Article Text

Abstract
Objective Ten percent of adults presenting with iron deficiency anaemia (IDA) have underlying cancer. This analysis – the Iron Deficiency as an Indicator Of Malignancy (IDIOM) study – was undertaken to assess whether five simple clinical parameters can usefully predict the likelihood of gastrointestinal (GI) malignancy on subsequent investigation of patients with IDA.
Design Retrospective observational study, with multivariable analysis of the predictive value of sex, age, haemoglobin concentration (Hb), mean red cell volume (MCV) and iron studies for the risk of underlying GI malignancy.
Setting District General Hospital IDA clinic.
Patients 720 adults with confirmed IDA.
Results Sex, age and Hb were strongly associated with the risk of GI malignancy—the parsimonious model including only these variables yielded ORs of 4.0 (95% CI 2.3 to 7.0) for males compared with females; 3.3 (95% CI 1.7 to 6.4) for age >70 years compared with ≤70 years; and 5.3 (95% CI 2.4 to 11.7) for a Hb of ≤91.4 g/L compared with ≥111.5 g/L. Combining these risk factors identified a subgroup (12% of the study population) at particularly low risk (<2% likelihood), and a second subgroup (16% of the study population) at especially high risk (>20% likelihood) of underlying GI malignancy.
Conclusions Three simple and objective clinical parameters can be combined to provide a clinically useful cancer risk stratification model for subjects with IDA. This may assist with patient counselling and the prioritisation of investigational resources.
- Iron Deficiency
- Gastrointestinal Neoplasia
Statistics from Altmetric.com
Introduction
Iron deficiency anaemia (IDA) is a common clinical problem. In adult males or postmenopausal females, about 30% of subjects overall will have underlying gastrointestinal (GI) pathology. Malignancy accounts for about a third of these, about 10% of the total, often in the absence of localising symptoms.1–4
The IDA clinic at Poole Hospital has been operational since 2004, and is the point of referral for patients with IDA who have minimal or no symptoms to indicate the nature or location of the underlying cause of iron deficiency.5 Basic patient data have been collected since inception, for the purposes of clinical care, audit and service evaluation. The register now exceeds 1000 subjects.
It is inherently unlikely that all subjects with IDA will have the same pretest probability of malignancy, but without the tools to predict individual risk it is currently standard practice to recommend urgent investigation for IDA on the grounds that there might be an underlying malignancy.6 A simple but reliable pretest predictor of risk would help considerably with patient counselling. It could also facilitate better use of resources, with prioritisation of high-risk subjects for fast-track investigation and perhaps avoidance of investigation in particularly low-risk individuals.
Method
The aim of the study was to determine whether simple and objective clinical parameters could usefully identify subgroups of patients with IDA at particularly high and low risk of underlying malignancy of the GI tract. Given an overall prevalence of GI malignancy of about 10% in this patient population, it was decided—on a purely arbitrary basis—that identifying a low-risk subgroup with a cancer risk of <2%, and/or a high-risk subgroup with a cancer risk of >20%, might prove useful in clinical practice.
The study involved a retrospective analysis of clinical data for subjects on the Poole IDA clinic register assessed between June 2004 and May 2012 inclusive, who went on to have GI investigation and for whom information on the final diagnosis was available. Anonymised data were analysed using Predictive Analytics Software (PASW) to assess whether five clinical parameters—sex, age, haemoglobin concentration (Hb), mean red cell volume (MCV) and iron studies—could usefully predict the likelihood of GI pathology, and in particular malignancy, on subsequent investigation. Having viewed the protocol, the National Research Ethics Service advised that formal Research Ethics Committee approval was not required.
Age was categorised as a dichotomous variable (70 or less vs over 70 years), as the incidence of the major GI malignancies rises steeply after this age. An initial examination of the data revealed a striking stepwise increment in the prevalence of underlying cancer at around the age of 70 years—rising from 2.6% in the 60–69-years age group, to 11.6% in the 70–79-years age group. Hb and MCV were analysed as study population quartiles in order to obtain approximately equally sized groups, since there is no accepted way of categorising these variables—the quartiles are presented in order of increasing anaemia and microcytosis, respectively. Dichotomous outcome variables were created to indicate a diagnosis of malignant neoplasm, benign neoplasm over 1 cm in diameter (smaller lesions were felt unlikely to have made a significant contribution to the development of IDA), inflammatory disorder, vascular malformation or coeliac disease. A further outcome variable was created based on whether subjects had any of the above diagnoses.
