Article Text

Abstract
Background: Gas pooling within the gut may produce abdominal symptoms but the segment of the intestine responsible for gas retention is unknown. Our aim was to determine the role of the proximal and distal bowel in symptomatic gas accumulation using an experimental model of gas retention triggered by intraluminal lipids.
Subjects: Sixteen healthy subjects.
Methods: A gas mixture (N2, O2, and CO2 in venous proportions) was infused into the intestine at12 ml/min for three hours and gas evacuation was continuously measured via an anal cannula connected to a barostat. Abdominal perception and girth changes were measured at 10 minute intervals. Lipids (1 kcal/min) were simultaneously perfused either into the duodenum (n = 8) or into the ileum (n = 8). Each subject was studied twice on separate days, with gas infused into the jejunum or ileum.
Results: Duodenal lipids produced retention of gas infused into the jejunum (646 (62) ml) but the volume retained was much smaller when gas was infused directly into the ileum (262 (90) ml; p<0.05). The effects on gas retention were even more pronounced during ileal perfusion of lipids (1546 (184) ml during jejunal gas infusion and 847 (142) ml during ileal gas infusion; p<0.05). Abdominal distension correlated with the volume of gas retained (r = 0.87; p<0.001). Healthy subjects tolerated gas retention, and significant symptoms (score 3.7 (0.8)) developed only during jejunal gas infusion plus ileal lipid perfusion when gas retention was very large.
Conclusion: Intraluminal lipids induce intestinal gas retention, predominantly acting on the proximal small bowel.
- intestinal gas
- intestinal transit
- gut reflexes
- gut sensitivity
- abdominal distension
- bloating
- gastric distension
- lipids
- SF6, sulphur hexafluoride
Statistics from Altmetric.com
- intestinal gas
- intestinal transit
- gut reflexes
- gut sensitivity
- abdominal distension
- bloating
- gastric distension
- lipids
In healthy subjects the gut effectively regulates gas transit, adapting gas propulsion and evacuation rates to a wide range of intraluminal gas loads.1 This process is balanced by stimulatory and inhibitory reflex mechanisms: focal distension accelerates whereas intraluminal lipids delay gas transit.2,3 Using a gas challenge test we have further shown that patients with irritable bowel syndrome and functional bloating have impaired transit of gas and develop retention, abdominal distension, and discomfort in response to gas loads that are well tolerated by healthy subjects.4 Such dysfunction appears to be related to abnormal reflex control of gut motility because in these patients the lipid induced reflex is upregulated and produces an exaggerated delay in gas transit.3
Despite its pivotal importance for therapeutic targeting, the region of the gut most prone to symptomatic gas retention (that is, gas retention associated with abdominal distension and discomfort) has not been identified. We hypothesised that the colon, a wide gas producing organ,5 can accommodate and displace large masses of gas whereas the small intestine, longer and with a smaller lumen, is markedly less compliant and tolerant to gas loads. Thus our specific aim was to determine the putative role of the small intestine in gas retention and conscious perception. To this end we used a model of lipid induced gas retention in healthy subjects to compare the effects of jejunal versus ileal gas infusion. We have previously shown that duodenal lipids delay gas transit,3,6 but the effects were relatively small. As lipids seem to induce much more potent effects on gut motility when infused into the ileum (that is, the ileal brake),7–9 we performed separate experiments involving duodenal and ileal lipid perfusion.
MATERIAL AND METHODS
Participants
Sixteen healthy individuals (seven women and nine men; age range 21–35 years) participated in the study after giving written informed consent. Subjects completed a pre-entry questionnaire to verify the absence of gastrointestinal symptoms, particularly symptoms of constipation,10 difficult gas evacuation, feeling of excessive abdominal gas, or excessive gas evacuation. The protocol for the study had been approved previously by the institutional review board of the University Hospital Vall d’Hebron.
Intestinal tube assembly
Four types of tubes were used featuring different positions for the gas and lipid infusion sites in the following combinations. Duodenal lipids were perfused 15 cm orad and ileal lipids 100 cm caudad to the angle of Treitz. In each instance, jejunal gas was infused 5 cm caudad and ileal gas 115 cm caudad to the angle of Treitz. We used polyvinyl tube assemblies (3.2 mm OD) that incorporated a gas infusion channel (1.6 mm ID), lipid perfusion channel (1.2 mm ID), and a latex balloon on the tip, which was inflated (via a 0.8 mm ID channel) during the intubation procedure after passing the pylorus to speed intestinal passage. When the tube was in position the balloon was deflated.
Gas transit test
Intestinal gas infusion
Gas was continuously infused at 12 ml/min using a modified volumetric pump (Asid Bonz PP 50–300; Lubratronics, Unterschleissheim, Germany). We infused a gas mixture containing 88% nitrogen, 6.5% carbon dioxide, and 5.5% oxygen bubbled into water for saturation, mimicking the partial pressures of venous blood gases to minimise diffusion across the intestinal-blood barrier.11 To validate the absence of leakage in anal gas collection, a 6 ml bolus of sulphur hexafluoride (SF6), as a non-absorbable stable gaseous marker,12 was administered in the gas mixture over a 10 minute period 60 minutes after starting the infusion.
