Article Text

Abstract
Objective Recent data have suggested that non-selective β-blockers (NSBB) are associated with increased mortality in patients with cirrhosis and refractory ascites. However, other evidence implies that NSBB may be beneficial in this setting by reducing bacterial translocation. Our aim was to determine whether NSBB use was a risk factor for mortality in patients with end-stage chronic liver disease and ascites awaiting liver transplantation.
Design This was a single-centre retrospective study of 322 patients with ascites listed January 2007 to July 2011.
Results NSBB patients (n=159) and non-NSBB patients (n=163) were comparable with regards to listing model for end-stage liver disease score (p=0.168), frequency of hepatocellular carcinoma (p=0.193) and refractory ascites (35.2% vs. 37.4%, p=0.681). 82 patients died, 221 patients were transplanted and 19 patients were removed from the list during a median follow-up duration of 72 days; the median time to death was 150 and 54 days in the NSBB and non-NSBB groups, respectively. In a multivariate competing risk Cox model, patients on NSBB had reduced mortality compared with propensity risk score-matched non-NSBB patients (HR 0.55; 95% CI 0.32 to 0.95, p=0.032). Similarly, in the subgroup of patients with refractory ascites (n=117), NSBB remained independently associated with less waitlist death (adjusted HR 0.35; 95% CI 0.14 to 0.86, p=0.022).
Conclusions NSBB in patients with ascites and refractory ascites listed for liver transplantation are not detrimental, and instead are associated with reduced waitlist death. Our findings argue that NSBB are safe and may confer benefit in patients with ascites complicating end-stage liver disease.
- LIVER TRANSPLANTATION
- ASCITES
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Recent observational data have suggested that non-selective β-blockers (NSBB) are associated with increased mortality in patients with cirrhosis and refractory ascites.
However, NSBB reduce the frequency of portal hypertension-related complications and may independently reduce bacterial translocation and the secondary systemic inflammatory response.
Given progressive waiting times and an increasing need to optimise waitlist survival, the debate regarding NSBB in patients with ascites awaiting transplantation is especially relevant.
What are the new findings?
Patients with end-stage liver disease and ascites awaiting liver transplantation receiving NSBB had reduced mortality compared with matched non-NSBB patients.
Similarly, in the subgroup of patients with refractory ascites, NSBB remained independently associated with less waitlist death.
How might it impact on clinical practice in the foreseeable future?
We recommend that NSBB should be continued in patients with end-stage liver disease and ascites or refractory ascites awaiting liver transplantation unless intolerant.
These findings argue that NSBB are safe and may confer benefit in patients with ascites complicating end-stage liver disease.
Introduction
Non-selective β-blockers (NSBB) are frequently prescribed in patients with decompensated chronic liver disease in an effort to reduce morbidity and mortality. Via a decrease in cardiac output (β1-blockade) and splanchnic vasoconstriction (β2-blockade with unopposed α1 agonism),1 NSBB lower portal pressure and have been demonstrated to reduce the frequency of portal hypertension-related complications. NSBB lessen the risk of first variceal haemorrhage compared with placebo with similar efficacy to endoscopic therapy, while the combination of NSBB and endoscopic treatment is associated with a lower rate of rebleeding after variceal haemorrhage than endoscopic therapy alone.1–5 Several meta-analyses have confirmed survival advantage of NSBB over placebo, both before and after the occurrence of variceal bleeding.3 ,6 More recently, haemodynamic response to β-blockade has also been linked with a lower probability of the development of ascites, refractory ascites and hepatorenal syndrome.7 ,8
Importantly, the benefits of NSBB in patients with cirrhosis may not be exclusively attributable to the effects on portal pressure alone. NSBB reduce markers of intestinal permeability, bacterial translocation and systemic inflammation, and reduce the risk of spontaneous bacterial peritonitis.9 ,10 Such associations are observed in the absence of a fall in portal pressure, suggesting that NSBB modulate gut mucosal integrity directly.9 ,10 The systemic inflammatory response is increasingly recognised as a pathogenetic factor in the circulatory dysfunction of advanced cirrhosis; patients with Child-Pugh Class C disease have a greater frequency of bacterial translocation, and patients with ascites with evidence of endotoxemia have more pronounced circulatory dysfunction.11 ,12 Long-term prophylactic antibiotics reduce the incidence of hepatorenal syndrome and improve survival, independent of the prevention of overt infection.13 Therefore, it follows that in patients with advanced liver disease NSBB may also have a positive impact on non-bleeding-related mortality.
