Article Text

Abstract
The prevalence of Helicobacter pylori infection is very low in patients with fundic gland polyps (FGPs) of the stomach. We report here two cases with multiple FGPs that regressed following new H pylori acquisition. Patient Nos I and II had multiple FGPs in normal fundic mucosa without inflammatory changes or atrophy. Both were not infected with H pylori. Following acquisition of H pylori infection however, all FGPs in both patients completely disappeared except for one FGP in patient No I. Although the size of the remaining polyp in patient No I was greatly reduced after H pylori acquisition, it became enlarged again after eradication. Interestingly, in the remaining polyp, we found an activating β-catenin gene mutation whereas no such mutations were detected in FGPs of patient No II. Thus H pylori infection may have an inhibitory effect on the development of FGPs.
- stomach
- corpus
- chronic gastritis
- infection
- hyperplasia
- oxyntic cells
- FGP, fundic gland polyps
- FAP, familial adenomatous polyposis
- GSK-3β, glycogen synthase kinase 3β
Statistics from Altmetric.com
Hyperplastic gastric polyps, which are characterised by hyperplasia of the foveolar epithelium, often develop in Helicobacter pylori infected gastric mucosa.1 In contrast, fundic gland polyps (FGPs), which are composed of fundic glands with disordered architecture and microcysts, frequently develop in the normal fundic mucosa.2,3 Interestingly, the prevalence of H pylori infection in patients with FGPs is extremely low.4,5 Thus H pylori infection does not appear to be involved in the development of FGPs. FGPs have generally been regarded as non-neoplastic lesions, either hamartomatous or hyperplastic in nature.6 However, recent studies have demonstrated somatic alterations of two genes in FGPs.7,8 Firstly, FGPs occurred in patients with familial adenomatous polyposis (FAP) containing second hit alterations in the adenomatous polyposis coli gene. Secondly, sporadic FGPs have somatic activating mutations of the β-catenin gene. Here we report two cases of multiple FGPs of a sporadic form that regressed following H pylori acquisition. Notably, we found that a somatic mutation of the β-catenin gene in one FGP in one patient, the size of which was markedly reduced after H pylori acquisition, was enlarged following eradication of H pylori.
CASE REPORTS
Patient No I
A 71 year old man underwent gastrointestinal endoscopy in February 1999 because of abdominal discomfort. Endoscopy demonstrated 15 recognisable polyps in the gastric corpus (fig 1A). Biopsies revealed that the polyps consisted of fundic gland hyperplasia with microcysts, the typical morphology of FGPs (fig 1B). Neither active gastritis nor atrophic changes of the fundic glands was detected. Results of both the rapid urease test and immunohistological staining for H pylori were negative. Serum antibody to H pylori was also negative. A colonoscopic examination performed one month later showed entirely normal colon, ruling out FAP. However, follow up endoscopy one year later demonstrated disappearance of all FGPs except for one polyp, the size of which was markedly reduced, in association with diffuse erythematous fundic mucosa (fig 1C). Biopsies showed chronic inflammatory changes in the corpus and antrum. H pylori acquisition was confirmed by culture, rapid urease test, immunohistological staining, and elevated serum IgG to H pylori. In addition, the remaining polyp was characterised by oedematous changes and neutrophilic infiltration concentrated in the foveolar compartment. Moreover, the remaining polyp showed disappearance of cystic dilatation of glandular ducts with concomitant appearance of elongation of foveolar epithelium (fig 1D). H pylori eradication was performed with lansoprazole, amoxicilin, and clarithromycin.