Measurement of anal gas evacuation
Intestinal gas evacuation was collected via an anal cannula which fits hermetically between the buttocks.1 The anal cannula was connected via a leak proof collection line to a barostat,13 and the volume of gas evacuated was continuously recorded on a paper polygraph (model 6006; Letica, Barcelona, Spain), as previously described.1 Subjects were provided with an event marker to signal every gas expulsion for later correlation with the recorded gas evacuation. A sample of gas evacuated (flatus) during each 30 minute period was stored in metallic bags (gas collection 750 ml; QuinTron, Milwaukee, Wisconsin, USA) for later analysis of SF6 concentration by infrared absorbance after determination of standard curves.14
Measurement of abdominal girth changes
Once subjects were in bed (see “procedure” below), a non-stretch 48 mm wide belt with a metric tape measure was adjusted around the abdomen over the umbilicus by means of two elastic bands. Girth measurements were taken at 10 minutes intervals while subjects were breathing in a relaxed manner as the average of inspiratory and expiratory determinations over three consecutive respiratory excursions.
Intestinal lipid perfusion
Experiments were performed during continuous perfusion of a lipid emulsion (Intralipid 20%; Pharmacia and Upjohn, St Cugat del Vallés, Spain) diluted in 0.9% saline (296 mosmol/l) and infused into either the duodenum or ileum at 2 ml/min (1 kcal/min) using a volumetric pump (Asid Bonz PP 50-300; Lubratronics).
Perception measurements
Subjective perception was measured at 10 minute intervals using a graded questionnaire to measure the intensity and type of sensations perceived, and an anatomical questionnaire to measure the location and extension of the perceived sensations.1,15 The graded questionnaire included four graphic rating scales specifically for scoring four possible abdominal sensations: (a) pressure/bloating, (b) cramp/colicky sensation, (c) stinging sensation, and (d) other type of sensation (to be specified), respectively. Each sensation was independently scored on the respective rating scale from 0 (no perception) to 6 (painful sensation). Participants were asked to score any abdominal