Despite these encouraging findings, Serste et al14 ,15 have in recent years questioned the benefits of NSBB in end-stage cirrhosis. They observed that in patients with refractory ascites NSBB were associated with greater all-cause mortality and hypothesised that NSBB increase the susceptibility to paracentesis-induced circulatory dysfunction.14 Supporting this postulation, in a small pilot study, patients receiving NSBB had an impaired chronotropic response to large volume paracentesis and increased incidence of circulatory dysfunction.15 Other authors have suggested that systolic dysfunction and a relatively low cardiac output state, insufficient to maintain arterial blood pressure and renal perfusion, may be contributing.16 Nevertheless, the suggestion that NSBB should be contraindicated in these patients has been widely challenged by the hepatology community. Concerns have been raised regarding the methodology of the original observational study.14 In particular, the NSBB patients appeared to be sicker at baseline than the non-NSBB patients, and it is difficult to link causality between NSBB and the main reasons for death.17–20 As a result, it remains unclear whether NSBB should be continued in this setting.
Ascites is common in patients with end-stage cirrhosis listed for liver transplantation. Given progressive waiting times and an increasing need to optimise waitlist survival, the debate regarding NSBB in patients with ascites awaiting transplantation is especially relevant. The aim of this study was, therefore, to determine whether NSBB at listing are a risk factor for mortality in patients with ascites awaiting liver transplantation.
Methods
This was a single-centre retrospective study of consecutive patients with ascites listed for first elective liver transplantation January 2007 to June 2011. Patients listed for acute liver failure, combined liver–kidney transplantation or retransplantation, or who had a transjugular porto-systemic shunt in situ (n=20) were excluded from the analysis. Furthermore, those prescribed a selective β-blocker were not assessed (n=14). The study cohort comprised 322 patients.
Patients were identified from a prospectively collected database. The following variables at the time of listing for liver transplantation were recorded: age, gender, blood group, weight, height, aetiology of liver disease, hepatocellular carcinoma, presence of diabetes mellitus, previous variceal haemorrhage and laboratory data (serum bilirubin, albumin, international normalised ratio, creatinine, serum sodium). The prescription and type of NSBB was documented. Our unit is a tertiary referral centre, and, in most cases, the patients who were on an NSBB were already on the NSBB at the time of referral. In the UK, the indications for NSBB in patients with chronic liver disease are primary prophylaxis of oesophageal variceal haemorrhage (endoscopic evidence of grade II or above), and frequently the secondary prophylaxis of variceal haemorrhage in addition to endoscopic therapy.1 ,2 NSBB are started at a low dose and titrated to the maximum tolerated. Practice varies substantially however, and our unit rarely alters the management of the referring hepatologist. The administration of long-term antibiotic prophylaxis was also recorded. The indication for antibiotics was usually the secondary prophylaxis of spontaneous bacterial peritonitis or end-stage liver disease.2 ,13 Again, this is clinician dependent. All patients had a clinical history consistent with, and radiographic evidence of, ascites. Refractory ascites and type 2 hepatorenal syndrome were defined according to the International Ascites Club criteria.21 ,22 Hyponatraemia was defined as a serum sodium <135 mmol/L. The model for end-stage liver disease (MELD) score was determined.23 The UK Score for Patients with End-Stage Liver Disease (UKELD), a recently devised scoring system that incorporates serum sodium in addition to the MELD variables used routinely in the UK to prioritise graft allocation, was also calculated.24 Glomerular filtration rate was estimated (eGFR) using the modification of diet in renal disease (MDRD) study four-variable equation (eGFR=186×creatinine(mg/dL)−1.154×age(years)−0.203×1.212(if black)×0.742(if female)).25
Towards the end of the study period, blood pressure was recorded routinely on our computerised database. Therefore, in a subgroup of patients, blood pressure data were available.
