Article Text

Statistics from Altmetric.com
Message
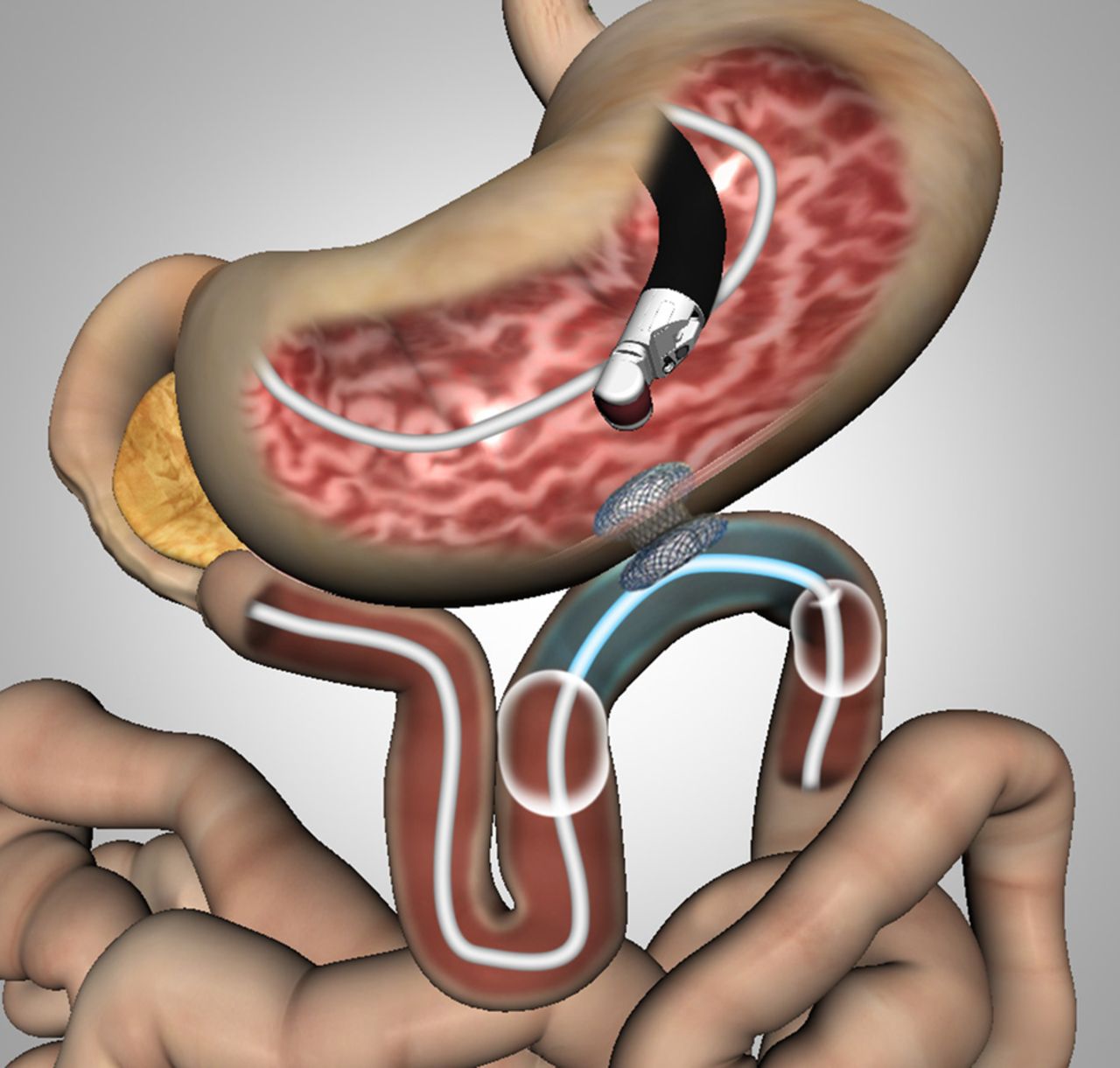
Surgical gastrojejunostomy (GJ), which has been the standard palliative treatment for malignant gastric outlet obstruction (MGOO), is associated with good functional outcome and the long-term relief of symptoms. Endoscopic placement of a metal stent for MGOO treatment has been gaining popularity as an alternative to surgical GJ because of its high technical success rates and less invasiveness. Interestingly, several investigators have attempted endoscopic GJ as ‘endoscopic bypass’ for longer efficacy while maintaining a less invasive procedure.1 We previously reported on the feasibility and safety of EUS-guided GJ (EUS-GJ) using a lumen-apposing metal stent (LAMS)2 ,3 and a special double-balloon enteric tube in an animal model and a pilot clinical study.3 Herein, we describe the first prospective clinical study of EUS-guided double-balloon-occluded gastrojejunostomy bypass (EPASS) using a LAMS (figure 1). We performed EPASS in 20 patients with MGOO. The double-balloon tube (figure 2) was correctly inserted into the jejunum across from the stomach in all cases. The technical success rate of stent placement was 90%.

