Acute pancreatitis
BMJ 2014; 349 doi: https://doi.org/10.1136/bmj.g4859 (Published 12 August 2014) Cite this as: BMJ 2014;349:g4859
Chinese translation
该文章的中文翻译

- C D Johnson, professor of surgical sciences1,
- M G Besselink, hepatopancreatobiliary surgeon2,
- R Carter, consultant pancreatic surgeon3
- 1University Surgery, University Hospital Southampton, SO16 6YD, UK
- 2Dutch Pancreatitis Study Group, Academic Medical Center Amsterdam, Netherlands
- 3West of Scotland Pancreatic Unit, Glasgow Royal infirmary, Glasgow, UK
- Correspondence to: C D Johnson cdj{at}soton.ac.uk
Summary points
All patients with acute pancreatitis should have liver function tests and abdominal ultrasonography within 24 hours of admission to look for gallstones
Severe acute pancreatitis is characterised by persistent (>48 hours) organ failure; these patients have a >30% mortality rate
If symptoms persist for more than seven days computed tomography is required to assess pancreatic and peripancreatic necrosis
Initial management includes adequate fluid resuscitation and supplemental oxygen
If gallstones are found, definitive treatment (by cholecystectomy or sphincterotomy) should be given within two weeks of resolution of symptoms
Necrotising pancreatitis should be managed by a specialist team including surgeons, endoscopists, interventional radiologists, and intensivists
Acute pancreatitis is a common cause of emergency admission to hospital. Most hospitals in the United Kingdom serving a population of 300 000-400 000 people admit about 100 cases each year. We review up to date evidence for the assessment, diagnosis, and management of acute pancreatitis.
Sources and selection criteria
We have drawn heavily on three recent evidence based guidelines1 2 3 that we helped to write and we reviewed the Cochrane Library for relevant clinical trials. In December 2013 we again reviewed the Cochrane Library to identify any systematic review or update relevant to acute pancreatitis.
What is acute pancreatitis?
Acute pancreatitis is inflammation of the pancreas; it is sometimes associated with a systemic inflammatory response that can impair the function of other organs or systems. The inflammation may settle spontaneously or may progress to necrosis of the pancreas or surrounding fatty tissue. The distant organ or system dysfunction may resolve or may progress to organ failure. Thus there is a wide spectrum of disease from mild (80%), where patients recover within a few days, to severe (20%) with prolonged hospital stay, the need for critical care support, and a 15-20% risk of death.3 If patients have organ failure during the first week in hospital, it is usually already present on the first day in hospital.1 This early organ failure may resolve in response to treatment. The diagnosis of severe acute pancreatitis depends on the presence of persistent organ failure (>48 hours) either during the first week or at a later stage, and also on the presence of local complications (usually apparent after the first week).
What are the risk factors and potential causes of acute pancreatitis?
Acute pancreatitis has many causes, the commonest in most European and North American studies being gallstones (50%) and alcohol (25%). Rare causes (<5%) include drugs (for example, valproate, steroids, azathioprine), endoscopic retrograde cholangiopancreatography, hypertriglyceridaemia or lipoprotein lipase deficiency, hypercalcaemia, pancreas divisum, and some viral infections (mumps, coxsackie B4). About 10% of patients have idiopathic pancreatitis, where no cause is found.
How does acute pancreatitis present?
Acute pancreatitis presents as an emergency, requiring acute admission to hospital. Patients almost always mention severe constant abdominal pain (resembling peritonitis), usually of sudden onset and, in 80% of cases, associated with vomiting. The pain may radiate to the back, usually the lower thoracic area. Most patients present to hospital within 12-24 hours of onset of symptoms. Abdominal examination shows epigastric tenderness, with guarding. Differential diagnoses to consider include perforated peptic ulcer, myocardial infarction, and cholecystitis.
How is the diagnosis confirmed?
Biochemical tests
The diagnosis is based on abdominal pain and vomiting, associated with increases in serum amylase or lipase levels at least more than three times the upper limit of normal.2 3 In the United Kingdom, amylase testing is widely available, although estimation of lipase is preferred by some because lipase levels remain increased for longer than amylase levels after the onset of acute pancreatitis. In about 5% of patients, enzyme levels may be normal at the time of admission to hospital.