Statistical analyses
Normally distributed continuous variables and non-parametric continuous variables were compared using Student t test and Mann–Whitney test, respectively. χ2 analysis or Fisher's exact test was used for comparison of categorical data. Survival modelling was performed using Cox proportional hazards analysis. The outcome of interest was death. In the first instance, traditional Cox modelling was performed with patients censored at the time of liver transplantation, removal from the list because of clinical improvement or refusal, or last follow-up if still active. Thereafter, competing risk Cox regression analysis was used according to the method of Fine and Gray.26 In patients listed for liver transplantation, the outcome transplantation is a competing risk that may impact on the probability of death, and vice versa. Competing risk analysis provides event-specific (death or transplant) HRs that are adjusted for interdependence. Competing risk analysis is considered the most appropriate statistical method for assessing the relationship between covariates and death in patients on a transplant waiting list, while traditional Cox regression analysis estimates the probability of death in the absence of transplantation.27 In the competing risk analysis, patients were censored at the time of removal from the list because of clinical improvement or refusal, or last follow-up if still active. Covariates with p≤0.200 on univariate competing risk analysis were included simultaneously in the multivariate models.
In view of probability of selection bias, the analysis was repeated in a cohort of NSBB and non-NSBB propensity risk score (PRS)-matched patients. Matching patients by PRS is a recognised method of controlling for selection bias.28 ,29 A PRS for NSBB use versus no NSBB use was generated by non-parsimonious multiple logistic regression. This model included all variables at the time of listing of clinical relevance to the outcome measure waitlist mortality (age, gender, diagnosis, hepatocellular carcinoma, body mass index, MELD score, serum sodium, eGFR, refractory ascites, previous variceal haemorrhage, prophylactic antibiotic use), as well as the five interaction terms with p≤0.100 (gender×variceal haemorrhage, serum sodium×MELD, serum sodium×variceal haemorrhage, refractory ascites×prophylactic antibiotics, hepatocellular carcinoma×eGFR). The c-statistic of the PRS for NSBB was 0.723 (95% CI 0.67 to 0.78). The nearest available matching (1:1) on the estimated PRS method was used to construct the control group with a calliper width of 0.2 of the SD of the logit of the propensity score.28 ,30 After matching, appropriate paired tests were used (the paired t test with non-parametric variables transformed into their natural logarithms and the McNemar test for dichotomous variables). Balance was achieved between the NSBB (n=104) and non-NSBB (n=104) groups on the recognised confounders (table 1).31 Due to the importance of, for example, MELD as a predictor of mortality, it was included both in the PRS model for the pairing of patients and in the multivariable survival analysis models. By considering the variable twice, there is a risk of overfitting. However, since the models based on both paired and unpaired data yielded similar results, it was concluded that any effect of overfitting was negligible.
Characteristics of patients with ascites at the time of listing for liver transplantation subdivided according to the presence or absence of NSBB
UKELD was implemented in the second half of the observation period. Separate models were constructed with UKELD substituted for MELD and hyponatraemia to ensure that this did not alter any association between NSBB and death. All analyses were repeated in the subgroup of patients with refractory ascites. Bootstrapping was used to confirm the validity of the results.
Data were analysed using the SPSS 21 package (SPSS Inc, Chicago, Illinois, USA), except the competing risk analyses, which were performed using Stata V.13.1 (Stat Corp, College Station, Texas, USA). All values are expressed as mean and SD, and median and IQR as appropriate. p<0.05 was considered statistically significant. Where data are analysed using multiple methodologies, such as Cox regression and competing risk survival analyses, unadjusted p values are quoted throughout. This is since adjustments for multiple comparisons assume that many independent analyses are being performed as opposed to correlated analyses based on the same underlying data. A post hoc power calculation is detailed in online supplementary statistics 1.
Results
The mean age of the entire cohort was 54.1 (SD 9.7) years (men:women=1.8:1), and the mean listing MELD score was 17 (SD 5). The prevalence of refractory ascites was 36.3%. Non-refractory and refractory patients with ascites are compared in online supplementary table S1.
In total, 82 patients (25.5%) died, 221 patients (68.6%) were transplanted and 19 patients (5.9%) were removed from the list during a median follow-up time of 72 (IQR 27–162) days. The estimated 6-month and 12-month survival was 69.4% and 49.2%, respectively. The documented causes of death were liver failure (46 patients), sepsis (14 patients), multiorgan failure cause unspecified (7 patients), cardiac (4 patients), tumour (2 patient), gastrointestinal haemorrhage (1 patient) and other (8 patients).
A total of 159 patients (49.4%) were on an NSBB; 119 patients (74.8%) were taking propanolol and 40 patients (25.2%) were prescribed carvedilol. The median dose of propanolol was 80 (range 10–240) mg per day, and the median dose of carvedilol was 6.25 (range 3.125–12.5) mg per day.