Schema of EUS-guided double-balloon-occluded gastrojejunostomy bypass (EPASS) using a lumen-apposing metal stent.

Double-balloon enteric tube allows the filling-water between two balloons.
In more detail
EPASS was performed in 20 patients with MGOO between March 2014 and March 2015 (10 male) (supplementary tables 1 and 2). The median intubation time of the double-balloon tube insertion was 10.5 min (range 6–28 min). The technical success rate of stent placement was 90% (18/20) (figure 3 and supplementary table 3). The median intubation time from the double-balloon tube intubation to stent placement was 25.5 min (range 10–39 min). In the two failed cases, we recognised the maldeployment of the distal flange immediately after deployment of the proximal flange by the presence of pneumoperitonium on fluoroscopy and endoscopic visualisation of the abdominal cavity through the LAMS. Post-treatment gastric outlet obstruction scoring system (GOOSS) score improved in all 18 cases in which EPASS was successfully performed. The mean post-GOOSS score was significantly higher than the pre-GOOSS score (0.6±0.75 vs 2.94±0.23, p<0.001). The median post-GOOSS score was significantly higher than the pre-GOOSS score (0 vs 3, p<0.001). No stent occlusion or migration was observed in 18 cases during the follow-up period (median 100 days; range 44–233 days).
{kind=link}
{kind=link}
{kind=link}
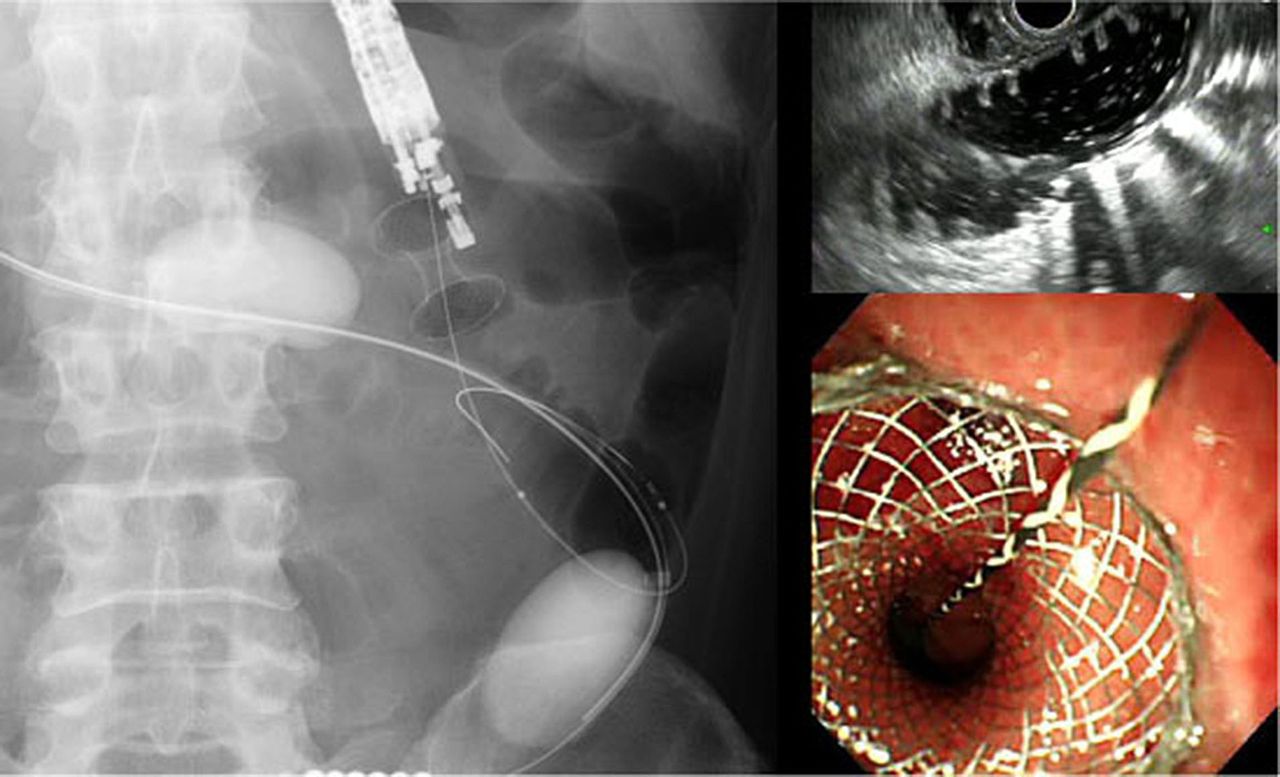
EPASS procedure. EUS shows distended jejunum (right upper). Biflanged lumen-apposing metal stent is placed between stomach and jejunum (left). Endoscopic imaging proximal flange in the stomach (right lower).
Comments