Imaging
In cases where there is diagnostic doubt, either because the biochemical tests are not conclusive (enzyme levels may decrease during delayed presentation to hospital) or because the severity of clinical presentation raises the possibility of other intra-abdominal conditions such as perforation of the gastrointestinal tract, contrast enhanced computed tomography may be needed to make the diagnosis.2 3 4 International consensus is that acute pancreatitis is diagnosed when two of three criteria are present: typical abdominal pain, raised enzyme levels, or appearances of pancreatitis on computer tomography. Computed tomography also has a role in the assessment of the severity of acute pancreatitis if the illness fails to resolve within one week.
What other diagnostic tests are required?
Once acute pancreatitis has been diagnosed, the cause needs to be sought. In most cases this will be determined from a combination of careful clinical evaluation and initial investigations. When taking a history, it is important to ask about alcohol consumption, drug use, symptoms of viral illness, and a family or personal history of genetic disease. Blood tests may reveal hypercalcaemia and hypertriglyceridaemia. Abdominal ultrasonography may identify gallstones. No evident cause will be found in 10-20% of patients3; these people may require further investigation, especially if they have experienced more than one acute attack.
Ultrasonography
Gallstones are found in about half of patients with acute pancreatitis, so in every case abdominal ultrasonography should be performed within 24 hours of admission to look for gallstones in the gallbladder.3 5 Early detection helps plan the definitive management of gallstones (usually by cholecystectomy) to prevent further attacks of pancreatitis.
Liver function tests
In addition to ultrasonography, increased liver enzymes levels provide supportive evidence for gallstones as the cause of the acute pancreatitis. Two large observational studies with 139 and 464 patients of whom 101 and 84 had gallstones found that an alanine transaminase (ALT) level >150 U/L has a positive predictive value of 85% for gallstones.4 5 6 These tests should be done in all patients within 24 hours of admission.
Endoscopic ultrasonography
A systematic review of five studies in patients with apparently idiopathic pancreatitis after initial assessment reported a diagnostic yield of up to 88% with endoscopic ultrasonography, with detection of biliary sludge, common bile duct stones, or chronic pancreatitis.7
Magnetic resonance cholangiopancreatography
Expert opinion also recommends magnetic resonance cholangiopancreatography to elucidate rare anatomical causes of acute pancreatitis.2 The sensitivity of this investigation is improved by the addition of secretin stimulation.
Endoscopic ultrasonography and magnetic resonance cholangiopancreatography are usually requested only after patients have recovered from the acute phase and after a detailed history and repeat ultrasonography have failed to identify a cause.
How is the severity of acute pancreatitis assessed?
Eighty per cent of patients with acute pancreatitis respond to initial support with intravenous fluid, oxygen supplements, and analgesia, and they can be discharged home within a week or so. About 20% of patients, however, do not recover during the first few days and may need transfer to a specialist unit.8
The Atlanta classification is a useful framework for assessing the severity of acute pancreatitis.9 The current classification recognises three levels of severity: mild, where patients recover with good supportive care within a week without complication; moderately severe, in which there is transient organ failure that resolves within 48 hours, or a local complication (that is, peripancreatic fluid collections) without organ failure; and severe acute pancreatitis, in which there is persistent organ failure for more than 48 hours. This classification enables non-specialist clinicians to identify those patients who require treatment by, or in consultation with, a specialist centre (box 1). Persistent organ failure during the first week is associated with a 1 in 3 risk of mortality.10 11
Box 1: Revised Atlanta classification of acute pancreatitis9: definitions of severity
Mild
No organ failure
No local or systemic complications
Moderately severe
Organ failure that resolves within 48 hours (transient organ failure)
Local or systemic complications (sterile or infected) without persistent organ failure
A patient with moderately severe pancreatitis may have one or both of these features
Severe
Persistent organ failure (>48 hours): single organ or multiple organ failure
Definitions of organ failure: thresholds for organ failure
Respiratory: arterial oxygen pressure/fractional inspired oxygen ≥300
Circulatory: systolic blood pressure <90 mm Hg and not fluid responsive
Renal: plasma creatinine concentration ≥170 µmol/L
Patients who have local complications and organ failure with infection of the pancreas or extrapancreatic necrosis are at extremely high risk of death.12 This subgroup of patients should be managed in a specialist centre.
Markers of severity in the first week
Markers of systemic inflammatory response syndrome help to identify those patients who may develop persistent organ failure. Several observational studies have shown a strong association between persistent systemic inflammatory response syndrome (>48 hours) and subsequent persistent organ failure (box 2).11 13
Box 2: Features of systemic inflammatory response syndrome (SIRS)*
Core body temperature >38°C or <36°C
Heart rate >90 bmp
Respiratory rate >20/min (or arterial carbon dioxide pressure <32 mm Hg)
White cell count >12×109/L or <4×109/L
*If SIRS is present for >48 hours the patient is likely to have severe pancreatitis
There are many different predictive scoring systems for severity based on physiological variables or single biochemical markers, but none of these has shown clear superiority.