Datasets were complete for sex, age, Hb, MCV and final diagnosis. Results for iron studies—transferrin saturation or serum ferritin or both—were available for 90% of the study population. The major reason for the absence of data for the remaining 10% was that iron supplements had been commenced prior to referral, without the relevant test being requested. Iron deficiency was therefore analysed as a dichotomous variable, being ‘severe’ (arbitrarily defined as a transferrin saturation <10%, a serum ferritin <10 µg/L or both) or ‘non-severe’ (criteria for severe deficiency not met).
Frequencies were run to provide descriptive information for the study population. Logistic regressions were used to investigate the associations with each explanatory variable on their own to obtain ORs, and together to adjust for all the other demographic and clinical characteristics. The parsimonious model was then selected for malignant neoplasm including only the factors that were significant (using a significance level of 5%) and 95% CIs were presented. The Nagelkerke R Square was used to assess the proportion of variance explained in the data, that is, a measure of how well the models fitted the data.
Results
Almost 1000 subjects were seen in the IDA clinic during the study period. Having excluded those in whom iron deficiency was not confirmed, or where investigations were not completed due to patient preference, frailty or concurrent illness, data for 720 persons were analysed. The study group comprised 433 women and 287 men, with a median age of 75 years (inter-quartile range 62–82 years). Of these, 219 (30.4%) were found on investigation to have at least one GI diagnosis considered to be clinically significant, and 68 (9.4%) had a GI malignancy.
Colorectal cancer accounted for 52/68 (76%) of the GI malignancies identified. Other underlying GI diagnoses in the study population were inflammatory disorders in 80 (11.1%), coeliac disease in 34 (4.7%), vascular malformations in 34 (4.7%) and benign neoplasia in 21 (2.9%). Some subjects had more than one diagnosis.
As shown in table 1, male sex, age >70 years, and severity of anaemia were all significantly associated with an increased risk of underlying GI malignancy on univariate analysis. Male sex and age >70 years were also significantly associated with an increased risk of ‘any underlying GI diagnosis’, but the relationships were not so strong, and the link with GI malignancy appeared to be driving these associations.
Odds ratios and significance levels for the associations between clinical characteristics and the outcomes of (a) gastrointestinal malignancy, and (b) any gastrointestinal diagnosis, in 720 subjects with iron deficiency anaemia, Poole Hospital 2004–2012
On logistic regression analysis with adjustment for other variables, sex, age and Hb remained significant independent predictors of the probability of underlying GI malignancy. Table 2 presents the results from the parsimonious model including only these variables. Men were four times more likely to be diagnosed with a GI malignancy than women, and subjects over 70 years old were three times more likely than those ≤70 years. Those with a Hb of 91.5–102.4 g/L were two-and-a-half times more likely, and those with a Hb of ≤91.4 g/L were five times more likely to be diagnosed with a GI malignancy than those with a Hb of ≥111.5 g/L.