In the present study, we demonstrated a high technical success rate (90%) for EPASS. Notably, in cases of the free style technique, the technical success rate was 9/9 (100%). These data are similar to or better than those of endoscopic stenting reported previously.4 In the EPASS technique, we considered several important points for a safe and reliable procedure as follows. First, we used a 0.89-inch large diameter guidewire and/or an overtube to facilitate passage of the double-balloon enteric tube into the jejunum beyond the ligament of Treitz even with the presence of severe obstruction. The importance of using a large diameter guidewire and/or an overtube is to avoid the looping of the balloon tube in the stomach fornix and enable its advancement over the 0.025-inch guidewire. In fact, in this study, the double-balloon tube could be advanced into the jejunum in all cases in approximately 10 min without any difficulty. In our experience, the overtube was superior to the guidewire for the balloon tube advancement. Second, anatomically the jejunum beyond the ligament of Trize is the most close position to the gastric wall based on our examination of a lot of screening upper GI graphy (unpublished data). Thus, if the saline solution is filled only between two balloons across this portion, the distended jejunum is easily located under EUS guidance, allowing easy and safe access to the jejunum. Third, we found that the cautery tipped delivery system (Hot Axios, Xlumena, Mountain View, California, USA) enables a true ‘one-step stenting’ for EUS-GJ, simplifying the procedure tremendously. In general, tract dilation is required in all EUS-guided transmural stent placement procedures and is eliminated if this delivery system is used. Eventually, EPASS was completely performed in the endoscopic unit within 30 min in all cases. Our present data suggest that EPASS is easier and faster than surgical GJ and is relatively comparable to endoscopic stenting.