The acute physiology and chronic health evaluation (APACHE)-II score can be assessed within 24 hours of admission to hospital and is a useful positive predictor of severe pancreatitis if scored 8 or more.14 The early warning score (or a modified EWS) is widely used for recording clinical observations (pulse, blood pressure, respiratory rate, and urine output) in hospitals in the United Kingdom and has a similar accuracy for prediction of severe pancreatitis.15 Scoring systems have limited day to day value in the management of patients and perform best for the description of patient groups in clinical trials and other research studies.
Computed tomography
Computed tomography should be performed to look for local complications in those with signs or symptoms of systemic disturbance, particularly persistent organ failure that lasts for more than one week. As described in the revised Atlanta criteria,9 local complications include peripancreatic fluid collections, or necrosis (hypoperfusion) of pancreatic or peripancreatic tissue (necrotising pancreatitis). Fluid collections and areas of necrosis may be identified early (<4 weeks) or late (>4 weeks) (box 3 and figure⇓).
Box 3: Revised definitions of types and grades of severity of acute pancreatitis9
Interstitial oedematous pancreatitis
Acute inflammation of pancreatic parenchyma and peripancreatic tissues, but without recognisable tissue necrosis
Necrotising pancreatitis
Pancreatic parenchymal necrosis or peripancreatic necrosis, or both
Acute peripancreatic fluid collection
Peripancreatic fluid with interstitial edematous pancreatitis but no necrosis (this term applies only within the first 4 weeks after onset of interstitial edematous pancreatitis and without features of a pseudocyst)
Pancreatic pseudocyst
Encapsulated collection of fluid with a well defined inflammatory wall usually outside pancreas with minimal or no necrosis (usually occurs > 4 weeks after onset of pancreatitis)
Acute necrotic collection
Fluid and necrosis associated with necrotising pancreatitis affecting pancreas or peripancreatic tissues, or both
Walled-off necrosis
Mature, encapsulated collection of pancreatic or peripancreatic necrosis with an inflammatory wall, or both (walled-off necrosis usually occurs >4 weeks after onset of necrotising pancreatitis)
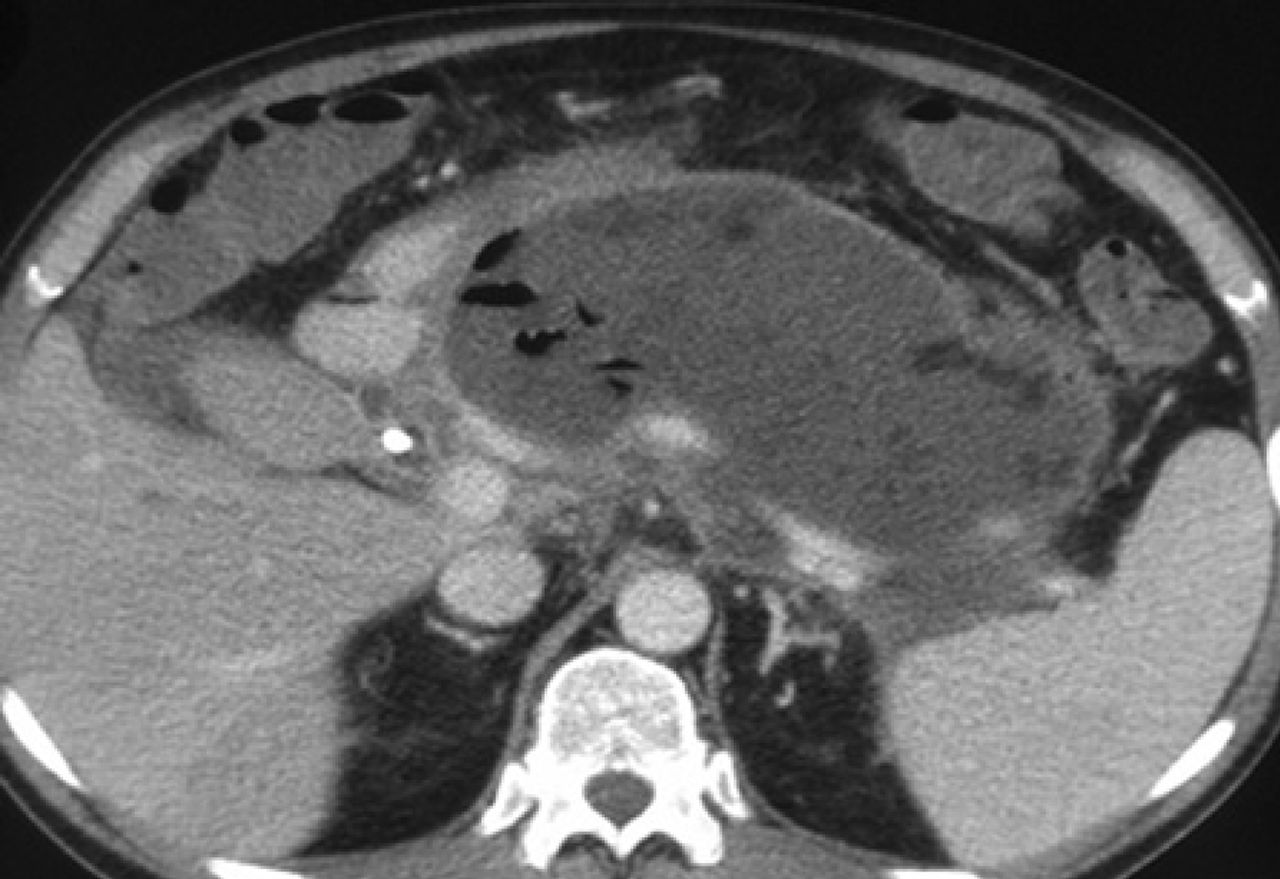
Body of pancreas and surrounding tissue replaced by area of walled-off necrosis with enhancing wall, which contains bubbles of gas (black areas), clearly different from heterogeneous variations in density elsewhere and diagnostic of infection
{kind=link}