Comparison of NSBB and non-NSBB patients
Baseline characteristics of the two patient groups are outlined in table 1. NSBB and non-NSBB patients were comparable with regards to listing MELD score (p=0.168) and frequency of hepatocellular carcinoma (p=0.193), refractory ascites (p=0.681) and type 2 hepatorenal syndrome (p=0.830). NSBB patients, however, had a higher serum sodium (p=0.016) reflected in a lower UKELD score (p=0.014) and were more likely to have had a previous variceal haemorrhage (p=0.003).
A total of 104 NSBB patients (65.4%) and 103 non-NSBB patients (63.2%) were prescribed regular diuretic therapy (p=0.678). The most common diuretic used was spironolactone (92.8% of all patients receiving diuretics), followed by frusemide (40.1%). Diuretic therapy was less likely in patients with refractory ascites (refractory ascites 49.6%; non-refractory ascites 72.7%; p<0.001). There was no difference in the median dose of spironolactone per day between the NSBB and non-NSBB groups (NSBB 100 (100–200) mg; non-NSBB 100 (100–200) mg, median (IQR); p=0.946). Similarly, there was no difference in the median dose of frusemide per day (NSBB 40 (40–80) mg; non-NSBB 40 (40–65) mg, median (IQR); p=0.648). The frequency of dual diuretic prescription was 23.3% in NSBB patients and 23.9% in non-NSBB patients (p=0.890).
Blood pressure data were available in 81 patients (25.2%; 43 NSBB patients and 38 non-NSBB patients). Baseline systolic blood pressure (NSBB 115 (13) mm Hg; non-NSBB 122 (20) mm Hg, mean (SD); p=0.036), but not diastolic blood pressure (NSBB 71 (7) mm Hg; non-NSBB 73 (11) mm Hg, mean (SD); p=0.371), was lower in the NSBB group.
The outcome after listing was death in 22.0% of NSBB patients and 28.8% of non-NSBB patients, and transplantation in 73.6% of NSBB patients and 63.8% of non-NSBB patients. The median time to death in the NSBB group was 150 (IQR 56–351) days and in the non-NSBB group it was 54 (IQR 27–148) days. The median time to transplantation was 76 (IQR 29–161) days and 44 (IQR 15–132) days for the NSBB and non-NSBB patients, respectively. There was no difference in the frequency of cause of death between the NSBB and non-NSBB patients (p=0.540, see online supplementary table S2).
Predictors of death after listing for liver transplantation in patients with ascites
Variables associated with death on univariate analysis are presented in table 2. In a multivariate Cox regression model adjusting for clinically relevant variables, patients with ascites on NSBB had reduced mortality in the absence of transplantation compared with non-NSBB patients (HR 0.53; 95% CI 0.34 to 0.84, p=0.007, table 3). When transplantation was considered as a competing risk, there was no relationship between NSBB and death (HR 0.70; 95% CI 0.45 to 1.10, p=0.119). In this model, variables associated with mortality were hyponatraemia (p=0.010) and no antibiotic prophylaxis (p=0.013), and variables associated with transplantation were increasing MELD score (p=0.017), hepatocellular carcinoma (p=0.002) and antibiotic prophylaxis (p=0.003).