Although direct access under EUS guidance appears simple, the ordinary jejunum is usually collapsed and can contain air, guaranteeing no safe puncture. Moreover, even if the puncture is successfully performed, following several steps such as guidewire advancement in the deeper jejunum, tract dilation and stent delivery system insertion is not easy because the collapsed jejunum can move away from the stomach. Thus, to date, there have only been two major techniques for EUS-GJ, namely, water-filling technique2 ,5 and water-inflated balloon technique.5 For the water-inflated balloon technique, although needle puncture to the inflated balloon (approximately 2 cm) appears easy to perform in the jejunum, following the procedure, however, seems to be difficult unless lumen-apposing devices such as a tilt-tag or an anchor wire are used ideally for securing the jejunum to the stomach wall and bringing together the two non-adherent organs. In terms of the water-filling technique, rapid infusion of a large amount of water to sufficiently dilate the small bowel may cause serious complications, including dilutional hyponatraemia and a general burden on the cardiovascular system. In addition, the injection of a large amount of fluid distends the targeted small intestine and the colon, leading to miss-puncture such as in gastrocolonostomy. Therefore, EPASS appears to be the preferred technique for EUS-GJ.
In the present study, we encountered two unsuccessful stent deployment cases. After carefully reviewing the video from the two failed cases, we realised that pushing the guidewire caused the distended jejunum to move away from the stomach, resulting in maldeployment of the LAMS. Since then, we stopped using the over-the-wire technique and selected the ‘free style’ direct catheter advancement/stent placement technique instead. Consequently, the technical success rate improved from 81.8% to 100%. Our result suggests that the best EUS-GJ technique is double-balloon tube placement using the overtube and the direct catheter advancement/stent placement using an electrocautery tipped delivery system containing a LAMS.
The main purpose of the therapy for MGOO is to restore the ability to eat. Thus, long-term stent function is one of the most important issues for the treatment of MGOO. Our results revealed that post-GOOSS score was significantly improved compared with pre-GOOSS score. In particular, a GOOSS score of 3 was observed in all cases but 1. Surprisingly, there were no stent occlusion cases needing re-intervention during the follow-up period. These results were quite different from previous data of endoscopic stenting and even surgical GJ.4 Our results suggest that a 15 mm diameter and 10 mm long stent works well for the intake of a low-residue or full diet. We are not sure whether a 15 mm diameter LAMS is ideal or not for MGOO treatment because the standard diameters of surgical GJ and endoscopic metal stents are 30 and 20 mm, respectively. However, a LAMS diameter of 15 mm was the maximum stent size that could be included in the 10.8-F delivery system. Nevertheless, we believe that a 15 mm fully covered LAMS can prevent tumour ingrowth and maintain sufficient stent patency based on the present results.
In terms of adverse events, stent maldeployment was observed in two cases (10%). As we observed this immediately after stent placement, the stent was removed and the patient was treated by conservative therapy. However, if the patient's condition is poor owing to cancer progression and concomitant acute cholangitis, stent maldeployment may cause a fatal event. Regarding the rate of late adverse events, such as stent occlusion due to tumour ingrowth or stent migration in EPASS using a LAMS, appears to be low compared with endoscopic stenting because of the biflanged, fully covered and short-length LAMS. From this point, once a LAMS is placed correctly, the long-term efficacy of EPASS appears to be similar to that of surgical GJ.
In conclusion, we established the feasibility of an EUS-GJ technique using a unique double-balloon tube and a novel electrocautery tipped stent delivery system equipped with a LAMS in the human setting.
Acknowledgments
We are grateful to Associate Professor Edward Barroga, Senior Medical Editor of the Department of International Medical Communications for the editorial review of the manuscript. We also appreciate Professor Arthur Kaffes to give us great suggestion in EPASS procedure.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors TI: literature search, study design, patient inclusion, data collection, data analysis, statistical analysis, data interpretation, drafting of the manuscript and final approval. KI, NI, AS, TG and FM: patient inclusion, data collection, critical revision and final approval of the manuscript. VD, AYBT and KFB: critical revision and final approval of the manuscript.
Competing interests TI: Consultant for Xlumena. KFB: the inventor of the AXIOS stent and delivery system and the founder of Xlumena.
Patient consent Obtained.
Ethics approval Ethical Committee and board of Tokyo Medical University.
Provenance and peer review Not commissioned; internally peer reviewed.