Evidence from a descriptive study with 88 patients16 and the UK guidelines3 recommend that the first computed tomography scan for assessment of severity should be performed 6-10 days after admission in patients with persistent systemic inflammatory response syndrome or organ failure. Computed tomography scoring systems do not outperform clinical scoring systems for prediction of severity and evidence suggests that early (inappropriate) computed tomography increases length of hospital stay with no improvement in clinical outcome.2
How is acute pancreatitis managed?
Fluid management
Two small randomised studies with 40 and 41 patients investigated the effect of different types of fluid on outcomes. These showed benefit for Ringer’s lactate compared with other types of fluid, in that fewer patients had systemic inflammatory response syndrome, and C reactive protein levels were lower although clinical outcomes did not differ.17 18 Guidelines by the International Association of Pancreatology2 recommend the use of Ringer’s lactate; in the United Kingdom, Hartmann’s solution is a widely used alternative.
Infusion rates during the first 24 hours in hospital should be sufficient to restore circulating volume and urine output.4 Consensus opinion is that 2.5-4 litres in 24 hours will be sufficient for most patients, but that volumes infused should be determined by the clinical response. Two randomised studies with a total of 191 patients19 20 showed that more aggressive fluid replacement increased the requirement for mechanical ventilation and rates of sepsis and death. In these studies the control groups received 2.5-4.8 litres of crystalloid daily in the first 48 hours, whereas the treatment groups received 4.0-5.8 litres daily. Restoration of circulating volume while maintaining haematocrit above 0.35 was associated with a better outcome. However, further prospective data are needed to clarify whether patients deteriorate because of inadequate fluid replacement or because of the severity of illness despite large volumes.
Consensus opinion is that response to fluid resuscitation should be assessed by non-invasive response monitoring (heart rate <120 bpm, mean arterial pressure 65-85 mm Hg, urine output 0.5-1 mL/kg/h). However, a recent large three arm randomised trial21 with 64-68 patients per arm compared non-invasive monitoring with invasive monitoring in patients with severe acute pancreatitis admitted to an intensive care unit within 24 hours of onset of the disease. All the patients received saline and colloid (hydroxyethyl starch), and one group received fresh frozen plasma in addition. Rates of infusion were regulated by vital signs, urine output, and haematocrit over the first 24 hours in the control group. The other two groups had invasive monitoring. The patients who received early goal directed treatment with invasive monitoring had fewer days of ventilator support or intensive care unit stay and lower rates of abdominal compartment syndrome, organ failure, and death. This carefully monitored approach to rapid fluid resuscitation is rational and requires further evaluation.
