjects. The aim of this study was to verify whether PCR methods could be used for the detection of SFB in biopsy of patients with ulcerative colitis and its relationships with the disease stage.
Methods PCR methods were used to identify SFB in biopsies from the terminal ileum of patients with ulcerative colitis, showing that this approach represents a useful tool for the detection of SFB presence and analysis of the bacterial load.
Results Our analysis detected SFB in all faecal samples of children at the time of weaning, and also show that putative SFB sequences are present in both patients with ulcerative colitis and control subjects. Results obtained using real-time quantitative PCR analysis confirm the presence of putative SFB sequences in samples from the terminal ileum of patients with ulcerative colitis and in control subjects.
Conclusions The presence of putative SFB sequence in both patients with ulcerative colitis and control subject suggests that SFB cannot be considered as being uniquely associated with the disease. The second conclusion is that among the patients with ulcerative colitis, a tendency does exist for active disease samples to show higher SFB load, opening new perspectives about possible identification and pharmacological manipulation of SFB-mediated processes for new therapeutic strategy.
- ulcerative colitis
- leum biopsy
- segmented filamentous bacteria
- polymerase-chain reaction
- diagnosis
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Summary box
What is already known about this subject?
The detection of segmented filamentous bacteria (SFB) presence and load is of pivotal relevance to evaluate its role in the pathogenesis of inflammatory and autoimmune human pathologies.
SFB is virtually present in terminal ileum of all the animals, including mouse, rat, chicken and fish.
The presence of SFB in human biopsies has been demonstrated on the basis of a single observation based on optical microscopy.
In human, PCR-based SFB sequences have been detected in faecal samples but its presence in human colon diseases is still unclear.
PCR-based SFB detection has been developed but not applied to human biopsies.
What are the new findings?
PCR-based SFB sequences have been quantified in human biopsies from terminal ileum.
SFB sequences are present in both patients with colorectal ulcerative colitis (RCU) and control subjects.
SFB cannot be considered as being uniquely associated with the RCU pathology.
A possible tendency to be further confirmed on a higher number of patients does exist between SFB load and the activity of RCU disease.
How might it impact on clinical practice in the foreseeable future?
The impact of this study in the clinical practice is related to possible diagnosis, therapeutic treatment and patient stratification of ulcerative colitis during acute phase and remission.
Introduction
Segmented filamentous bacteria (SFB) are Gram-positive bacteria which cannot be cultured with methods available in clinical settings. SFB were discovered in 1849 by Joseph Leidy in the intestines of myriapods and termites and reported as ‘jointed threads’; due to their peculiar shape, Leidy called these bacteria Arthromitus,1 but they are generally simply referred to SFB, a distinct lineage of the Clostridiaceae still pending with respect to precise systematic identification. Subsequently, SFB have been detected in a wide range of different animals including insects, fishes, birds and mammals.2 3 Recently, the interest on SFB has been renewed by two important studies showing that the SFB presence represents a required condition for a specific and coordinated induction of T-cell activity, in particular with respect to T helper 17 (Th-17) lineage and regulatory T-cell responses.4 5 As a result of this novel information, the fascinating hypothesis that these bacteria may play a role in the pathogenesis of autoimmune diseases has been proposed and then confirmed in animal models of multiple sclerosis, autoimmune arthritis and autoimmune diabetes.6–8
The presence of SFB in humans has been described following single observation based on optical microscopy.7 However, clear morphological data remain still scarce in humans.9 10 We have recently shown the presence of SFB-like bacteria in biopsies of the terminal ileum and ileocecal valve of patients with ulcerative colitis and control subjects.11 On the other hand, we and other authors have published several ultrastructural studies demonstrating the presence of SFB in animal models. In mice, rats, chickens and fish, a holdfast segment of SFB is anchored to enterocytes of the specialised epithelium of the Peyer’s patches.12–16 In animal models, SFB appears at the time of weaning, and then expands to become one of the dominant bacteria. Later on, SFB load decreases becoming stable in adult animals probably in relation to age-dependent maturation and activity of the immune system.17 It is difficult to validate similar data in humans, with follow-up studies of children from weaning to adult age. However, Yin et al analysed fresh faecal samples18 and showed that SFB colonisation is age dependent in humans with the majority of individuals colonised within the first 2 years of life, and also that this colonisation disappeared by the age of 3 years. Observations in animal models suggest in any case that SFB are involved in driving the maturation and the differentiation of component of the gut-associated lymphoid tissue in all the animal models.19 20