sensation (one or more perceived simultaneously) on the scales but only the highest score, instead of the mean or cumulative score, was computed for comparisons. The questionnaire included two additional tick boxes (yes/no) to signal belching and difficult gas evacuation. The anatomical questionnaire incorporated a diagram of the abdomen divided into nine regions corresponding to the epigastrium, periumbilical area, hypogastrium, both hypochondria, flanks, and iliac fossae. Participants were instructed to mark the location—that is, abdominal region (s)—where the sensations were perceived.
Procedure
Participants were instructed to follow a diet excluding legumes, vegetables, garlic, onions, nuts, cereals, wholemeal bread, and fizzy drinks during the two days prior to the study. The night before the study they had a light dinner that consisted of meat, fish, eggs, rice, pasta, and/or white bread but avoiding in particular dairy products, salad, fruit, and alcoholic beverages. On the day of the study, participants were orally intubated after an eight hour fast. The intestinal tube assembly was positioned in the desired location (see “experimental design”) under fluoroscopic control. Studies were conducted in a quiet isolated room with subjects placed supine in bed at an angle of 30° to the horizontal. After a 30 minute basal period with lipid perfusion, gas infusion was started and both were maintained for the three hour test period. During the studies, abdominal perception and girth changes were measured at 10 minute intervals.
Experimental design
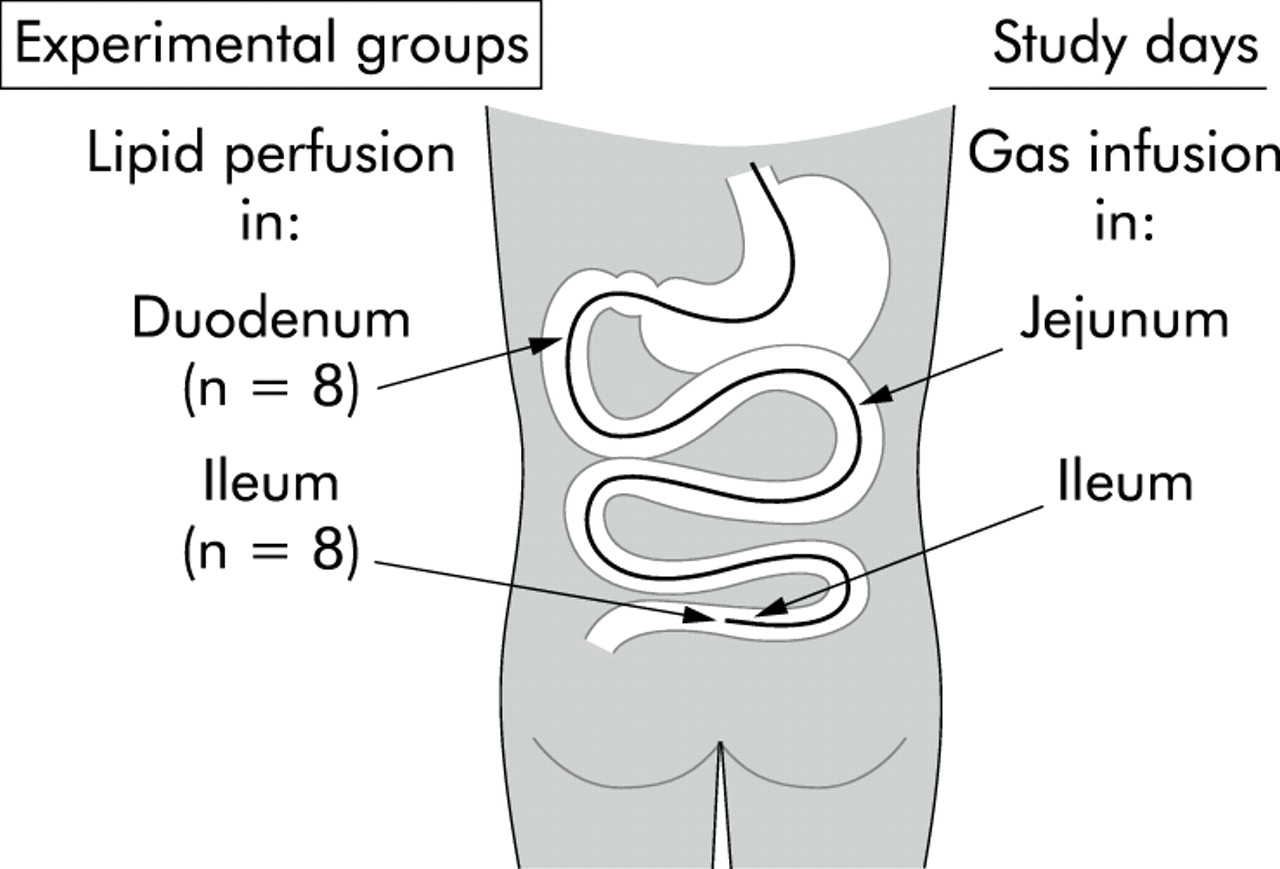
In one group of subjects (n = 8), studies were performed with duodenal lipid perfusion and in the other group (n = 8) with ileal lipid perfusion. In each of the 16 individuals the effect of jejunal and ileal gas infusion was tested on separate days, at one week intervals, and in random order (fig 1).
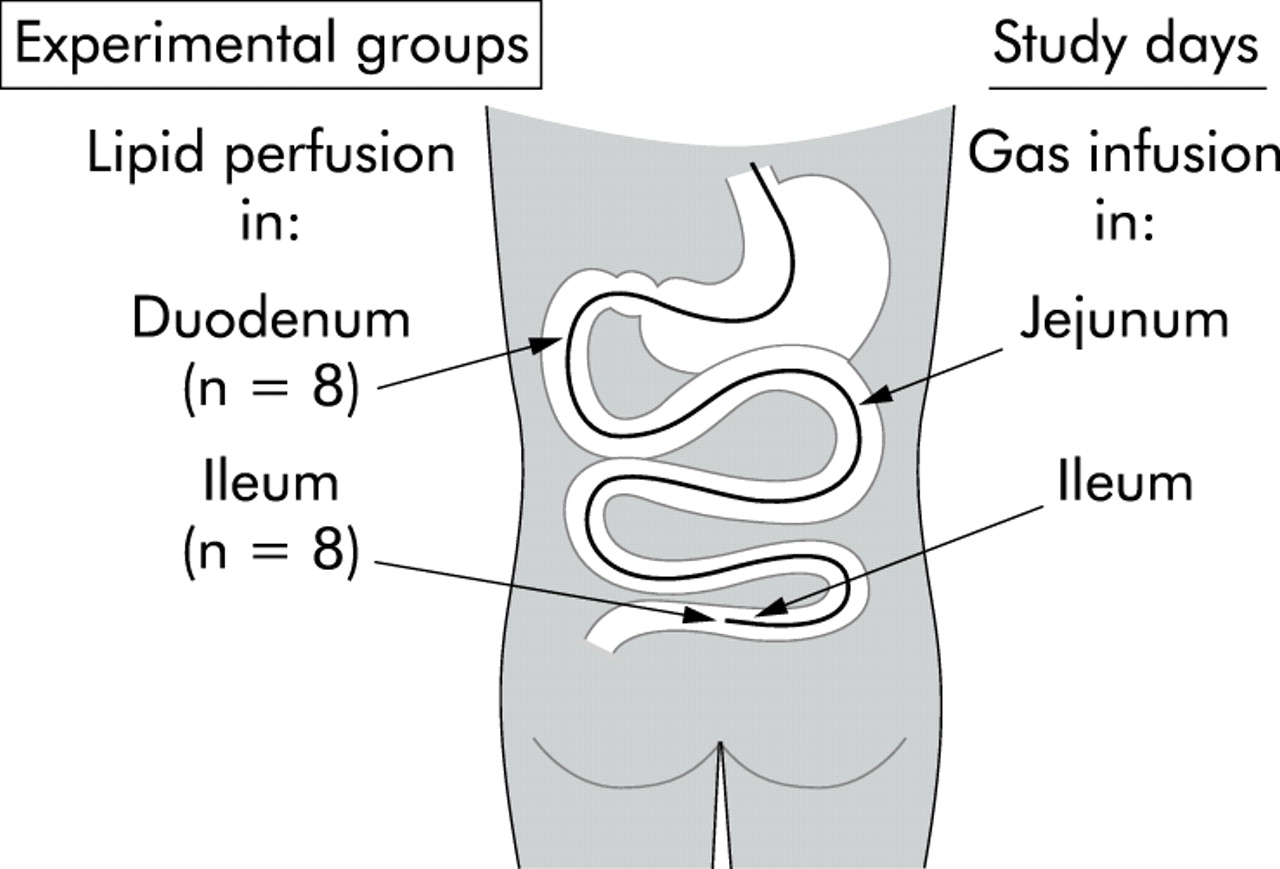
Experimental design. In two groups of healthy subjects, we studied the effect of lipid perfusion in the duodenum (n = 8) and ileum (n = 8), respectively. In each individual the effect of gas infusion in the jejunum and ileum was tested in random order on separate days at one week intervals.
