Article Text

Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Non-alcoholic fatty liver disease (NAFLD) with advanced fibrosis is associated with an increased risk of overall and liver-specific mortality.
However, the risk of overall and cause-specific mortality across the full histological spectrum of NAFLD has yet to be established.
What are the new findings?
Among adults in Sweden with biopsy-confirmed NAFLD, the overall mortality rate was significantly elevated, compared with age, sex, county and calendar-year matched participants without NAFLD.
Significant excess mortality risk was found across all stages of NAFLD, and it increased progressively with worsening NAFLD severity.
This increased risk was primarily due to deaths from extrahepatic cancer and cirrhosis, while in contrast, the contributions of cardiovascular disease and hepatocellular carcinoma were relatively modest.
How might it impact on clinical practice in the foreseeable future?
These findings underscore the importance of reversing all stages of NAFLD.
Public health efforts focussed on the prevention of cancer and cirrhosis in patients with NAFLD should be prioritised.
Introduction
Non-alcoholic fatty liver disease (NAFLD) represents the most common cause of chronic liver disease in Western countries, affecting nearly 25% of U.S. and European adults.1 2 Nearly one-third of patients with NAFLD develop progressive steatohepatitis (non-fibrotic steatohepatitis (NASH)) and fibrosis, which can lead to cirrhosis, decompensated liver disease and death.3–5 Small clinical studies have demonstrated that among patients with NAFLD, advanced liver fibrosis, rather than inflammatory NASH, is the most important histological predictor of survival.4–8 Accordingly, current guidelines recommend that patients with NAFLD undergo risk stratification according to the presence or absence of significant fibrosis.7 However, robust, population-level data to support this strategy are lacking. Published evidence linking NAFLD histology to survival derives exclusively from studies with small, selected populations of less than 650 subjects and which recorded relatively few deaths, resulting in imprecise risk estimates and limited ability to comprehensively assess mortality.4 5 8–12 Thus, the precise impact of NAFLD histology on the long-term risk of overall and cause-specific mortality is still undefined. Given the growing burden of NAFLD, leveraging population-level data to quantify the magnitude of these risks is important for developing more effective strategies for prevention, surveillance and intervention.13
Thus, we evaluated the risks of overall and cause-specific mortality according to the presence and histological severity of NAFLD, in a population-based cohort comprising all adults in Sweden with biopsy-confirmed NAFLD. With complete, nationwide histopathology data and over 30 years of long-term follow-up, this cohort permits a more comprehensive assessment of mortality risk across the full histological spectrum of NAFLD.
Methods
We conducted a population-based, matched cohort study using the ESPRESSO (Epidemiology Strengthened by Histopathology Reports in Sweden) cohort. ESPRESSO includes prospectively-recorded liver histopathology data from all 28 Swedish pathology departments (1966 to 2017), and therefore is complete for the entire country of Sweden.14 Each report includes a unique personal identity number, biopsy date as well as topography within the liver and morphology. We then linked ESPRESSO to validated registers containing prospectively-recorded data regarding demographics, comorbidities, prescribed medications and death. ESPRESSO was approved by the Stockholm Ethics Board on 27 August 2014 (No.2014/1287-31/4). Informed consent was waived as the study was register-based.15
We identified all liver biopsy specimens from adults aged ≥18 years, submitted between 1966 to 2017, with topography codes corresponding to the liver, and Systematised Nomenclature of Medicine (SNOMED) codes corresponding to steatosis, without any other recorded aetiology of liver disease (online supplemental eMethods). Using a validated algorithm, we excluded anyone with another aetiology of liver disease, prior history of alcohol abuse/misuse, liver transplantation or emigration from Sweden before the index date, or with <180 days of follow-up (online supplemental figure S1). We further categorised NAFLD patients into four histological groups (ie, simple steatosis; NASH without fibrosis; non-cirrhotic fibrosis; and cirrhosis)(online supplemental eMethods).
Supplemental material
Supplemental material
Validation
We completed a validation study of 149 randomly-selected adults meeting criteria for biopsy-confirmed NAFLD. A physician (JFL) confirmed 137/149 to be NAFLD by reviewing free text from the pathologist (positive predictive value (PPV) of 92%). Additionally, we evaluated 119 different, randomly-selected adults and obtained PPVs of 90% (27/30) for simple steatosis, 87% (27/31) for NASH without fibrosis, 93% (28/30) for non-cirrhotic fibrosis and 97% (27/28) for cirrhosis.