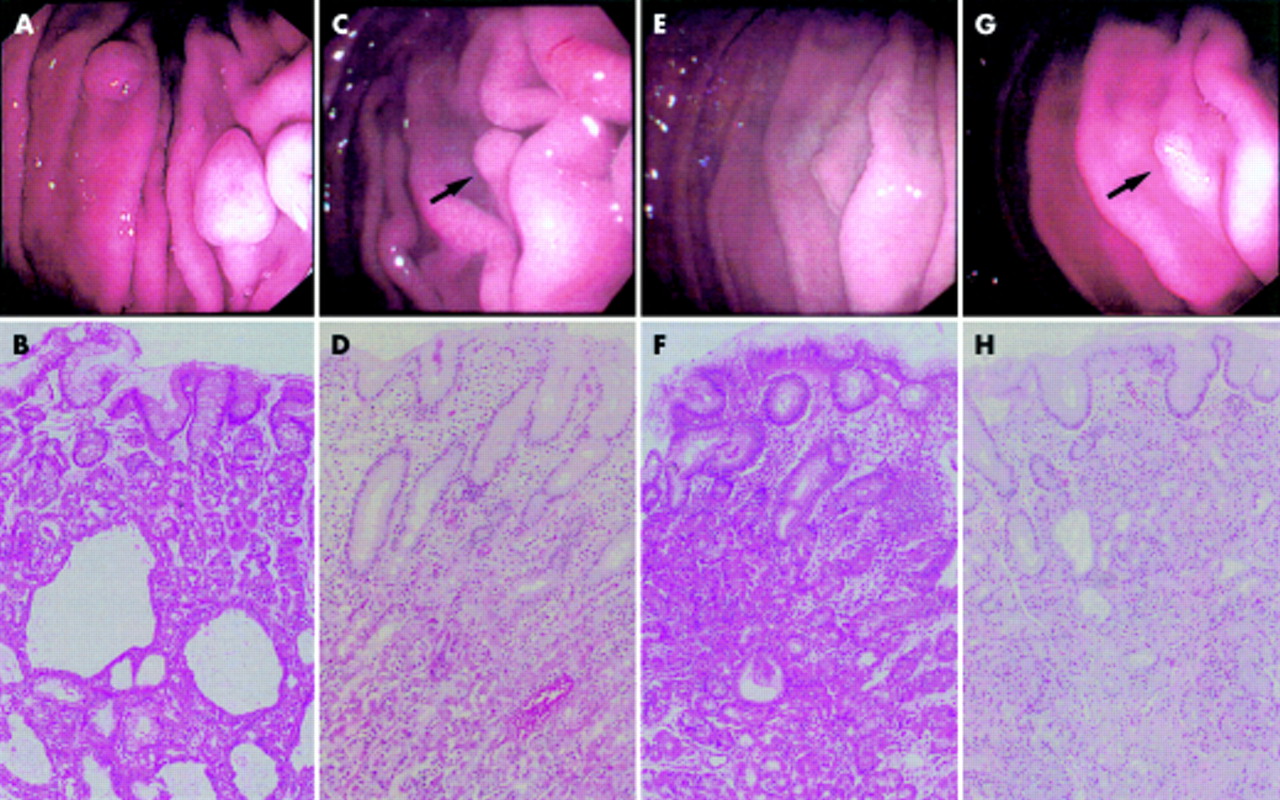
Endoscopic and microscopic findings in patient No I. Sessile polyps were seen in the normal gastric corpus in February 1999 (A). Biopsies revealed that the polyps consisted of fundic gland hyperplasia with cystic dilatation of glandular ducts—typical morphology of fundic gland polyps (FGPs) (B). Endoscopy one year later showed erythematous mucosa of the corpus and disappearance of FGPs except for one polyp (arrow), the size of which was markedly reduced (C). On histological examination, the remaining polyp showed oedematous changes and neutrophilic infiltration concentrated in the foveolar compartment whereas less inflammatory cells infiltrated the fundic gland compartment (D). Two months after completion of Helicobacter pylori eradication therapy, endoscopy showed reduction of erythematous mucosa and no recurrence of polyps (E). Biopsy demonstrated marked reduction of active inflammation in the remaining polyp (F). Six months after completion of eradication, endoscopy demonstrated enlargement of the remaining polyp (arrow) (G). Biopsy of the polyp revealed hyperplasia of the fundic glands with microcysts, suggesting FGP morphology (H). Endoscopic photographs (top) show the same view in the corpus. (Haematoxylin-eosin staining; original magnifications: lower panels 100×.)
Two months after completion of eradication therapy, follow up endoscopy showed no recurrence of polyps (fig 1E). Biopsy demonstrated marked reduction of active inflammation in the antral and corpus mucosa, including the remaining polyp (fig 1F). Biopsy and culture for H pylori and the urea breath test showed clearance of H pylori. Serum gastrin, pepsinogen I, and pepsinogen II levels were decreased. However, on follow up endoscopy six months after completion of eradication therapy, enlargement of the remaining polyp was noted (fig 1G). Polyp biopsies revealed hyperplasia of the fundic glands with microcysts (fig 1H), showing typical FGP morphology, and resolution of gastritis without atrophy was again confirmed. At 18 months after H pylori eradication, endoscopy again detected the remaining polyp, while no recurrence of other polyps. During his clinical course he has not received any specific medication except those for H pylori eradication.