Outcome measures
In each subject, we calculated the volume of gas retained within the gut as the difference between the volume of gas infused and the volume of gas recovered. Reliability of this method of calculation has been validated previously in detail.1
Perception of abdominal sensations experienced by participants during the studies was measured by the score rated on the scales. In each subject we also counted the number of times each abdominal sensation was scored to calculate the frequency (as per cent distribution) of each specific sensation. Perception of rectal gas retention and belching were analysed separately.
Changes in abdominal girth during the study were referenced to girth measurements at the start of the study.
Statistical analysis
In each subject, we averaged over 30 minute periods the parameters (gas retention, abdominal perception, and girth changes) that were measured at 10 minute intervals. Unless otherwise indicated, the effects of the various stimuli tested in each subject were compared using the average of the values measured during the last 30 minutes of the test period. In each group of subjects we calculated the mean (SEM) or grand mean (SEM) values, as appropriate, of the parameters measured. The Komolgorov-Smirnov test was used to check the normality of the data distribution. Comparisons of parametric normally distributed data were performed using the Student’s t test, paired tests for intragroup comparisons, and unpaired tests for intergroup comparisons; otherwise the Wilcoxon signed rank test was used for paired data and the Mann-Whitney U test for unpaired data. Correlations between paired data were examined by linear regression analysis.