Comparators
Each NAFLD patient was matched to up to five general population comparators without recorded NAFLD, according to age, sex, calendar year and county. Comparators were derived from the Total Population Register,16 and identical exclusion criteria were applied (online supplemental figure S1).
All-cause mortality was ascertained from the Total Population Register, which prospectively records 93% of all deaths within 10 days, and the remaining 7% within 30 days. Specific causes of death were retrieved from the Cause of Death Register,17 and categorised as: hepatocellular carcinoma (HCC) mortality, extrahepatic (ie, non-HCC) cancer mortality, cirrhosis mortality (excluding HCC), cardiovascular mortality and other causes of death (defined in online supplemental eMethods and table S2).
Online supplemental table S2 and eMethods contain detailed data regarding demographic, clinical and medication covariates. We ascertained age, sex, date of birth and emigration from the Total Population Register.16 Education level was obtained from the LISA (longitudinal integrated database for health insurance and labour market studies) database.18 Clinical comorbidities were collected from the Patient Register, which prospectively records all data from hospitalisations (including surgeries), discharge diagnoses (from 1964) and speciality outpatient care (from 2001) and is well-validated, with PPVs for clinical diagnoses that are consistently 85%–95%.19 The Prescribed Drug Register has prospectively recorded all prescriptions dispensed from Swedish pharmacies since 2005, and is well-validated and virtually complete,20 permitting accurate and comprehensive ascertainment of relevant medications, including statins, low-dose aspirin (<163 mg), antidiabetic and antihypertensive agents.20
Statistical Analysis
Our primary analyses evaluated all-cause and cause-specific mortality in patients with NAFLD compared with matched population controls, and according to NAFLD histological severity. Follow-up began ≥180 days after the index date, and continued to the first recorded date of death, emigration or end of follow-up (31 December 2017; cause-specific mortality, 31 December 2016). Population comparators who subsequently developed NAFLD were censored at that diagnosis date, and subsequently contributed person-time in the NAFLD group.
We constructed Kaplan-Meier curves to calculate incidence rates and absolute rate differences with 95% CIs. We also calculated 20-year absolute risks and risk differences, with 95% CIs approximated by the normal distribution. Using Cox proportional hazard models, we estimated multivariable adjusted HRs (aHRs), accounting for a priori-defined covariates (ie, age, sex, county, calendar year, education level, cardiovascular disease and the metabolic syndrome (as a 5-level variable: 1 point for diabetes, obesity, hypertension and/or dyslipidaemia))(online supplemental table S2). The proportional hazards assumption was assessed by examining the association between Schoenfeld residuals and time.
To assess specific underlying causes of mortality, we constructed cause-specific regression models. Furthermore, because cause-specific mortality may be overestimated in the setting of competing events,21 we repeated this analysis after accounting for other causes of death as competing risks. In stratified models, we examined the associations between NAFLD and both all-cause and cause-specific mortality according to known and putative risk factors for mortality, and we tested the significance of effect modification using the log likelihood ratio test.
To further characterise the potential gradient of mortality risk associated with progressive NAFLD histological severity, and to minimise potential bias related to the original indication for liver biopsy, we restricted the cohort to patients with histologically-defined NAFLD, with simple steatosis as the comparator. Additionally, because patients with advanced fibrosis were older than those with simple steatosis, we repeated this analysis after re-matching patients with simple steatosis 1:1 to individuals in each of the other NAFLD groups, by age (±2 years), sex, calendar year and county.