Since SFB requires very complex in vitro growth conditions,21 this bacterium remains non-culturable with commonly available methods. Recently, SFB genome sequences of rat, mouse and rainbow trout have been published and primers for PCR-based molecular analyses designed by alignment of published 16S rRNA sequences from SFB from mouse, rat and chicken.22–25 Since existing data of the presence and prevalence of SFB in humans are still weak, it is evident that detection of SFB presence and load is of pivotal relevance to evaluating its role in the pathogenesis of inflammatory and autoimmune human pathologies. Considering that the availability of reliable diagnostic methods is a crucial point, we tested and compared primers used in previous PCR studies. The aim of this part of the study was to evaluate whether the use of these putative SFB-specific primers allows performing both qualitative and quantitative PCR (qPCR) analyses in biopsies from the terminal ileum of patients with ulcerative colitis and in subjects without evidence of intestinal disease. To our knowledge, this is the first time in which PCR is performed to identify SFB in biopsies from the terminal ileum instead of in faecal samples. The reason for this choice is related to the importance of studying SFB directly in their colonisation site, where they perform the relative biological activities, that is, in the specialised epithelium and M cells of the Peyer’s patches. Of course, the identification of SFB in patient’s stools by any available technique remains of pivotal importance from a diagnostic point of view (when the pathogenic role of this agent will be clarified). However, it also appears of great interest to show whether the bacteria are present in the areas in which they complete their life cycle and possibly play their pathogenic role. In this preliminary open pilot study, we evaluated the presence and density of SFB in bioptic samples of terminal ileum and ileocecal valve of patients with ulcerative colitis and control subjects by using PCR quantitative and qualitative methods.
Methods
Patients and control subjects
For the purposes of this pilot open study, 10 patients in follow-up for ulcerative colitis previously diagnosed (six males and four females, age 28–70 years) and eight subjects without endoscopic evidence of intestinal disease (four males and four females, age 36–72 years) referred to the Digestive Endoscopy Service of the Hospital of Ferrara and the Sacco Hospital of Milan were recruited prior informed and written consent. According to the protocol approved by the local ethics committee, two biopsies from the terminal ileum and one biopsy from the ileocecal valve have been taken in each subject: one of the biopsies taken from the terminal ileum was in formalin-buffered solution for the routine histopathologic examination, the other two biopsies, one from the terminal ileum and the other one from the ileocecal valve, were immediately frozen at −80°C in suitable cryovials which were then transferred into free nitrogen within a few hours for PCR analysis. Patients with severe ulcerative colitis or relevant clinical conditions, for example, toxic megacolon, tumours, severe liver or kidney failure, and patients who had recently (<3 months) received or who were under treatment with antibiotics or corticosteroids, immunosuppressants or biological agents were also excluded from the study because of the possible influence on SFB presence and density. A control group of healthy subjects, matched for age and sex, recruited among subjects performing colonoscopy for colorectal cancer screening were also recruited, provided they had not taken antibiotics in the previous 3 months and ileocolonoscopy was negative regarding mucosal lesions.
DNA extraction from stool
DNA extraction from frozen stool was performed using Stool DNA Extraction Mini Kit (Fisher Molecular Biology, Trevose, Pennsylvania, USA) according to the manufacturer’s instruction. Briefly, 100 mg of frozen stool was lysed with glass beads, proteinase K and lysis buffer; vortexed; and incubated for 10 min at 70°C. To ensure lysis of Gram-positive bacteria, samples were incubated at 95°C for 5 min under vigorous shaking. Inhibitors and contaminants were removed by buffer system and DNA-binding column. Purified DNAs were eluted with 50 µL of preheated elution buffer. Quality and quantity of DNA were assessed with NanoDrop 1000 (Thermo Scientific, Waltham, Massachusetts, USA). DNA samples were stored at −20°C until further analyses.