Univariate Cox regression analysis of variables associated with death in all patients after listing for liver transplantation
Multivariate Cox regression analysis of variables associated with death after listing for liver transplantation in all patients with ascites
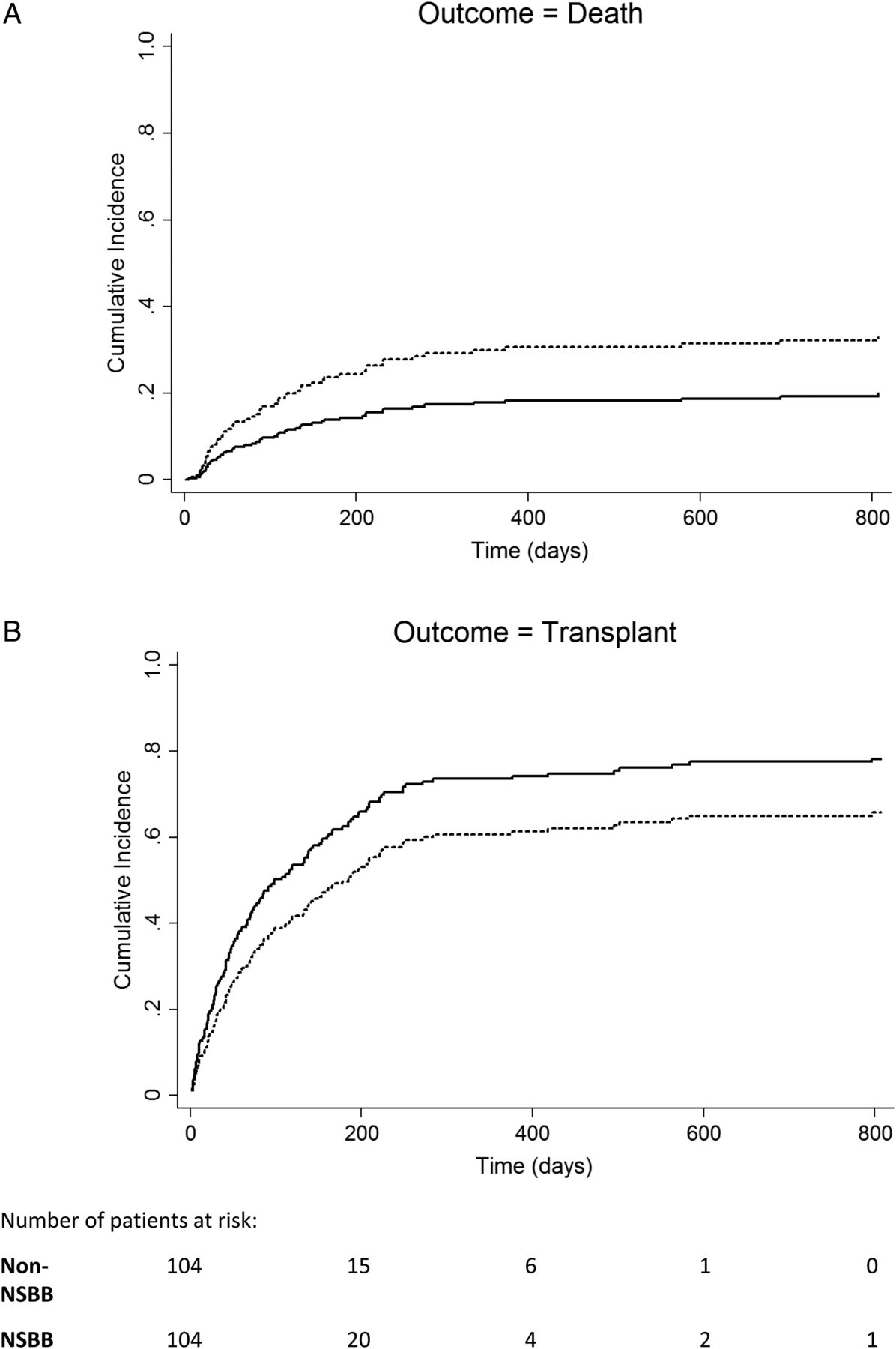
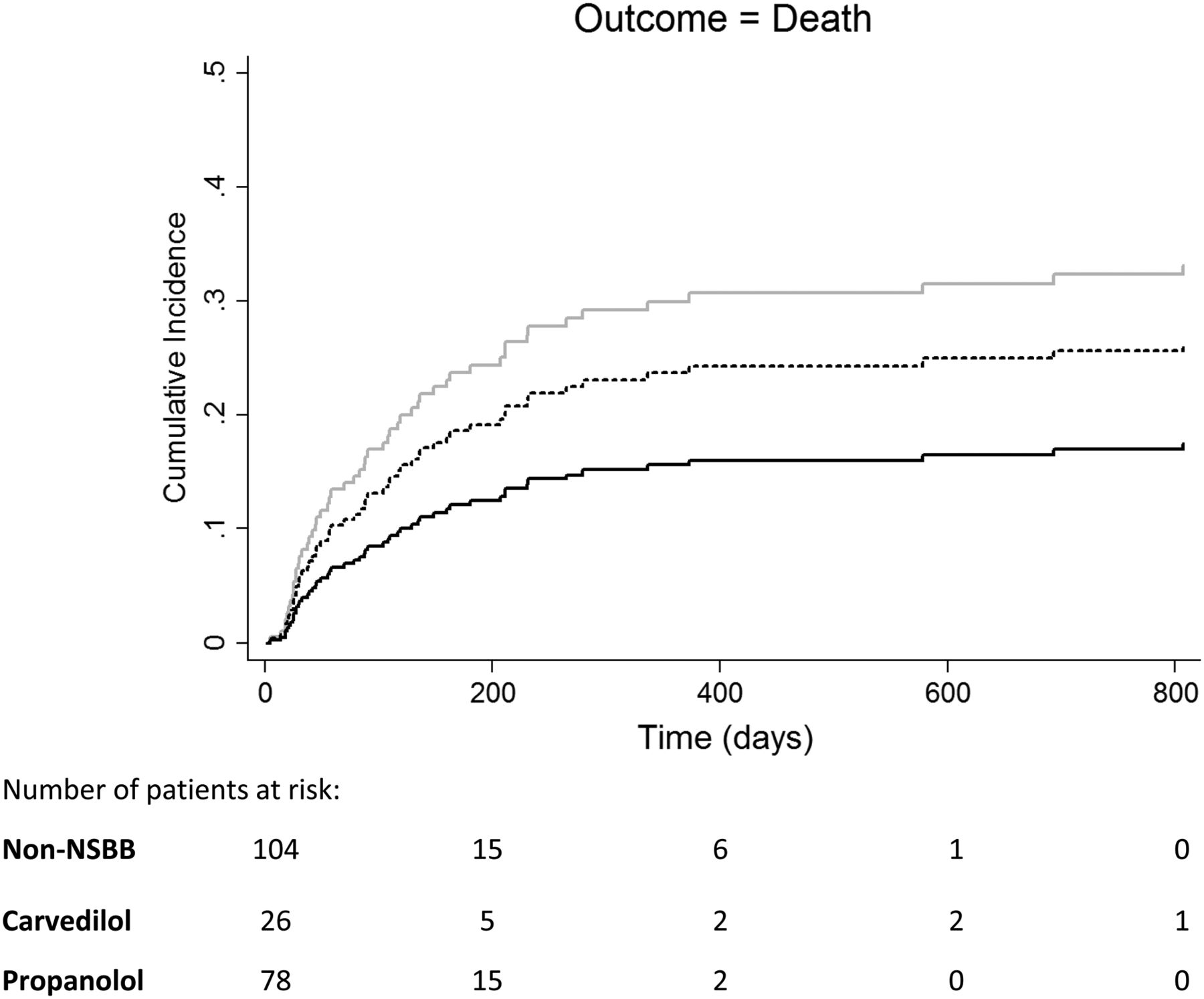
Given the observed differences between the NSBB and non-NSBB groups at baseline, a cohort of NSBB patients (n=104) and non-NSBB patients (n=104) matched by PRS were then identified. PRS matching is a recognised method of controlling for selection bias. The PRS-matched groups were comparable with regards to baseline characteristics, in particular listing MELD score (p=0.810) and serum sodium (p=0.814) (table 1). In a multivariate competing risk Cox model, patients with ascites on NSBB had reduced waitlist mortality compared with matched non-NSBB patients with ascites (adjusted HR 0.55; 95% CI 0.32 to 0.95, p=0.032, table 4 and figure 1) and were more likely to undergo transplantation (adjusted HR 1.42; 95% CI 1.01 to 1.99, p=0.041). Substitution of MELD and hyponatraemia with UKELD did not affect the statistical relationship between NSBB and death (competing risk-adjusted HR 0.58; 95% CI 0.34 to 1.00, p=0.050). When subdivided according to the β-blocker type, patients receiving propanolol and carvedilol had a lower cumulative incidence of waitlist mortality compared with non-NSBB patients (figure 2).
Multivariate Cox regression analysis of variables associated with death after listing for liver transplantation in PRS-matched patients with ascites

Cumulative incidence of (A) death and (B) transplantation in propensity risk score-matched patients with ascites listed for liver transplantation subdivided based on the presence of non-selective β-blockers (NSBB) (solid line) or absence of NSBB (dashed line). Cumulative incidence calculated using competing risk analysis and adjusted for model for end-stage liver disease score, hyponatraemia, hepatocellular carcinoma, previous variceal haemorrhage and prophylactic antibiotics.

Cumulative incidence of death in propensity risk score-matched patients with ascites listed for liver transplantation subdivided based on the presence of propanolol (solid black line), carvedilol (dashed line) or absence of non-selective β-blockers (NSBB) (solid grey line). Cumulative incidence calculated using competing risk analysis and adjusted for model for end-stage liver disease score, hyponatraemia, previous variceal haemorrhage and prophylactic antibiotics.