We conducted numerous sensitivity analyses to test the robustness of our results. First, we repeated our primary analyses after re-matching NAFLD patients to unaffected full siblings without NAFLD,16 to address potential confounding related to shared genetic or early environmental factors. Second, because a widely-used NAFLD histological scoring system was published in 2005,22 the year that medication data became available in Sweden, we restricted the cohort to index date ≥1 January 2006, and we adjusted for time-varying use of aspirin, statin and antidiabetic medications in our multivariable models. Third, to further address potential residual confounding, we constructed models additionally accounting for a modified Charlson Comorbidity Index (online supplemental eMethods), and also for incident diagnoses of alcohol abuse/misuse during follow-up (online supplemental table S1). Fourth, we censored anyone diagnosed with cancer within ≤180 days of follow-up, or anyone who died within <2 years. Finally, to further address potential residual confounding, we tested the sensitivity of our data to an unmeasured confounder.23
Statistical analyses were conducted using R software (V.3.6.1, R Foundation for Statistical Computing, Vienna, Austria; and survival package V. 2.44 (Therneau, 2015, https://CRAN.R-project.org/package=survival)). A two-sided p<0.05 was considered statistically significant.
Patient and public involvement
No patients were involved in setting the research question or the outcome measures. However, patients were involved in the establishment of the overall ESPRESSO cohort, which formed the foundation of this work. No patients were asked to advise on interpretation or writing up of results. The results of this research will be disseminated to patients by press release.
Results
Among 10 568 adults with histologically-confirmed NAFLD, 7105 (67.2%) had simple steatosis, 1218 (11.5%) had NASH without fibrosis, 1658 (15.7%) had non-cirrhotic fibrosis and 587 (5.6%) had cirrhosis (table 1). Among NAFLD patients, the average age at index biopsy was 52 years, and 44.8% were female. Compared with population comparators, NAFLD patients were more likely to have cardiovascular disease, diabetes, hypertension and dyslipidaemia (table 1). Median follow-up was 14.2 years among NAFLD patients, and 16.8 years among population comparators.
Characteristics of adults with histologically-defined NAFLD and matched population comparators at the index date
All-cause mortality
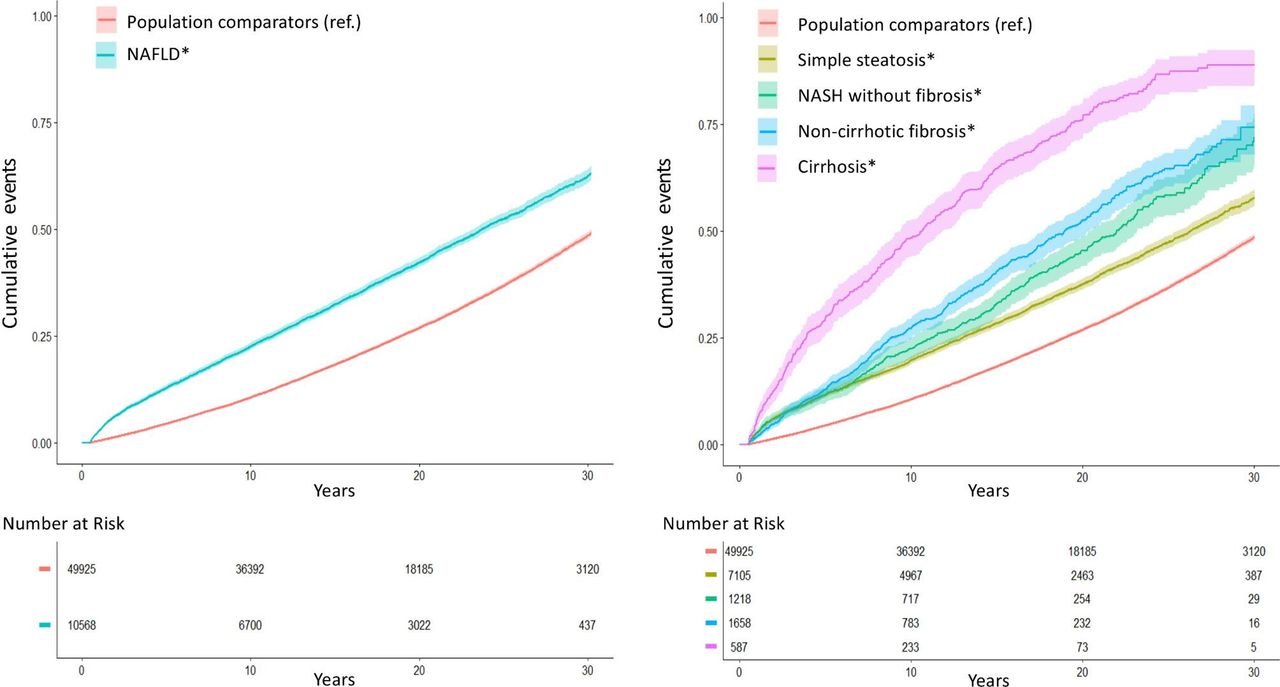
Overall, we documented 4338 deaths among NAFLD patients (28.6/1000 person-years (PY)), and 13 911 deaths among comparators (16.9/1000 PY) yielding an absolute rate difference of 11.7/1000 PY, and a 20-year absolute risk difference of 15.3% (95% CI=13.3 to 17.3)(table 2). After multivariable adjustment, NAFLD patients had a 1.93-fold higher risk of overall mortality, compared with population comparators (95% CI=1.86 to 2.00)(figure 1; table 2). The significant, positive association between NAFLD and increased risk of overall mortality was similar among women and men, and in patients with and without cardiovascular disease, diabetes, dyslipidaemia, hypertension or the metabolic syndrome (all pheterogeneity >0.05) (online supplemental figure S2). Hazard estimates for overall mortality were higher among patients diagnosed <60 years (vs ≥60 years), and those who died within the first 2 years of follow-up.