RESULTS
Anal gas collection was uneventful, and in all experiments signalled gas expulsions correlated with recorded evacuations (r = 0.99; p<0.001). No subject reported belching or sensations of difficult gas evacuation.
Duodenal lipid perfusion
Gas evacuation
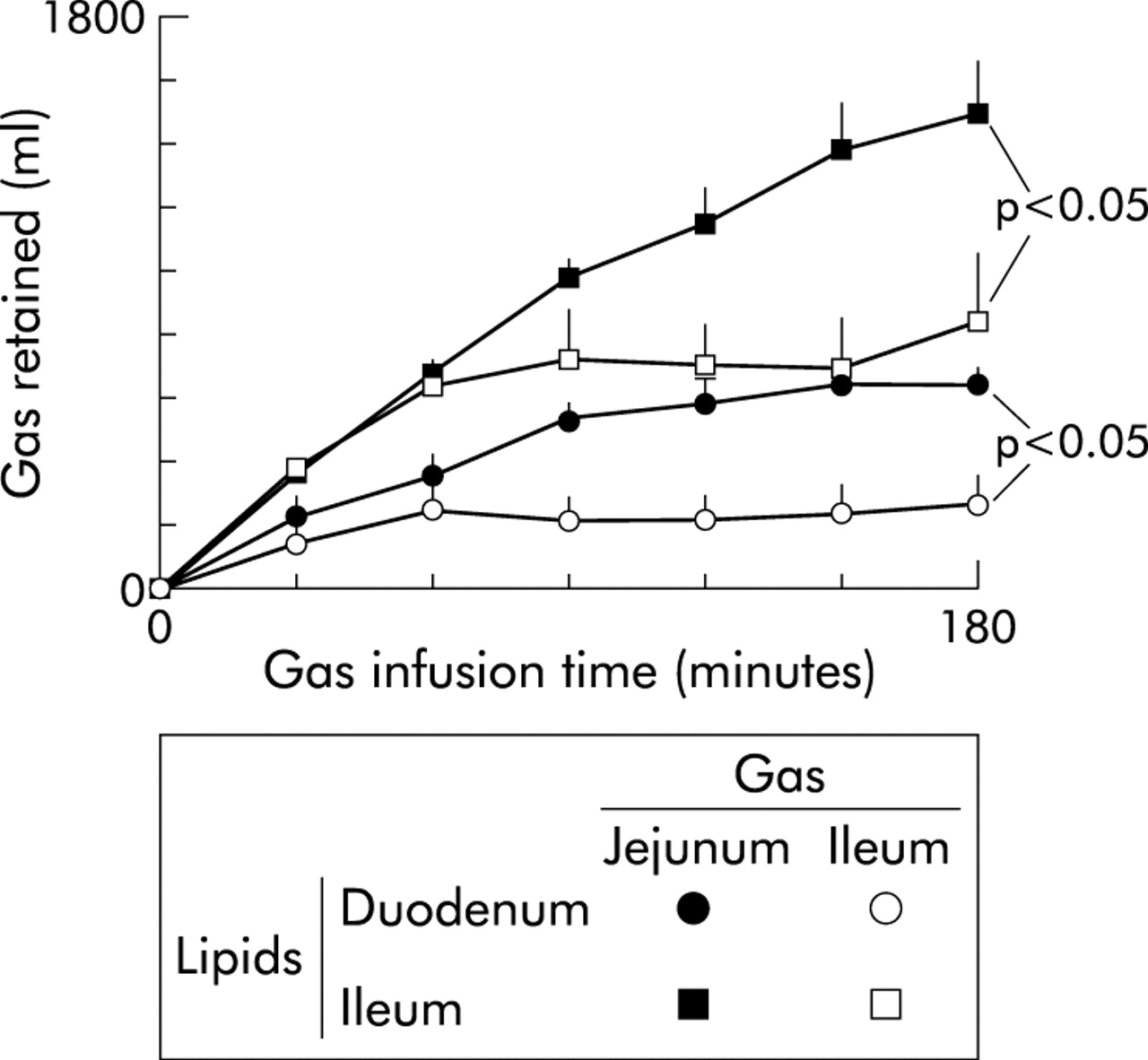
During the first 30 minutes with duodenal lipid perfusion prior to intestinal gas infusion (baseline period), endogenous gas evacuation was very small and similar on both study days (38 (24) ml/30 minutes; pooled data). Gas infusion into the jejunum resulted in significant gas retention (p<0.05) that remained steady from 90 minutes until the end of the study (fig 2). In contrast, when gas was infused in the same subjects into the ileum, gas evacuation was faster from the beginning of the test period (185 (64) ml expelled during the first 30 minutes of gas infusion v 123 (52) ml during jejunal gas infusion; p<0.05). After 60 minutes of infusion, the volume of gas retained became steady until the end of the study. Both average volume retention over the three hour test period (672 (33) ml v 885 (83) ml during jejunal gas infusion; p<0.05) as well as the volume retained by the end of the study (fig 2) were significantly smaller during ileal compared with jejunal gas infusion. Conversely, the total volume of gas evacuated by the end of the test period was greater during ileal compared with jejunal gas infusion (1811 (122) ml v 1513 (52) ml, respectively; p<0.05). The