Predictors of death after listing for liver transplantation in patients with refractory ascites
The analysis was then repeated in patients with refractory ascites only (n=117). There was no difference in the bilirubin (NSBB 47 (28–65) μmol/L; non-NSBB 46 (26–115) μmol/L, median (IQR); p=0.393), MELD score (NSBB 15 (4); non-NSBB 17 (5), mean (SD); p=0.079) or frequency of hepatocellular carcinoma (NSBB 5.4%; non-NSBB 6.6%; p=0.548) between patient groups. Serum sodium was however higher in the NSBB patients (NSBB 134 (6) mmol/L; non-NSBB 132 (5) mmol/L, mean (SD); p=0.018).
The outcome after listing was death in 23.2% of NSBB patients and 34.8% of non-NSBB patients, and transplantation in 73.2% of NSBB patients and 59.0% of non-NSBB patients. The median time to death in the NSBB group was 159 (IQR 121–315) days and in the non-NSBB group it was 52 (IQR 26–164) days. The median time to transplantation was 67 (IQR 29–142) days and 46 (IQR 17–113) days for the NSBB and non-NSBB patients, respectively.
On multivariate competing risk analysis of patients with refractory ascites, those receiving NSBB had reduced waitlist mortality relative to patients not receiving NSBB (adjusted HR 0.49; 95% CI 0.25 to 0.96, p=0.038, table 5). In the subgroup of PRS-matched patients with refractory ascites, NSBB and non-NSBB groups were matched for confounders (data not shown). In a multivariate model including only PRS-matched patients with refractory ascites, NSBB use remained associated with a lower risk of mortality (adjusted HR 0.35; 95% CI 0.14 to 0.86, p=0.022, table 6 and figure 3). Substitution of MELD and hyponatraemia with UKELD in this model did not affect the statistical relationship between NSBB and death (competing risk-adjusted HR 0.34; 95% CI 0.14 to 0.85, p=0.021).
Multivariate Cox regression analysis of variables associated with death after listing for liver transplantation in all patients with refractory ascites
Multivariate Cox regression analysis of variables associated with death after listing for liver transplantation in PRS-matched patients with refractory ascites

{kind=link}
{kind=link}
{kind=link}
Cumulative incidence of death in propensity risk score-matched patients with (A) refractory ascites and (B) non-refractory ascites listed for liver transplantation subdivided based on the presence of non-selective β-blockers (NSBB) (solid line) or absence of NSBB (dashed line). Cumulative incidence calculated using competing risk analysis and adjusted for model for end-stage liver disease score, hyponatraemia, hepatocellular carcinoma, previous variceal haemorrhage and prophylactic antibiotics.
Discussion
In this large single-centre observational study, we have examined for the first time the implications of NSBB for mortality in patients with ascites awaiting liver transplantation. Importantly, we have shown that patients receiving NSBB at listing have reduced transplant-free mortality and waitlist death compared with PRS-matched patients not receiving NSBB. In particular, in the subgroup of patients with refractory ascites, NSBB use was associated with a lower probability of death during follow-up. These findings suggest that NSBB may confer benefit in patients with end-stage liver disease and ascites.14
The apparent contradictory observations to those published by Serste et al14 may possibly be explained by the different populations studied. Our patients were a highly select cohort, active on a liver transplant waiting list, free of significant comorbidity and considered fit enough to survive transplant surgery. On the other hand, in the French study, patients had been hospitalised with refractory ascites, potentially with superimposed precipitants for decompensation such as infection that were not reported.14 Moreover, given their older age subclinical cardiac disease could have contributed to the results, which is actively excluded at the time of transplant assessment in our unit.16 Our patients with refractory ascites had a slightly lower baseline MELD score than the French patients and a slightly higher baseline serum sodium, perhaps indicating less advanced circulatory dysfunction.32 Nevertheless, it should be noted that our refractory patients with ascites had a similar estimated 1-year transplant-free survival of 40%.