ORs with 95% CI and p values for parsimonious logistic regression model of clinical variables associated with gastrointestinal malignancy, in 720 subjects with iron deficiency anaemia, Poole Hospital 2004–2012
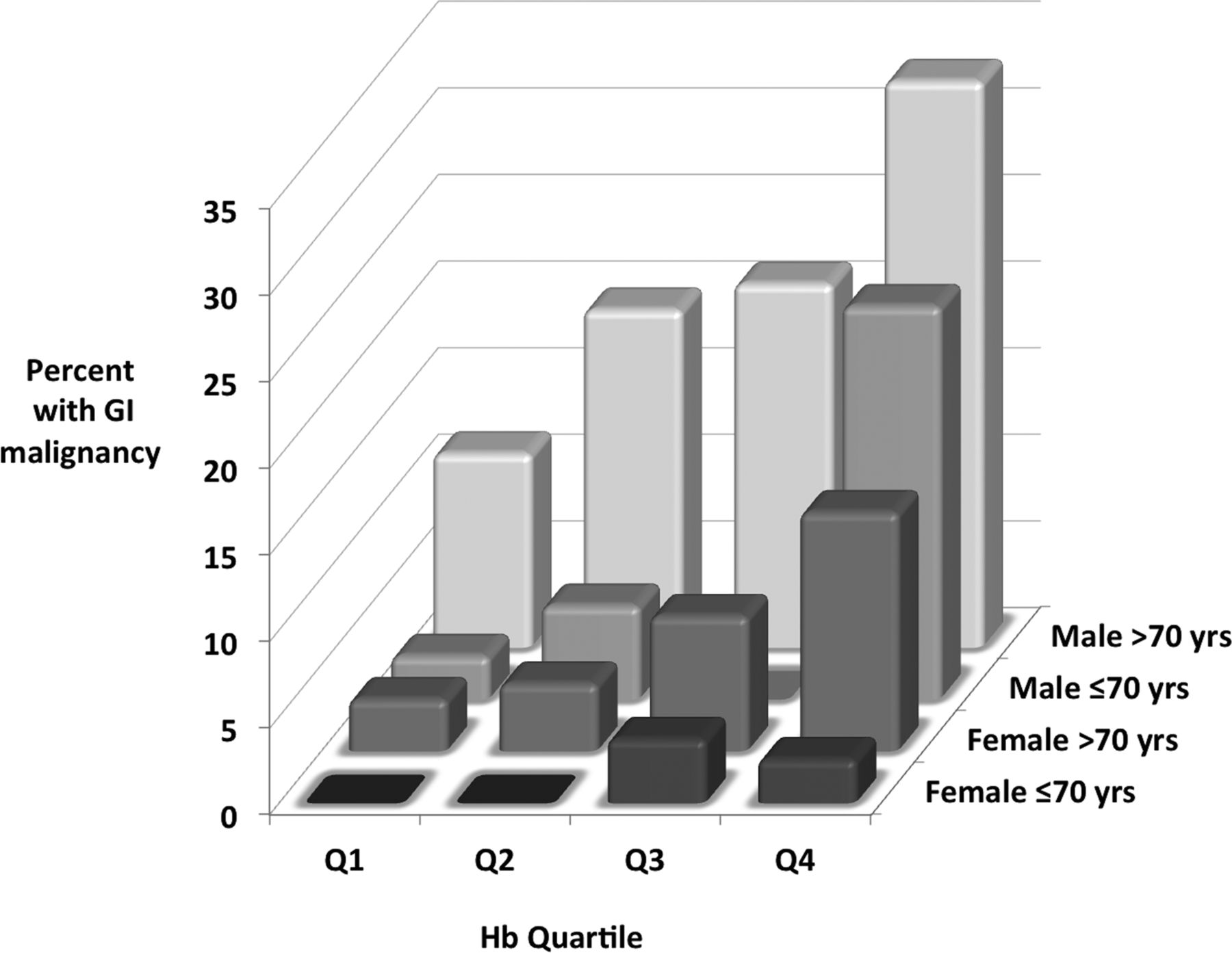
Combining the three predictive clinical variables provided a stronger indicator of the likelihood of GI malignancy than when considered in isolation. Individually, these three variables accounted for 5–7% of the variance in the data, while collectively they explained 18%. Broadly, there was an incremental increase in risk with increasing degree of anaemia within each of the four age/sex subgroups. The risk was generally greater for men than for women of the same age group and haemoglobin quartile (figure 1).

{kind=link}
The combination of the three clinical risk factors identified patient subgroups at the two ends of the spectrum of risk of underlying GI malignancy—those with cancer likelihoods exceeding the arbitrary thresholds of <2% and >20%. Specifically, younger women with mild anaemia (accounting for 12% of the study population) were at particularly low risk, while men with more severe anaemia (accounting for 16% of the study population) were at especially high risk of underlying GI malignancy (table 3).
The percentage prevalence (with 95% CIs) of gastrointestinal malignancy in 16 subgroups by sex, age and haemoglobin quartile of 720 subjects with iron deficiency anaemia, Poole Hospital 2004–2012
Discussion
IDA is a problem that is commonly encountered in current clinical practice.1–4 Our recent experience would suggest an increasing overall incidence that now approaches one case diagnosed per 1000 population per annum.5 The age-specific incidence of IDA in the elderly is considerably higher than this, and it is noteworthy that the median age of the study population was 75 years. This may of course reflect enhanced ascertainment due to the escalating number of requests for routine blood count estimations, particularly in the elderly.
Several mechanisms underlie the development of IDA, but the major categories are dietary insufficiency, malabsorption, and chronic low-grade haemorrhage from a mucosal surface. IDA in premenopausal women most commonly relates to dietary inadequacy and/or menstrual losses. About 30% of men and postmenopausal women, however, will prove to have significant underlying GI pathology, with malignancy accounting for about a third of these, often in the absence of clear clinical pointers to the diagnosis. Malignancy is undoubtedly the most important cause, and indeed it is the primary justification for the urgent investigation of subjects with IDA.1–6
Bidirectional endoscopy (BDE), combining gastroscopy and colonoscopy in the same session, is generally accepted as the most efficient method of assessing the GI tract in IDA unless there are clear clinical clues as to the cause.6 BDE is labour-intensive, however, taking up to one hour to complete for each patient. Furthermore, endoscopy carries a small but significant risk of complications, particularly in the elderly and those with major comorbidities.