Early antibiotic treatment
A Cochrane review22 of seven evaluable studies with 404 patients found no statistically significant effect of early antibiotics on reduction of mortality. Rates of infected necrotising pancreatitis were similar (treatment 19.7%, controls 24.4%) and rates of non-pancreatic infection were not affected by early antibiotic treatment. The authors concluded that antibiotics had no benefit in preventing infection of necrosis or death. None of the included studies was adequately powered, but a separate analysis showed an inverse relation between the study quality and effect size.23
At present there is no indication for early antibiotics to prevent infection of (presumed or existing) pancreatic necrosis.4 If infection is clinically suspected or found, antibiotic treatment should be guided by sensitivity of cultured organisms when available and by the duration and severity of septic symptoms.
Pain relief
The main symptom of acute pancreatitis is pain, and respiratory function may be impaired by restriction of abdominal wall movement. Providing effective analgesia may require the use of opioids. There are some theoretical risks of exacerbation of pancreatitis by morphine, which can increase pressure in the sphincter of Oddi, but there is little good evidence that this is clinically significant and no evidence exists about the comparative effectiveness of different opioids in acute pancreatitis.
Nutrition
Pancreatic endotoxin absorption is thought to be a potent stimulus of the systemic inflammatory response syndrome and contributes to a cycle of events that leads to organ failure in acute pancreatitis. It is assumed that enteral nutrition may help maintain the gut mucosal barrier and so reduce the absorption of endotoxin. However, these theoretical advantages have not been supported by clinical trials.
Mild pancreatitis
Three randomised trials with a total of 413 patients have shown that early oral nutrition in patients with mild pancreatitis does not increase the rate of complications. Enteral tube feeding shows no benefit in patients with mild pancreatitis, and such patients can resume oral intake as soon as they feel able.2
Severe pancreatitis
A Cochrane review24 of enteral versus parenteral nutrition in patients with (predicted) severe acute pancreatitis identified eight trials that showed a substantial reduction in mortality and complications with early enteral nutrition. It is possible that the difference between enteral and parenteral nutrition is an excess of complications such as line sepsis and other infections in the parenteral group.
One small randomised trial25 showed no difference between enteral nutrition and no support. A recent large multicentre trial in the Netherlands randomised 101 patients to early nasojejunal tube feeding started within 24 hours of admission and 104 to a control group with starvation for 72 hours followed by an oral diet with on-demand nasoenteral feeding whenever oral intake was insufficient. Preliminary data26 showed no difference in outcome. Therefore no evidence supports the use of enteral nutrition as prophylaxis for complications. Most specialist units in the United Kingdom refrain from early enteral nutrition and allow oral intake as tolerated.
Route of enteral nutrition
If enteral nutrition is required, it is usually delivered by tube feeding. Two randomised trials with 50 and 31 patients27 28 suggest that at least 80% of patients can tolerate the nasogastric route, avoiding the need for nasojejunal intubation. Nasogastric intubation is a ward based procedure and does not require specialist techniques such as radiological screening or endoscopic placement; nasojejunal tubes require these resources, and in practice the tube often becomes displaced back into the stomach. The patient experience of the two types of tube is similar.
Enteral nutritional supplements
The type of nutritional supplement used for tube feeding seems to have no effect on outcome in severe acute pancreatitis. A meta-analysis of 20 randomised trials concluded that no specific enteral nutrition supplement or immunonutrition formulation had any advantage.29
What is the best time for cholecystectomy after gallstone pancreatitis?
Expert consensus is that the best time to operate to deal definitively with gallstones is during the index admission with acute pancreatitis, after the initial symptoms have resolved. The risk of recurrent pancreatitis is directly related to the interval between first attack and cholecystectomy.30 Any recommended time limit is arbitrary, but the shorter the interval the lower the risk.
Whereas after mild biliary pancreatitis, cholecystectomy must be undertaken as soon as possible, the patient who has had a severe attack may be debilitated and may have ongoing intra-abdominal inflammatory changes. Further interventions within the abdomen may be needed. All of these considerations affect the timing of cholecystectomy, which should probably be delayed at least six weeks after discharge from hospital to allow resolution of inflammatory changes. No evidence supports this expert consensus.
How is necrotising pancreatitis managed?
Necrotising pancreatitis is suspected when there are persistent signs of systemic inflammation for more than 7-10 days after the onset of pancreatitis.
It is now widely accepted that intervention in the first two weeks of severe acute pancreatitis should be avoided if possible because of high mortality. Rare exceptions to the non-intervention approach include intra-abdominal haemorrhage or necrosis of bowel. In either case, it is better if possible not to disturb the pancreatic inflammatory mass at this time.