DNA extraction from ileum biopsy
DNA extraction from ileal biopsies was performed using GenElute Mammalian Genomic DNA Miniprep Kit (Sigma-Aldrich, St.Louis, Missouri, USA) according to the manufacturer’s instruction. Briefly, few micrograms of ileum tissue were added to a solution composed of a mixture of lysis solution T and proteinase K, vortexed and incubated at 55°C for 5 hours until the complete digestion of the sample. Samples were then incubated at room temperature for 2 min with RNase A to eliminate residual RNA. Two hundred microlitres of lysis solution C was added and samples were incubated at 70°C for 10 min. After the column preparation, as indicated by manufacturer manual, the lysate was transferred into a column. The elution was performed using 100 µl of elution buffer. Columns were incubated 5 min at room temperature and centrifuged at 6500 g for a minute. The flow-through was collected. Obtained DNA was visualised on a UV Transilluminator: Gel Doc 2000 (Bio-Rad, Hercules, California, USA) after a 0.8% agarose gel electrophoresis to evaluate DNA quality and quantified using the spectrophotometer Smart-Spec Plus (Bio-Rad). DNA was stored at −20°C for further analysis.
Polymerase chain reaction
SFB gene amplification was performed starting from 150 ng of genomic DNA, in a final volume of 30 µL. Amplification was carried out in the presence of 1X buffer (10 mM Tris-HCl pH 8.8, 1.5 mM MgCl2, 50 mM KCl, 0.1% Triton X-100), 33 µM dNTPs, 0.5 µM forward and reverse primers (IDT Integrated DNA Technologies, Coralville, Iowa, USA), 2U of DyNAzyme II DNA Polymerase (Finnzymes, Espoo, Finland) and ultrapure water. Primers features are summarised in table 1. Each reaction was subjected to an initial denaturation step of 3 min at 96°C. The 40 PCR cycles used were as follows: denaturation, 15 s at 95°C; annealing, 30 s at 58°C; elongation, 20 s at 72°C. The amplification was performed using Gene Amp PCR System 9700 thermal cycler (Applied Biosystems, Foster City, California, USA). PCR products were analysed by 2.5% agarose-gel electrophoresis, using ChemiDoc MP System (Bio-Rad), image acquisition and analysis was performed using Image Lab Software V.4.0 (Bio-Rad). The molecular weight marker used was GeneRuler 50 bp DNA Ladder (Thermo Scientific) designed to sizing a large wide range of double-stranded DNA.
Employed primers
Sequencing reaction of PCR amplicons
Micro-CLEAN (Microzone, Haywards Heath, West Sussex, UK) reagent was used to purify PCR products from unincorporated primers, according to the manufacturer’s instructions. After these purifications, PCR products were sequenced by using the ABI PRISM BigDye Terminator Cycle Sequencing Ready Reaction Kit, V.1.0 (Applied Biosystems-Life Technologies, Carlsbad, California, USA). Sequencing reactions were performed employing both forward and reverse PCR primers, in a reaction containing 15 ng of PCR template, 3.2 pmol of each sequencing primer, 8 µL of Terminator Ready Reaction Mix, in a final volume of 20 µL. The sequencing reaction consists of 45 amplification cycles (denaturation: 96°C for 10 s, annealing: 58°C for 5 s, elongation: 58°C for 3 min; for each cycle). Unincorporated dideoxyribonucleotides were removed from amplicons by using a 96-well MultiScreen plate (Merck Millipore, Merck KGaA, Darmstadt, Germany) containing Sephadex G-50 (GE Healthcare, Little Chalfont, Buckinghamshire, UK). Electrophoretic separation of sequencing reactions was performed by BMR Genomics (BMR Genomics, Padua, Italy), and the generated data were analysed by the Sequence Scanner software V1.0 (Applied Biosystems-Life Technologies).