faster evacuation of gas infused into the ileum was also evidenced by SF6 outflow: 10% of the SF6 bolus administered during steady state conditions (60 minutes after starting gas infusion) was evacuated in 51 (6) minutes during ileal versus 68 (7) minutes during jejunal gas infusion (p<0.05).

Retention of intestinal gas loads. Gas retention (infused minus evacuated) was significantly larger when gas was infused into the jejunum compared with the ileum. Conversely, the effect of lipids on gas retention was more potent with ileal than with jejunal lipid perfusion.
Perception and abdominal distension
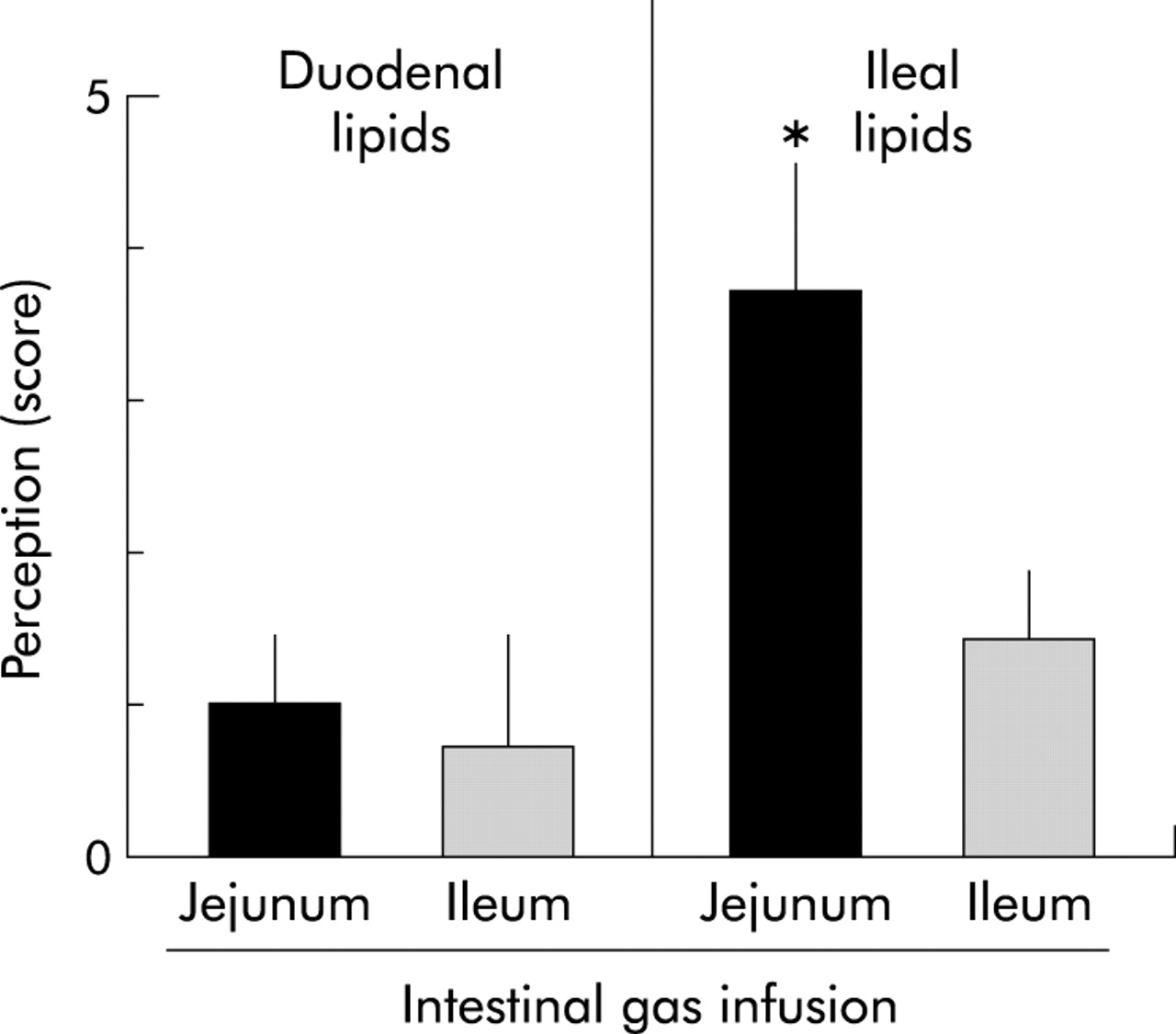
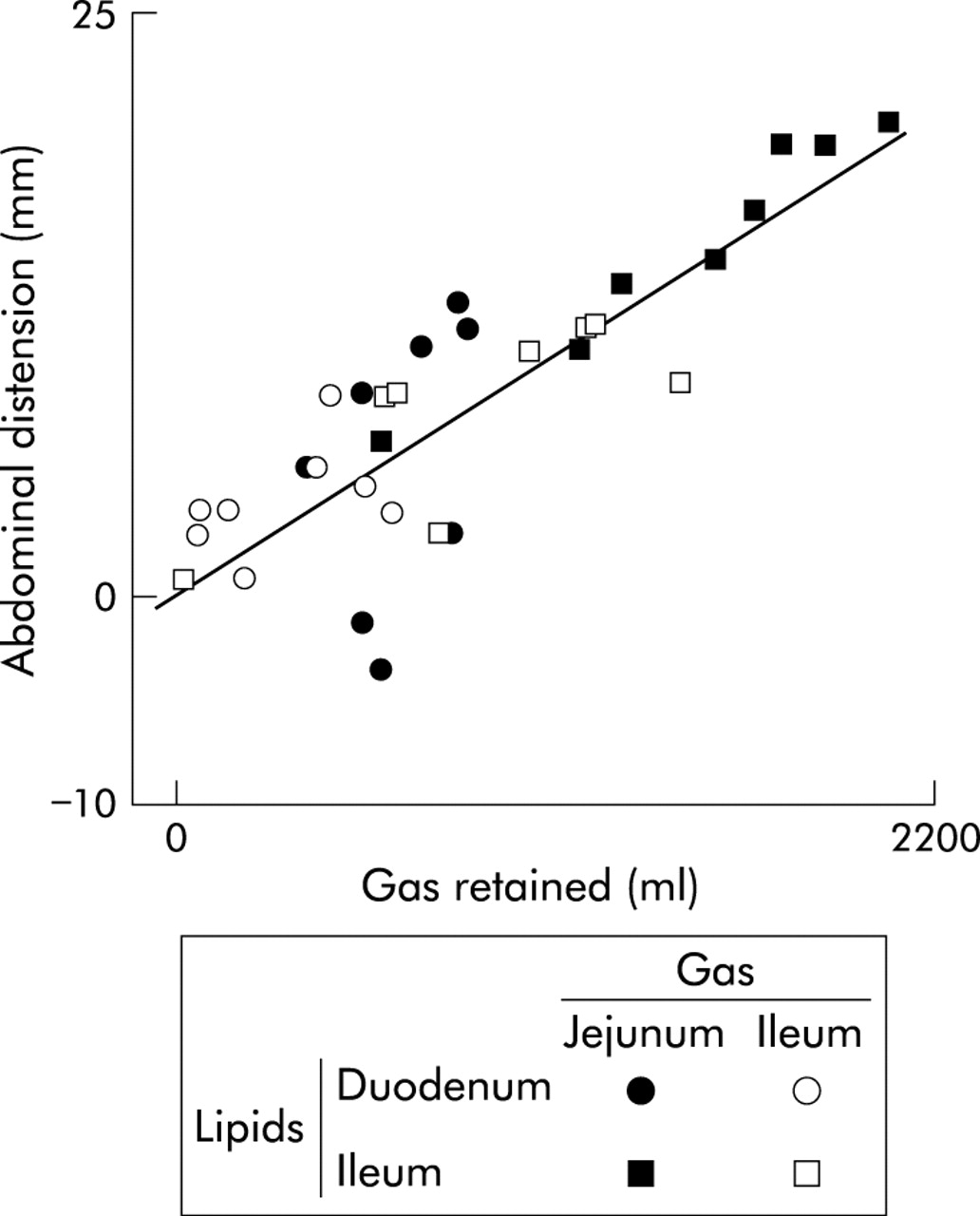
Intestinal gas infusion in the jejunum and ileum was well tolerated, and despite differences in gas retention, perception remained low and at a similar level in both instances (fig 3). Abdominal distension correlated with the volume of gas retention (fig 4). Distension was somewhat larger during jejunal than during ileal gas infusion but this differences was not statistically significant (6 (2) mm v 3 (1) mm girth increment by the end of the study, respectively; NS)

Perception of intestinal gas loads. Data are mean (SEM) during the last 30 minutes of the test period. Significant symptoms were only reported during jejunal gas infusion plus ileal lipids, when gas retention was greater.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abdominal distension induced by intestinal gas loads. Overall, girth increments correlated with the amount of gas retained within the gut.