There is consensus that pancreatic intervention should be delayed until walled-off necrosis has developed, typically 3-5 weeks after the onset of symptoms. Indications for intervention include confirmed (or strongly suspected) infection of necrosis and persistent organ failure for several weeks with a walled-off collection. Patients who might require intervention—that is, anyone with a hospital stay of more than 14 days after the onset of symptoms—should be managed by, or in consultation with, a specialist pancreatic team.
A randomised trial of 88 patients compared primary open necrosectomy with a “step-up” approach of percutaneous drainage, followed by minimally invasive surgical necrosectomy if needed.31 The step-up approach reduced major morbidity by 43%. Of the patients assigned to this approach, 35% were treated with percutaneous drainage only. Based on this trial and other studies, including a systematic review,32 the consensus is that the initial step should be catheter drainage,2 but there is no consensus on the best intervention for necrotising pancreatitis.
What treatment is required after discharge following severe acute pancreatitis?
After severe acute pancreatitis, patients need general supportive measures and some specific treatments. In addition, the cause of the pancreatitis should be identified and treated if possible, most often by treatment of gallstones. Many pancreatic specialists recommend avoidance of alcohol for 6-12 months whatever the cause or severity of the pancreatitis. There is evidence from a randomised trial that interventions to manage alcoholism may reduce recurrent attacks of pancreatitis in those with high alcohol intake.33 34
This review will not consider the needs of patients who have spent a considerable period in intensive care with a serious illness, apart from pancreatitis specific problems. Most patients recovering from severe acute pancreatitis will have had weight loss during their illness, and at the time of discharge from hospital may have ongoing anorexia, which impairs their ability to regain weight. Such patients therefore benefit from nutritional supplements, which may need to be varied to improve acceptability. In specialist centres a dietitian is often available to advise on nutritional support during this recovery phase.
After severe acute pancreatitis, patients often have impaired pancreatic exocrine and endocrine function. Hyperglycaemia may be absent initially if nutritional intake is low, and blood glucose should be tested in the weeks after discharge as intake improves.
Pancreatic exocrine insufficiency is under-recognised in the recovery phase after severe acute pancreatitis. In two small observational studies with 57 patients, 53% overall (and 84% after severe pancreatitis) had pancreatic exocrine insufficiency (table⇓) and were thought to possibly benefit from pancreatic enzyme supplements.35 36 These should be given for at least six months, after which exocrine function can be tested by measuring faecal elastase levels. Endocrine insufficiency (diabetes) was less common but should also be considered. Functional recovery may continue for up to 12 months after the onset of pancreatitis, but further recovery after this time is unlikely. Most patients gain some additional useful exocrine function, but those with necrosis of a substantial proportion of pancreas may require supplements indefinitely.
Pancreatic exocrine insufficiency (PEI) and diabetes after acute pancreatitis in participants of two small observational studies
Additional educational resources
Information for healthcare professionals
References 1-4 contain detailed literature reviews of the clinical management of patients with acute pancreatitis
Cochrane Library (www.thecochranelibrary.com/details/browseReviews/578409/Acute.html)—contains several Cochrane reviews on aspects of pancreatitis
Information for patients
NHS UK (www.nhs.uk/Conditions/Pancreatitis/Pages/Introduction.aspx)—provides information for patients on the causes, symptoms, and treatment of acute pancreatitis
Patient.co.uk (www.patient.co.uk/health/acute-pancreatitis)—has information about the causes, symptoms, and treatment of acute pancreatitis
Notes
Cite this as: BMJ 2014;349:g4859
Footnotes
Contributors: All authors contributed to the design and planning of this manuscript, edited drafts, and approved the final version. CDJ wrote the manuscript and amended it in line with comments from the other authors. CDJ is the guarantor.
Competing interests: We have read and understood the BMJ Group policy on declaration of interests and declare the following interests: each author has recently contributed to evidence based reviews of diagnosis and management of acute pancreatitis. CDJ has conducted an evidence based review of the diagnosis and management of acute pancreatitis, and contributed to an international consensus on definitions and classification of the disease. MGB was the lead for development of guidelines for the management of acute pancreatitis for the International Association of Pancreatology and the American Pancreatic Association. RC is the joint lead of a working group of the United Kingdom and Ireland Pancreatic Guidelines Development Group.
Provenance and peer review: Commissioned; externally peer reviewed.