Supplemental material
{kind=link}
Cumulative incidence of all-cause mortality according to the presence and histological severity* of NAFLD. NAFLD, non-alcoholic fatty liver disease; NASH, non-alcoholic steatohepatitis; ref., reference group. *Histological severity of NAFLD was defined in four categories, as simple steatosis, NASH without fibrosis, non-cirrhotic fibrosis and cirrhosis (online supplemental eMethods).
All-cause mortality among adults with histologically-confirmed NAFLD and matched population comparators
Mortality risk increased with worsening NAFLD severity (ptrend <0.01) (figure 1; table 2). Compared with population controls, the absolute rates and corresponding aHRs for overall mortality were significantly elevated in all NAFLD patients, including those with simple steatosis (8.3/1000 PY, aHR=1.71, 95% CI=1.64 to 1.79), NASH without fibrosis (13.4/1000 PY, aHR=2.14, 95% CI=1.93 to 2.38), non-cirrhotic fibrosis (18.4/1000 PY, aHR=2.44, 95% CI=2.22 to 2.69) and cirrhosis (53.6/1000 PY, aHR=3.79, 95% CI=3.34 to 4.30). After 20 years, this corresponded to an absolute excess risk of overall mortality of 10.7% with simple steatosis, 18.5% with NASH without fibrosis, 25.6% with non-cirrhotic fibrosis and 49.4% with cirrhosis, compared with population controls. These findings were similar in men and women, and in those with and without cardiovascular disease, diabetes, hypertension, dyslipidaemia and metabolic syndrome (all pheterogeneity >0.05; not shown).
Cause-specific mortality
In both NAFLD patients and population controls, extrahepatic cancer and cardiovascular disease represented the two most common causes of death. Compared with controls, NAFLD patients had significantly higher rates of cause-specific mortality due to extrahepatic cancer (4.8 vs 9.3/1000 PY, aHR=2.16, 95% CI=2.03 to 2.30), followed by cirrhosis (0.2 vs 2.8/1000 PY, aHR=18.15, 95% CI=14.78 to 22.30), cardiovascular disease (6.9 vs 8.3/1000 PY, aHR=1.35, 95% CI=1.26 to 1.44) and HCC (0.1 vs 1.3/1000 PY, aHR=11.12, 95% CI=8.65 to 14.30)(table 3). Deaths from other causes were also more common among patients with NAFLD.
Cause-specific mortality among adults with histologically-confirmed NAFLD* and matched population comparators
We also evaluated cause-specific mortality according to NAFLD histological categories. Compared with population comparators, mortality rates from extrahepatic cancer, cirrhosis, cardiovascular disease and HCC were modestly but significantly elevated in simple steatosis (absolute rate differences, 4.4, 1.2, 0.7 and 0.7/1000 PY, respectively), and these rates increased progressively in NASH without fibrosis (3.9, 3.0, 2.7 and 1.3/1000 PY, respectively), non-cirrhotic fibrosis (4.5, 5.5, 1.8 and 2.5/1000 PY, respectively) and cirrhosis (6.5, 22.3, 8.2 and 5.5/1000 PY, respectively). After accounting for potential competing events (ie, other causes of death),21 we observed similar, dose-dependent gradients of increasing risk of extrahepatic cancer-related, cirrhosis-related and HCC-related mortality, with worsening NAFLD histological severity, consistent with our primary analysis (all ptrend <0.01) (online supplemental table S3). In contrast, after accounting for competing risks, NAFLD was no longer significantly associated with significant excess risk of cardiovascular mortality (aHR=0.98, 95% CI=0.92 to 1.04) nor was a dose-response relationship observed (ptrend=0.75).