Ileal lipid perfusion
Gas evacuation
During the first 30 minutes with ileal lipid perfusion prior to intestinal gas infusion (baseline period), endogenous gas evacuation was completely inhibited by ileal lipids, and no gas was expelled on either study day (p<0.05 v duodenal lipids). This early effect of ileal lipids was sustained during the first hour of gas infusion: both during jejunal and ileal lipid infusion, gas evacuation during the first hour was virtually nil (p<0.05 v duodenal lipids for both), and the gas infused was retained within the gut (fig 2). Thereafter, gas evacuation started. During jejunal gas infusion, gas evacuation never matched the infusion rate, and progressive gas retention developed during the study (p<0.05 v duodenal lipids) (fig 2). In contrast, after 60 minutes of ileal gas infusion, gas evacuation matched the infusion rate, and gas retention remained steady until the end of the study (fig 2) at a lower level than during jejunal gas infusion (p<0.05). The number of gas evacuations during jejunal gas infusion (7 (1) evacuations/hour) was lower than during ileal gas infusion (11 (1) evacuations/hour; p<0.05). The volume of gas retained and number of evacuations in the experiments with ileal lipids were significantly greater than in experiments with duodenal perfusion of lipids, both during jejunal and ileal gas infusion (p<0.05 for both). However, the volume of gas expelled per evacuation was similar under all four experimental conditions (49 (5) ml jejunal v 43 (5) ml ileal gas (NS); NS v duodenal lipids). The effect of ileal lipids on gas transit was also reflected in recovery of the gaseous marker. Thus 10% of SF6 administered 60 minutes after starting the gas infusion was evacuated earlier during ileal than during jejunal gas infusion (73 (10) minutes v 109 (8) minutes, respectively; p<0.05) but significantly later than in experiments with duodenal lipid perfusion (p<0.05 for both).
Perception and abdominal distension
During jejunal gas infusion, the massive gas retention induced by ileal lipids caused significant perception of abdominal symptoms (fig 3). In contrast, smaller retention during ileal gas infusion was associated with smaller perception (p<0.05), similar to that with duodenal lipids (fig 3). Symptoms referred to by subjects in experiments with ileal lipids and jejunal gas infusion were pressure/bloating (47 (11)%) and cramp/colicky sensation (38 (9)%), and were predominantly referred to the abdominal midline (76 (13)% of the time). Abdominal distension correlated with gas retention (fig 4) and accordingly, girth increment was significantly greater during jejunal than during ileal gas infusion (15 (2) and 8 (1) mm by the end of the study, respectively; p<0.01), and both were greater than with duodenal lipid perfusion (p<0.05 for both).
DISCUSSION
We have shown that the small intestine, despite its smaller capacity relative to the colon, may play a major role in the development of gas retention, abdominal symptoms, and objective abdominal distension.
Our studies were performed using a model of gas retention induced by intestinal lipid infusion.3,6 In this model we showed significant differences in gas transit and retention when gas was infused into the jejunum compared with the ileum, which indicates the small intestine as a major site of gas pooling. We previously found that gas retention induced by duodenal lipids was well tolerated without symptoms.3,6 To study the role of the small intestine on gas related symptoms, we took advantage of the potent effects of ileal lipids (that is, the ileal brake),7,8 and hence we also tested the effect of direct lipid perfusion into the ileum. Indeed, ileal lipids delayed gas transit to a greater extent that duodenal lipids. With ileal lipids, a large proportion of the gas infused into the jejunum was retained within the gut and caused abdominal symptoms, but when gas was infused into the ileum, gas retention was markedly smaller and less perceived. Hence it seems that in healthy subjects, gas pooling requires a certain threshold to trigger symptomatic perception. In contrast with this discontinuous threshold dependent perception, abdominal distension exhibited a continuous linear correlation with the volume of gas retention and seemed unrelated to the site of either gas or lipid infusion.