Quantitative real-time PCR
SFB DNA quantification was performed using real-time qPCR, and interleukin 8 (IL-8) gene was used as internal reference in order to verify that the same amount of DNA was load in each sample. Thirty nanograms of total DNA, 150 ng of each primer (IDT, Integrated DNA Technologies or Sigma-Aldrich) (table 1) and 1X iTaq Universal SYBR Green Supermix (Bio-Rad) were used for each reaction, reaching the final volume of 20 µL/well. The following amplification conditions were used: 96°C for 3 min, 50 cycles at 95°C for 10 s, 60°C for 30 s and 72°C for 25 s, using CFX96 Touch Real-Time PCR Detection System (Bio-Rad). A melting curve analysis was performed in order to validate primer pairs and amplification conditions. Melting curves have been performed and the results obtained demonstrated in all the reactions analysed absence of primer dimers. Duplicate negative controls (no template DNA) were also run to assess specificity and to rule out contamination. Data were analysed using CFX96 Software and the relative quantification (fold) of SFB DNA was performed using the ∆∆Ct method.
Results
Identification of putative SFB sequences in samples of terminal ileum of patients with ulcerative colitis and control subjects
We first tested, using a PCR approach, the primers proposed by Jonsson25 and by Suzuki et al,26 27 and found that those proposed by Suzuki et al displayed in our experimental conditions good efficiency in generating PCR products (data not shown). Due to the unavailability of SFB cloned DNA to be used as positive control, the PCR reactions were performed on total DNA extracted from faecal samples from stools of young children at their weaning time, a period in which SFB infection and colonisation frequently takes place in animal models (figure 1). In these experiments, 150 ng of input DNA was used and gene amplification was conducted using PCR primers amplifying SFB sequences (figure 1A) (for the sequences of the primers used in our experiments, see table 1) as well as universal PCR primers18 28 amplifying bacterial 16S ribosomal DNA sequences without any species specificity (figure 1B). The stool samples were all positive to SFB amplification, despite the fact that different amounts of 134 bp SFB PCR products were obtained. The identity of amplified PCR products with SFB was verified by DNA sequencing. Second, the experiments were performed on samples isolated from terminal ileum. Figure 2 shows SFB-specific amplification and bacterial 16S ribosomal DNA amplification, from the terminal ileum of patients with ulcerative colitis (n=10) (A and C) and of subjects without evidence of intestinal disease (n=8) (B and D). In these experiments, 150 ng of input DNA was used. A final comment concerning this first approach is that putative SFB sequences were present both in patients with ulcerative colitis and in control subjects and that this PCR amplification gives rise to a 139 bp PCR product, as expected (NCBI Reference Sequence Database, KC135882.1). To further sustain this conclusion, the 139 bp PCR products were sequenced. In online supplementary figure S1, an electropherogram section is depicted obtained sequencing the PCR product amplified from a colorectal ulcerative colitis (RCU) biopsy sample, to be considered as a representative example of the results obtained. When the sequences obtained from the PCR-positive stool samples and from three randomly selected bioptic samples (two RCU patients and one donor) were compared with known sequences retrieved in the NCBI Reference Sequence Database, the highest homology, with up to 94% identity, was found with entries related to Candidatus arthromitus sp. SFB isolated from mouse (NZ_AGAG01000005.1, NZ_CP008713.1, NC_017294.1 and NC_015913.1), rat (NC_016012.1), turkey (NZ_LXFF01000001.1) and human (KC 135882.1) (online supplementary table S1). Sequence variability with the only human SFB sequence available is expected in different isolates as well as the finding that the SFB sequence is conserved when the isolate is analysed in different species. Altogether, these data support the concept that the employed PCR primers allow amplification of putative SFB sequences.