NAFLD-only subgroup
After restricting the population to patients with biopsy-confirmed NAFLD, and using simple steatosis as the comparator, we observed a similar, dose-dependent relationship between worsening NAFLD histological severity and increased overall mortality (ptrend <0.01; table 4). Compared with simple steatosis, the aHRs with NASH without fibrosis, non-cirrhotic fibrosis and cirrhosis were, 1.14 (95% CI=1.03 to 1.26), 1.26 (95% CI=1.15 to 1.38) and 1.95 (95% CI=1.75 to 2.18), respectively.
Risk of all-cause mortality in the NAFLD-only subgroup*
We also assessed between-group differences in the absolute risk of overall mortality among patients with non-cirrhotic fibrosis, compared with those with NASH without fibrosis (figure 1, panel B). At 10 years, the cumulative incidence of all-cause mortality was significantly higher among patients with non-cirrhotic fibrosis (27.2 percentage points (95% CI=25.6 to 28.9)) compared with NASH without fibrosis (22.5 percentage points (95% CI=20.8 to 24.1); pdifference=0.041). However, at 20 years, this difference was no longer statistically significant (20-year cumulative incidence in patients with non-cirrhotic fibrosis versus NASH without fibrosis, 52.4 percentage points (95% CI=48.8 to 56.0) vs 45.4 percentage points (95% CI=42.1 to 48.7); pdifference=0.15).
We also evaluated cause-specific mortality according to NAFLD severity, within this NAFLD-only subgroup. Compared with patients with simple steatosis, the 20-year absolute excess risks of liver-specific, cardiovascular-specific and HCC-specific mortality were significantly higher in patients with NASH without fibrosis (3.3, 4.4 and 1.7%, respectively), non-cirrhotic fibrosis (6.8, 4.9 and 4.0%, respectively) and cirrhosis (30.4, 16.0% and 11.1%, respectively); in contrast, no significant between-group differences were found for cancer-specific mortality (online supplemental table S4).
Sensitivity analyses
Our findings were robust across all sensitivity analyses, including: (1) after matching NAFLD patients to full-sibling comparators (online supplemental table S5); (2) after restricting the index date to ≥1 January 2006, and further adjusting for time-varying medications (online supplemental table S6); (3) after constructing multivariable models additionally accounting for the modified Charlson Comorbidity Index (online supplemental table S7A,B), or incident alcohol abuse/misuse (aHRmortality for NAFLD=1.85, 95% CI=1.78 to 1.91); and (4) after excluding anyone diagnosed with cancer within ≤180 days (n=6258 excluded; aHRmortality=1.71, 95% CI=1.64 to 1.78). To further address potential reverse causation, and to account for the elevated HRs observed in persons with very short follow-up time, we also excluded anyone who died within <2 years of follow-up (n=1342 excluded), and our results were similar (aHRmortality=1.76, 95% CI=1.69 to 1.83). Finally, we observed that an unmeasured confounder would have to be both very strongly associated with mortality and highly imbalanced (ie, aHR <0.1 or≥4.5, with >50% difference in prevalence), to fully attenuate our results (online supplemental table S8).
Discussion
In this population-based cohort of 10 568 adults with biopsy-confirmed NAFLD and 49 925 matched general population comparators, NAFLD was associated with a 93% higher relative risk of overall mortality, and a 20-year absolute excess risk of 15.3%. Significantly elevated risk of overall mortality was apparent at all stages of NAFLD, and this risk increased in a dose-dependent manner with worsening histological severity. Specifically, 20-year absolute excess risk of mortality was 10.7% higher with simple steatosis, 18.5% higher with NASH without fibrosis, 25.6% higher with non-cirrhotic fibrosis and 49.4% higher with cirrhosis, compared with the general population. This excess risk was due primarily to increased cancer-specific and cirrhosis-specific mortality, while the contributions of cardiovascular disease-specific and HCC-specific mortality were relatively modest.