Our results suggest that the small intestine may be the origin of gas symptoms. However, alternative interpretations should be examined. For instance, the gas stimulus in the proximal, but not the distal, intestine could induce colonic delay of transit via an inhibitory enterocolic reflex, and this reflex could be sensitised by intraluminal lipids, particularly when lipids are administered into the ileum. However, we have previously shown that small bowel distension accelerates the transit of gas through the gut and almost completely antagonises the delaying effect of lipids.2 In the latter experiments focal balloon distension was tested but these data render the putative inhibition of transit via a gas induced enterocolic reflex unlikely.
Other studies from our laboratory support a predominant role of the small intestine in symptomatic gas retention. Using a model of intestinal gas retention by blocked gas outflow, we recently showed that symptoms depend on the territory of gas pooling: gas infused into the jejunum produces abdominal symptoms whereas the same gas load delivered via the rectum does not.16 Furthermore, scintigraphic scanning of radiolabelled gas in these studies demonstrated that gas infused into the jejunum largely pools within the small intestine and proximal colon whereas gas infused via the rectum remains in the rectosigmoid region without reaching the proximal colon.
Perception of intraluminal gas depends also on the mechanisms of retention. Gas retention may result either from reduced propulsion or from increased resistance to flow. Reduced propulsion induced by pharmacological inhibition of gut motility produces intestinal gas retention associated with abdominal distension but without abdominal discomfort. In contrast, a similar amount of gas retained by increased resistance to flow, modelled by self restraint anal gas evacuation, induces significant abdominal discomfort.17 The effect of lipid infusion on gut motility may vary depending on the level of the gut investigated.7,18–21 In the context of our experiments, gas retention was related to a relaxatory effect because large volumes of gas retained during either jejunal gas plus duodenal lipids or during ileal gas plus ileal lipids were well tolerated; only extreme gas retention during jejunal gas plus ileal lipids activated intestinal mechanoreceptors and induced symptoms.22 In a previous study using the model of retention by blocked gas outflow,16 perception was higher (score 4.4 (0.4) at 720 ml) than in the present studies using the lipid induced retention model.
The “ileal brake” has been shown to control transit of chyme. This effect is associated with endogenous release of peptide YY9 and is abolished by naloxone23 and 5-hydroxytryptamine-3 receptor antagonists.24 Subsequent studies have confirmed that the ileal brake is mediated by peptide YY,25 opioid efferent pathways,26 and 5-hydroxytryptamine-3 receptors, possibly located on myenteric neurones.27These types of reflexes have been shown to depend on the type of nutrient exposure: lipids are particularly effective in delaying the transit of chyme8 and this nutrient specificity seems to apply to modulation of gas propulsion also.28 The site of action of lipids in reference to gas propulsion remains uncertain. The terminal ileum and ileocolonic sphincter have a specific function in regulating passage of chyme into the colon but a selective action at this level seems unlikely as transit of jejunal and ileal gas loads would have been equally affected. Alternatively, lipids could act at the jejunal level but more likely lipids may exert a general effect all along the small bowel, and the predominant effect on jejunal gas observed would depend only on the length of the caudal segment exerting resistance to gas progression. Indeed, a distal effect of ileal lipids seems undeniable because in contrast with duodenal lipids, they significantly delayed transit of gas infused into the ileum. Further support for distal retention is provided by the fact that ileal lipids inhibited spontaneous evacuation of endogenous gas during the baseline period, prior to experimental gas infusion.
Our study considered very specific non-physiological conditions (that is, intestinal lipid perfusion) but nevertheless, our results could have important pathophysiological implications. Patients with unexplained abdominal bloating, such as those with irritable bowel syndrome or functional bloating,10 frequently attribute their symptoms to intestinal gas and indeed, they have both impaired gas propulsion and heightened perception. We have recently shown that this dysfunction is severely aggravated by intraluminal lipids.3 Hence patients with such functional disorders manifest a hypersensitivity to intestinal lipids that induces disproportionate effects on gas retention and marked intolerance. Interpretation of abnormalities in gas tolerance and transit in these patients is at this moment purely speculative but our data challenge the old pathophysiological hypothesis—namely, that patients with irritable bowel syndrome have an excess amount of nutrients in the potent trigger zone of the distal small bowel, suffer from a hypersensitive ileum, or a combination of both.
Acknowledgments
Supported in part by the Spanish Ministry of Education (Dirección General de Enseñanza Superior del Ministerio de Educación y Cultura, BFI 2002-03413), Instituto de salud Carlos III (grants 02/3036 and C03/02), and by the National Institutes of Health, USA (grant DK 57064). Dr Hernando-Harder was supported by a scholarship from the Argentinian Society of Gastroenterology and Dr Serra by a scholarship from the Spanish Ministry of Health (ISCIII 02/3036). The authors thank Nuria Ferrer and Isidre Casals, Serveis Cientifico-Tecnics of the Central University of Barcelona, for help in gas infrared absorbance analysis; Maite Casaus and Anna Aparici for technical support; and Gloria Santaliestra for secretarial assistance.
REFERENCES
Footnotes
-
↵* Present address: Department of Medicine II, University Hospital, Theodor-Kutzer-Ufer, 68135 Mannheim, Germany