Supplementary file 1
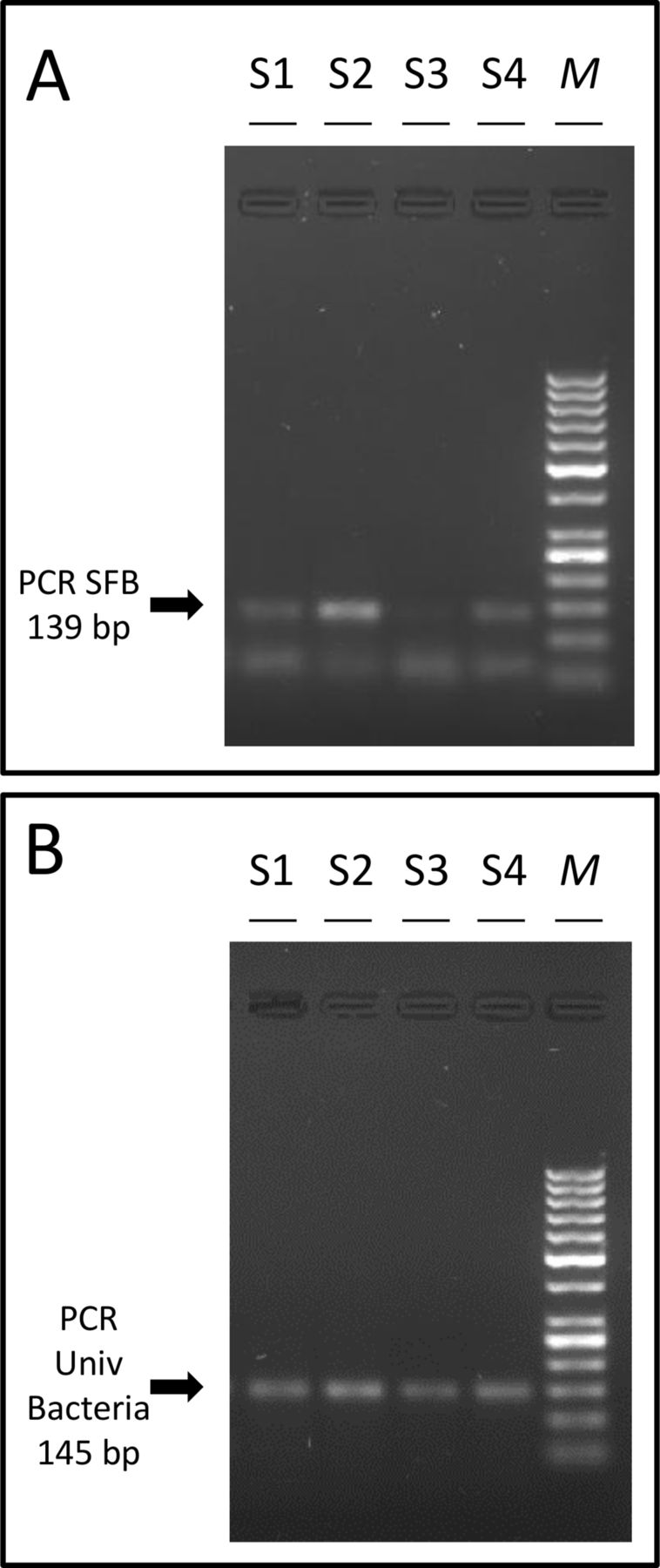
Representative results showing PCR amplification of DNA from stools using PCR primers amplifying (A) SFB sequences and expected to generate an SFB 139 bp specific product or (B) universal PCR primers amplifying bacterial 16S sequences without species specificity. The generated products were analysed by electrophoresis in 2.5% agarose. Expected PCR products are arrowed. Sequences of the employed PCR primers are reported in table 1. M, molecular wt markers; SFB, segmented filamentous bacteria.

PCR amplification of genomic DNA from patients with ulcerative colitis (RCU) (A and C), and healthy subjects (B and D) using PCR primers amplifying SFB sequences and expected to generate an SFB 139 bp specific product (A and B) or universal PCR primers amplifying bacterial 16S sequences without species specificity and originating a 145 bp product (C and D). For nucleotide sequences, see table 1. SFB, segmented filamentous bacteria.