Given that over 90% of endoscopic examinations in individuals with IDA will fail to reveal a GI malignancy, it is obviously important to consider the risk-benefit ratio for investigation of IDA on an individual case basis. There is, therefore, a need for a simple and reliable pretest predictor of the risk of underlying malignancy that is sufficiently discriminating to be clinically (and not just statistically) significant.
To the authors’ knowledge, there are only three published multivariate analyses of variables predictive of the risk of GI malignancy in IDA to date.7–9 The findings are summarised in table 4, along with those of the current study for comparison. There is universal agreement that age is a risk factor, but the findings for the other variables are somewhat discordant. However, two of the studies had a rather small sample size, and it is notable that the two largest studies are fully concordant for all five risk factors assessed. The findings from this current study confirm the results from the Nottingham study,9 identifying age, sex and Hb as independent variables predictive of underlying GI malignancy in IDA. This conclusion fits well with the findings of a large study using electronic primary care records employing a case-control methodology, which correlated age and degree of anaemia with colorectal cancer risk.10
Summary of published multivariate analyses of variables predictive of underlying gastrointestinal (GI) malignancy in subjects with iron deficiency anaemia
The predictive value of age and sex is not unexpected, given that the incidence of the major GI malignancies rises steeply after the age of 70 years, particularly in males.11 It may simply be that Hb is predictive of cancer risk because the nature of the pathology means that GI malignancy is disproportionately more likely than the other (non-malignant) causes of IDA to lead to greater degrees of anaemia. Why this is not reflected by the results of iron studies is less clear, though of course ferritin and transferrin saturation are surrogate markers of body iron stores, and may be influenced by other factors—serum ferritin, in particular, is an acute-phase protein, and may therefore be spuriously high in individuals with malignancy.
Given an overall probability of underlying GI malignancy of 10%, it was arbitrarily considered that identifying a low-risk subgroup with a cancer risk of less than 2%, and a high-risk subgroup with a cancer risk of greater than 20%, might be useful in clinical practice. The results suggest that over a quarter of subjects with IDA can be predicted to be of extremely low or high risk on the basis of these simple and objective clinical criteria. This may be of clinical relevance for patient counselling and prioritisation of investigations. It might also inform the decision as to whether to submit patients at extreme low risk to an invasive investigational strategy, though rigorous validation of the study results is essential before such a move can be contemplated.
The findings are unlikely to be the result of referral bias. Younger women with mild anaemia are probably the subgroup least likely to be referred unless there was some other reason for suspecting GI disease, for example, a positive family history of GI cancer. This might have been expected to result in a falsely high prevalence of GI malignancy in this subgroup, yet in the event the figure was 0%.
The study presented was retrospective and exploratory, carrying the inevitable issues associated with multiple significance testing. The limitations of multivariate analysis are also well established.12 Further work is clearly required to validate prospectively the predictive value of the risk factors identified, and this is underway. The results to date represent a first cut, using simple clinical information available from our IDA register. It is possible that additional clinical or laboratory variables could be added to improve the discriminatory capacity of the model still further—for example, a family history of GI malignancy, the use of aspirin, or faecal occult blood testing—and this avenue is also being explored.
In conclusion, this study has extended previous observations, confirming that sex, age and Hb are strong and independent predictors of the risk of underlying GI malignancy in subjects with IDA. It has also demonstrated that, in combination, these variables can identify over 25% of the study population who are at particularly high or low risk. The incremental nature of the model lends itself to the development of a simple scoring system for malignancy risk stratification that could be of practical value in a clinical setting.
What is already known on this topic
-
About 10% of adults with iron deficiency anaemia (IDA) have underlying gastro-intestinal malignancy, and clinical parameters may provide a guide to the likelihood of this.
What this study adds
-
Sex, age and haemoglobin concentration are independent predictors of cancer risk in IDA, and can be combined to provide a clinically useful cancer risk stratification model – with figures ranging from less than 2% in low-risk sub-groups to over 20% in high-risk sub-groups.
How might it impact on clinical practice in the foreseeable future
-
A simple and validated predictor of cancer risk in IDA would assist with patient counselling and the prioritization of investigational resources.
Acknowledgments
SLS, EJW and JAS conceived and designed this study. ACS and SLS collected the data and drafted the initial manuscript, while JAS was responsible for data collation. All authors made significant contributions to the subsequent revision of the paper, and have approved the final version prior to submission. We are grateful to Dr Nick Sharer for his constructive criticism of the manuscript.
Footnotes
-
Funding Poole Hospital Gastroenterology Research Fund.
-
Competing interests SLS and EJW have received honoraria for speaking at educational meetings sponsored by Pharmacosmos.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement The anonymised raw data for this study is available for sharing on application to the corresponding author.