Although previous studies have linked NAFLD fibrosis to increased risk of mortality,4 5 8–12 those prior studies have been limited by small sample sizes, with few recorded deaths in each histological group, which yield imprecise risk estimates and poor generalisability.8–12 For example, in one of the largest published studies, 619 patients with biopsy-confirmed NAFLD were followed for a median of 12.6 years, and liver transplant-free survival did not differ significantly between patients with simple steatosis and those with non-fibrotic NASH (p=0.238).8 However, that analysis included only 12 deaths in the non-fibrotic NASH group. In contrast, the current study leveraged a complete, nationwide population of all adults in Sweden with histologically-defined NAFLD, and included longer follow-up time and more recorded deaths (4,338) than all prior NAFLD histology cohorts, combined.4 5
Currently, it is widely held that among patients with NAFLD, liver fibrosis is the only significant histological predictor of survival4 5 8–12; however, robust population-level evidence to support this hypothesis is lacking.13 Our data confirm this association in a nationwide, unselected population, and the significant, dose-response relationships that we observed across histological groups lend further support to a causal relationship. Furthermore, our large sample size permitted us to detect important differences in mortality rates between groups of patients with earlier stages of NAFLD, which was not possible in previous smaller histology cohorts. Specifically, compared with patients with simple steatosis, those with non-fibrotic NASH had an excess mortality rate of 5.1 per 1000 PY. While that figure might seem modest, over 20 years it translates to one additional death for every 10 patients diagnosed with non-fibrotic NASH. Thus, our findings suggest the need for more refined algorithms for risk stratification, surveillance and monitoring for patients with early-stage NAFLD.7
It has been established that liver-related mortality increases progressively with worsening NAFLD fibrosis.4 5 However, much less is known about the relationship between NAFLD histology and other specific causes of death. We observed that the increased mortality associated with NAFLD was driven primarily by excess risk of cancer-specific and cirrhosis-specific mortality, together with a small, although significant, excess risk of HCC-specific mortality. In contrast, the absolute excess risk of cardiovascular-specific mortality was modest, and it was no longer significant after accounting for competing events. Together, these data are consistent with recent studies highlighting the growing importance of fatal cancers and cirrhosis, as complications of NAFLD,4 11 24 25 and which suggest that the relationship between NAFLD and cardiovascular mortality might be less important than previously suggested.24 26–31 Indeed, while substantial evidence links NAFLD to an increased risk of non-fatal cardiovascular events,32 whether NAFLD contributes to excess cardiovascular mortality remains controversial.33 To date, two large meta-analyses have failed to demonstrate a significant association between NAFLD and cardiovascular mortality risk.29 34 Although a third meta-analysis found that NAFLD was significantly associated with an increased risk of both fatal and non-fatal cardiovascular events, that relationship was no longer statistically significant when analyses focussed specifically on cardiovascular mortality.35 Thus, while it remains important to carefully assess cardiovascular disease risk in patients with NAFLD,7 our data lend strong support to the development of public health efforts designed to prevent cancer and cirrhosis, for this growing patient population.
We considered whether the relationship between NAFLD and premature death merely reflected an association with the components of the metabolic syndrome. Consistent with other administrative data sets, the recorded prevalences of hypertension and obesity were low, which could lead to unmeasured confounding. Nevertheless, our findings remained similar in patients with and without these diagnoses, when compared with controls with the same comorbidities. Moreover, robust evidence demonstrates that hypertension, obesity and metabolic syndrome contribute only modestly to excess mortality risk (aHRs for hypertension, 1.09 to 1.3736–38; for overweight/obesity, 0.94 to 1.1839; and for the full metabolic syndrome, 1.58).40 Finally, our sensitivity analysis demonstrated that our results are robust to unmeasured confounding; specifically, a confounder would need to have both an aHR ≥4.5 for overall mortality and a >50% difference in prevalence between groups to attenuate our results. Thus, the excess mortality risk observed with NAFLD appears to far exceed that which could be explained by the metabolic syndrome alone.