Real-time qPCR analysis
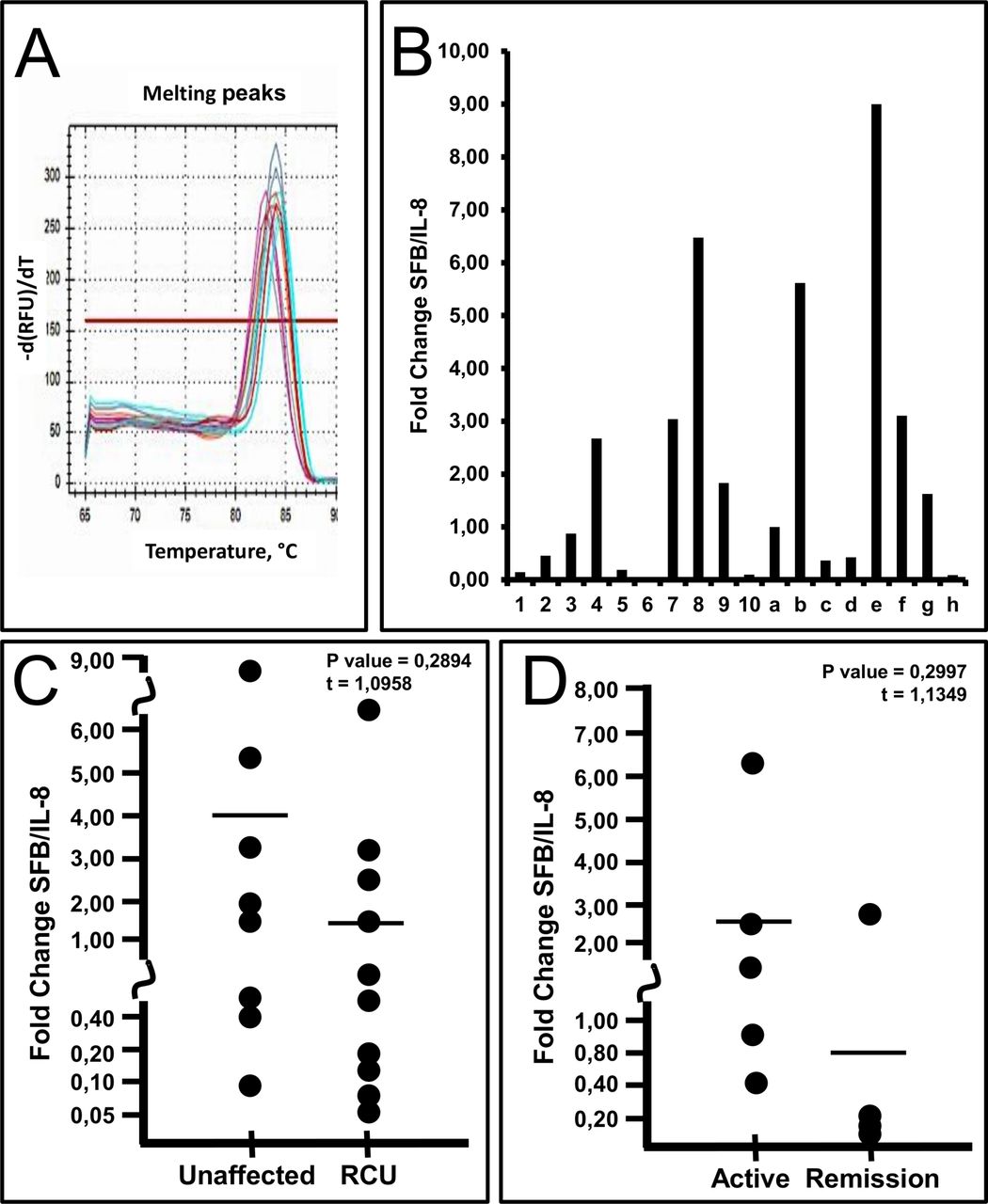
Figure 3A (left side of the panel) shows the real-time qPCR analysis performed using the primers proposed by Suzuki et al.26 27 As internal control, we used primers amplifying a human genomic region (the IL-8 gene) (figure 3A, right side of the panel).29 This was done in order to be confident about the input amount of DNA used in the qPCR mixture. In order to verify the coherence of these data with those shown in figure 2 and based on semiquantitative PCR, samples generating no PCR amplification in figure 2 (n=4) were compared with samples generating the highest levels of PCR products (n=3). As clearly shown, a statistically significant difference in SFB/IL-8 fold change was observed (figure 3B). Melting curves obtained with real-time qPCR analysis demonstrated the absence of primer dimers in all the reactions analysed (figure 4A). The data of qPCR confirm the presence of putative SFB sequences in samples from healthy subjects (figure 4B, samples a–h). When samples from RCU (figure 4B, samples 1–10) and healthy subjects (figure 4B, samples a–h) were compared, no statistically significant difference was found (figure 4C). However, the results obtained using the samples from the terminal ileum of patients with ulcerative colitis suggest a possible association between the bacterial load of SFB and the activity of the disease (see the complete set of data shown in table 2). In particular, the samples from active patients (#2, #3, #4, #8 and #9) showed SFB qPCR reaction products higher, although not reaching statistically significant values (P value=0.2997), when compared with samples obtained from patients in remission (#1, #5, #6, #7 and #10) (figure 4D). This tendency of active disease samples to show higher SFB load suggests that the SFB load might be somehow related to the clinical stage of the ulcerative colitis disease.