The issues that have been raised regarding the methodology of the Serste study are relevant in interpreting our data.17–20 In their paper, the NSBB patients appeared to be sicker at baseline than the non-NSBB patients, with a higher serum bilirubin and a tendency towards a higher Child-Pugh score.14 The non-NSBB group also had a greater proportion of patients with alcoholic liver disease, and no information was given regarding the prevalence of acute alcoholic hepatitis or abstinence from alcohol.20 The reported deleterious effect of NSBB could, therefore, have reflected more severe underlying end-stage liver disease at baseline in the NSBB patients.17–20 In our study, NSBB and non-NSBB patients were well matched with regards to cirrhosis aetiology, markers of hepatic synthetic function and MELD score. Acute alcoholic hepatitis is not currently an indication for transplantation in the UK, and abstinence from alcohol is mandatory for all patients listed for alcoholic cirrhosis. Furthermore, in a PRS-matched analysis, which is an accepted method of minimising selection bias in non-randomised studies, the observed benefit of NSBB was confirmed.19 ,28 ,29
It is notable that patients on NSBB had superior waitlist survival despite the accompanying lower systolic blood pressure. Reduced systemic blood pressure has been linked with prognosis in patients with cirrhosis and ascites, and is attributed to a relatively low cardiac output state failing to maintain the effective circulating volume.33 In the window hypothesis, Krag et al32 ,33 recommend that NSBB are avoided in patients with refractory ascites because this represents the threshold when β-blockade further impairs cardiac function. The lower systolic blood pressure we observed is consistent with a systemic haemodynamic response to NSBB, but the superior waitlist survival of the NSBB group goes against the postulation that the haemodynamic effects of β-blockade are detrimental in all patients with refractory ascites.32 We suggest that the therapeutic ‘window’ remains in such patients, and alternative markers of circulatory failure such as hypotension and reduced glomerular filtration rate may be more appropriate.
Our study has several limitations that should be mentioned. First, selection bias is inherent in any non-randomised observational study. Factors such as the clinical condition of the patient may have impacted on the use or non-use of NSBB and, hence, the association with waitlist mortality. Our unit is a tertiary referral centre, and, in most cases, the patients who were on an NSBB were already on the NSBB at the time of referral. Prescription is clinician dependent, varying within the catchment area, and being rarely altered by the transplant hepatologists. Furthermore, PRS matching was used, which is an accepted method of minimising selection bias in non-randomised studies.19 ,28 ,29 Second, the analysis relied on the assumption that all patients prescribed NSBB were compliant with their medications. Non-adherence is reported in patients on the liver transplant waiting list, although one perhaps might expect better compliance than in non-listed cirrhotic patients.34 Third, our NSBB patients were on a relatively low dose of NSBB when compared with the Serste study, which may be relevant when interpreting the results. Blood pressure data were only available for a subgroup of patients. However, it is well recognised that dose does not necessarily correlate with haemodynamic response and in a separate analysis (data not shown) we did not find an association between higher-dose NSBB and greater mortality.35 Finally, the documented causes of death are relatively superficial. Most deaths occurred in other hospitals, and the available information did not allow more detailed analysis. The impact of NSBB on specific causes of death, such as sepsis and hepatorenal syndrome, remains to be defined.
The findings of our study have important implications for patient management. NSBB are not associated with increased waitlist mortality in patients with ascites and refractory ascites listed for liver transplantation. Therefore, we recommend these patients should continue on NSBB in this setting unless they demonstrate intolerance or alternative markers of circulatory failure such as hypotension and reduced glomerular filtration rate. Given the select population studied, extrapolation of the results to non-listed patients with ascites should be done with caution. Even so, they are encouraging and justify prospective investigation in this setting.
In conclusion, in this large single-centre study, we have shown that NSBB in patients with ascites and refractory ascites listed for liver transplantation are not detrimental, and instead are associated with reduced transplant-free mortality and waitlist death. These findings argue that NSBB are safe and may confer benefit in patients with ascites complicating end-stage liver disease.
Acknowledgments
The study was supported by the National Institute for Health Research (NIHR) Liver Biomedical Research Unit based at Queen Elizabeth Hospital Birmingham and the University of Birmingham. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
JAL and NR contributed equally.
Contributors JAL and NR have substantially contributed to conception and design of this work, acquisition and analysis of data, the interpretation of data and the drafting/revising of the manuscript for important intellectual content. DT and JWF have substantially contributed to conception and design of this work, the interpretation of data for this work and the drafting/revising of the manuscript for important intellectual content. NT and BKG have substantially contributed to the acquisition of data for this work and the drafting/revising of the manuscript for important intellectual content. JH provided statistical input. All authors have approved the final version and agree to be accountable for all aspects of the work. JAL is the guarantor of this paper.
Funding None.
Competing interests None.
Patient consent None.
Ethics approval Clinical Audit Department at the Queen Elizabeth Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.