This study benefits from a nationwide, unselected population with complete and prospectively-recorded histopathological data for the entire country of Sweden. We used strict and validated definitions of both NAFLD and confounding variables, in registers with near-complete follow-up for the entire Swedish population.16 Our large sample size and long follow-up permitted calculation of more precise, population-level risk estimates across NAFLD histological categories, while minimising the inherent limitations of previous, smaller studies. Conducting analyses exclusively in patients with histologically-defined NAFLD further reduced potential exposure misclassification or bias related to the indication for biopsy. Using cause-specific hazards models allowed for more comprehensive analyses of underlying causes of mortality. We also applied numerous analytical techniques to minimise bias from residual confounding, reverse causation, and competing events.
We acknowledge several limitations. First, this was a retrospective study, and NAFLD was defined histologically; nevertheless, our case distribution, hazard estimates and absolute rate differences between histology categories accord with prior studies8–12 including a recent meta-analysis,5 which argue against selection bias and underscore the generalisability of our results. Second, it is possible that the influence of NAFLD on cause-specific mortality may differ if NAFLD is diagnosed using non-invasive parameters; however, our findings are broadly consistent with prior population-based studies in which NAFLD was defined by ultrasound41 or administrative codes.24 Third, pathology data may be subject to sampling error and interobserver variability, and we lacked detailed data regarding the length and number of portal tracts in each biopsy; however, our validation study demonstrated the accuracy of our exposure definition, and we would emphasise that any non-differential misclassification would most likely attenuate a true association. Fourth, despite careful matching and multivariable adjustment for clinical, demographic and medication confounders, residual confounding is possible, and we lacked detailed data regarding individual stages of non-cirrhotic fibrosis, smoking, alcohol consumption, body mass index (BMI) or laboratory values. However, our findings were robust in patients with and without clinical comorbidities, after re-matching NAFLD patients with full siblings, and after further accounting for incident alcohol abuse/misuse or a validated comorbidity index. Moreover, we demonstrated that an unmeasured confounder like BMI would need to be more strongly associated with mortality than previously described42 and also very highly imbalanced (ie, both aHR ≥4.5 and>50% difference between groups) to attenuate our results. Fifth, the Swedish population is primarily Caucasian, underscoring the need for research in diverse populations. Finally, although changing trends in NAFLD diagnostic strategies could have impacted our findings, all models accounted for calendar year, and our results were similar in recent time periods and in the NAFLD-only subgroup.
In conclusion, within a population-based cohort, all histological stages of NAFLD were associated with significantly increased risk of overall mortality, which increased in a dose-dependent manner with worsening NAFLD severity. Most of the excess mortality associated with NAFLD was from non-HCC cancer and cirrhosis, while in contrast, the contributions of cardiovascular disease and HCC were relatively modest. Our findings underscore the importance of reversing all stages of NAFLD, while also highlighting the need for effective public health strategies designed to prevent cancer and cirrhosis, in this high-risk and growing population.
Data availability statement
No additional data are available due to Swedish regulations.
Ethics statements
Ethics approval
This study was approved by the Regional Ethics Committee, Stockholm, Sweden (Protocol number: 2014/1287-31/4).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been corrected since it published Online First. Figure 1 has been amended.
Contributors Guarantor: The corresponding author (JFL) had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: All co-authors. Acquisition of data: JFL. Analysis: BR. Interpretation of data: All co-authors. Writing first draft of the manuscript: TS and JFL. Critical revision of the manuscript for important intellectual content and approval of final version: All co-authors.
Funding TS was supported by NIH K23 DK122104. TS was supported by the Harvard University Center for AIDS Research (CFAR). HH was supported by grants from Region Stockholm (postdoctoral appointment). HK was supported by the Crohns and Colitis Foundation Senior Research Award. JFL was funded by the Karolinska Institutet (institutional award).
Competing interests JFL coordinates a study on behalf of the Swedish Inflammatory Bowel Disease quality register (SWIBREG), that has received funding from Janssen Corporation. HH reports research grants to his institution from AstraZeneca, Intercept and Gilead, and board advisory for Bristol Myers Squibb and Gilead. TS has served as a consultant to Aetion for work unrelated to this manuscript.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.