Real-time quantitative PCR analysis. Results obtained using genomic DNA samples of biopsies from patients with ulcerative colitis (RCU) and healthy subjects are shown. (A) The employed PCR primers (see table 1 for nucleotide sequences) were reported to amplify SFB (on the left) and IL-8 (in the right). (B) In order to verify the coherence of these data with those shown in figure 2 and based on semiquantitative PCR, samples generating no PCR amplification in figure 2 (n=4) were compared with samples generating the highest levels of PCR products (n=3). IL-8, interleukin 8; SFB, segmented filamentous bacteria.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Analysis of SFB-specific sequences in genomic DNA samples of biopsies from patients with ulcerative colitis (RCU) and healthy subjects: quantitative determination. (A) Melting curves obtained in real-time qPCR with SFB-specific amplification. (B) Fold change with respect to healthy subjects. (B) Fold change of SFB/IL-8-specific amplification of healthy tissue with respect to RCU. (C) Fold change SFB/IL-8 of active with respect to remission RCU samples. IL-8, interleukin 8; SFB, segmented filamentous bacteria.
SFB loading in the clinical samples studied
Discussion
Most of our knowledge about SFB prevalence and body habitat derives from studies in animal systems. The study on SFB in humans is hampered by lack of knowledge about bacterial variations among different host species and, therefore, also by the lack of suitable specific reagents. An additional difficulty is represented by the clinical material to be analysed, that is, morphological studies require bioptic samples. Therefore, molecular analyses performed on faecal samples represent a valuable option, as already reported in the scientific literature.18 Yin et al18 analysed by PCR stool specimens from healthy human individuals of different ages and showed that SFB colonisation is age dependent, occurring within the first 2 years of age. Our analysis of a very limited number of faecal samples from children at the time of their weaning showed highly frequent positivity, confirming the observation by Yin et al about colonisation at a very young age, and further delimitates it to the time of weaning (or before).
This is the first study in which PCR methods are used to identify SFB in biopsies from the terminal ileum of patients with ulcerative colitis and control subjects. Our results confirm that quantitative and qualitative PCR may represent a useful tool for the detection of SFB presence and analysis of the bacterial load. From our study, it is possible to conclude that putative SFB sequences are present in both patients with ulcerative colitis and control subjects. Therefore, it appears that SFB cannot be considered as being uniquely associated with the disease. On the other hand, a second very important finding of our study is that among the patients with ulcerative colitis a close tendency does exist between bacterial presence and density and activity of the disease. A possible hypothesis, also based on the physiological role played by SFB on the maturation and the differentiation of the immune system, is that SFB is normally present in healthy subjects. In patients with ulcerative colitis, SFB presence and density do not appear directly related to the pathogenesis of the disease which could be linked to other microbiological and genetic factors; however, the disease may not be able to express themselves in the acute phase in the absence of SFB for the peculiar relationship of this bacterium with some components of the immune response, particularly in respect to Th-17 lineage.
Notably, SFB has been recognised as the only member of the gut microflora exhibiting the ability of inducing specific immune responses: in fact, SFB can be considered as the most potent microbial stimulus inducing intestinal IgA-producing cells,9 30 since it was found to induce the development of IgA plasma cells in the gut lamina propria and natural IgA occurring gut secretions. On the other hand, an aberrant and persistent SFB expansion throughout the small intestine has also been shown in IgA-deficient mice.26 In addition, SFB selectively induces the expression of the major histocompatibility complex class II molecules on the intestinal epithelial cells.9 More importantly, T-cell-mediated immunological responses are specifically induced by SFB. In this respect, natural killer (NK) cells and CD8+ T cells colonisation of mice by SFB induces a significant increase in cytotoxic activity.19 Given the influence of SFB on many players of the immune response, it seems quite possible that this bacterium can interfere with the expression and the activity of ulcerative colitis. It should also be underlined that SFB does not cause an apparent inflammatory reaction in the lamina propria of colonised areas16 31 and is therefore not considered a pathogenic bacteria.
These SFB biological effects might open new perspectives about possible pharmacological development of new therapeutic approaches, also considering that both antibiotics and probiotics have been found active against SFB in mice. In this respect, penicillin displayed the potential of eliminating SFB from the mouse terminal ileum as a first-step response, but some weeks after the halting of the antibiotic treatment a recolonisation of the ileum observed was reproducible.32 In addition, the high increase of SFB load in ileum samples of immunosuppressed mice was brought again into normal values when animals received the probiotic Lactobacillus plantarum.33 Chemotherapic cycles with effective antibiotics may induce rapid remission of active disease and the remission could be maintained through successive appropriately seriated antibiotic cycles over time. Although both antibiotic and probiotic treatments have shown some beneficial effects in the treatment of ulcerative colitis, their clinical use is limited so far. In relation to antibiotic therapy, fewer data are available in ulcerative colitis than in Crohn’s disease and the majority of them consists of limited small trials of ciprofloxacin, metronidazole and rifaximin based.34 As the outcome of these trials was not associated with a benefit for the treatment of active ulcerative colitis, two meta-analyses conducted by Wang et al35 and Khan et al36 concluded that antibiotic therapy leads to a moderate improvement of the clinical symptoms. While these data are clearly insufficient, our preliminary findings concerning SFB in patients with ulcerative colitis may influence the future research in this field. On the other hand, outcomes of an important meta-analysis by using probiotics in patients with ulcerative colitis37 seem to confirm that the use of lactobacilli speculatively able to compete for the attachment to the specialised epithelium in the terminal ileum is as effective as with standard mesalazine in maintaining remission.
Further investigations have to be carried out both to confirm these preliminary findings in a more large sample of patients and controls and to evaluate the antibiotic effectiveness in reducing the presence or the load of SFB by qualitative and quantitative PCR. The corollary successive research would be to identify more successful antibiotic and/or probiotic treatments to eradicate the presence and/or reduce the density of SFB, also evaluating these treatments in relation to the acute phase and maintaining remission of ulcerative colitis.
Acknowledgments
We would like to thank Dr Eleonora Brognara and Dr Cristina Zuccato for technical assistance and support.
References
Footnotes
Contributors AF, DDL, RG, MC: study concept and design; GM, VM, VG, MC: collection of biological material; AF, JG, IL, LCC, VG: performing the experiments on biological material; AF, JG, IL, DDL, RG, MC: analysis and interpretation of data; AF, JG, GM, DDL, RG, MC: writing and editing of the manuscript; GM, DDL, RG, MC: critical revision of the manuscript and important intellectual content. All authors approved the final draft of this manuscript for submission.
Funding This research was supported by grants from Consorzio Interuniversitario di Biotecnonologie (CIB) 2016, and by Fondo per le Agevolazioni alla Ricerca (FAR 2016) of Italian Ministry of Education, Universities and Research.
Competing interests None declared.
Ethics approval The protocol was approved by the local Ethics Committee of Azienda Ospedaliera Universitaria di Ferrara (Protocol n.86–2013, 20 June 2013).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement ll relevant data are within the paper and its supporting materials