Patient No II
A 42 year old woman underwent gastrointestinal endoscopy in July 1998 because of iron deficiency anaemia. She had been treated with oral administration of ferrous sulphate for two months. Endoscopy demonstrated 25 polyps in the corpus without any sign of gastritis (fig 2A). Biopsies revealed the polyps to consist of fundic gland hyperplasia with microcysts (fig 2B). Neither chronic inflammatory change nor atrophy was detected. Absence of H pylori was confirmed by the rapid urease test and immunohistological staining for H pylori. Serum antibody for H pylori was also negative. Two months later, colonoscopic examination showed entirely normal colon, ruling out FGPs associated with familial FAP. Endoscopic findings of the stomach one year later were unchanged. Two years after the first examination however, endoscopy demonstrated diffuse erythematous fundic mucosa with disappearance of all of the FGPs (fig 2C). Biopsies showed chronic inflammatory changes in the corpus and antrum (fig 2D), and H pylori acquisition was confirmed. H pylori eradication therapy was performed as described in patient No I. Two months after completion of eradication therapy, follow up endoscopy demonstrated no recurrence of FGPs (fig 2E) and biopsies revealed resolution of gastritis and hyperplastic change of the fundic glands (fig 2F). Clearance of H pylori was confirmed. Ten months after completion of eradication therapy, endoscopy revealed no recurrence of FGPs. During her clinical course after the first detection of FGPs, she has not received any specific medication except for H pylori eradication.

{kind=link}
{kind=link}
Endoscopic and microscopic findings in patient No II. Multiple sessile polyps were seen in the normal gastric corpus in July 1998 (A). Biopsies confirmed hyperplasia of the fundic gland with microcysts (B). Endoscopy two years later revealed diffuse erythematous mucosa with complete disappearance of all polyps (C). Biopsy specimens showed neutrophilic infiltration concentrated in the foveolar compartment (D). Two months after completion of Helicobacter pylori eradication, endoscopy demonstrated resolution of erythematous change of the fundic mucosa and no recurrence of polyps (E). On histological examination, gastritis was reduced and the fundic glands had hyperplastic changes (F). Endoscopic photographs (top) show the same view in the corpus. (Haematoxylin-eosin staining; original magnifications: lower panels 100×.)
Mutation analysis of the β-catenin gene
A recent report has revealed that sporadic FGPs possess β-catenin gene mutations at glycogen synthase kinase 3β (GSK-3β) phosphorylation sites.8 Therefore, we examined whether FGPs in our two patients had β-catenin gene mutations. Genomic DNA was extracted from formalin fixed paraffin embedded biopsy specimens of FGPs and non-polypoidal normal fundic mucosa, and a 200 bp fragment of exon 3 of the β-catenin gene encompassing GSK-3β phosphorylation sites was amplified by polymerase chain reaction and sequenced directly, as described previously,8 with slight modifications. In the FGP of patient No I, that remained even after H pylori acquisition, direct sequencing analysis showed 1 bp missense mutation (TCT→TTT, Ser→Phe) at codon 37, one of the serine/threonine residues at GSK-3β phosphorylation sites, both before and after H pylori acquisition. In contrast, other FGPs, which disappeared after H pylori infection, did not have such mutations in patient No I. Moreover, we could not detect β-catenin gene mutations from any FGP in patient No II, which completely regressed after H pylori acquisition. In both patients, no β-catenin gene mutation was detected in the non-polypoidal normal fundic mucosa.
DISCUSSION
In our two patients with FGPs, we found no colonisation of H pylori. Moreover, neither corpus gastritis nor atrophy was observed. On follow up endoscopy however, we found that they were newly infected with H pylori and developed chronic active gastritis in the corpus and antrum. Interestingly, the development of corpus gastritis by H pylori acquisition in these patients was associated with disappearance of FGPs except for one polyp in patient No I. These findings strongly suggest that FGPs were regressed by H pylori acquisition with the development of active corpus gastritis.
The precise mechanism for regression of FGPs by H pylori acquisition remains unknown at present. FGPs are usually defined as hyperplasia of the fundic glands as well as shortened foveolae.9 In contrast, H pylori infection induces development of fundic gland atrophy.2,10 At the same time, H pylori infection occasionally induces foveolar hyperplasia—for example, giant fold gastritis.11 As stem cells in the isthmus of the fundic mucosa can give rise to both foveolar mucous pit cell lineage and fundic glandular cell lineage,12 it may be interesting to speculate that acquired H pylori infection in our patients altered the direction of the differentiation process of the fundic gland progenitor cells in the FGPs from glandular cell lineage towards pit cell lineage. Our finding that, in addition to elimination of almost all FGPs after H pylori acquisition, the remaining polyp in patient No I showed disappearance of cystic dilatation of glandular ducts with concomitant appearance of elongation of foveolar epithelium, may support our hypothesis.
A recent study has reported that mutations of the β-catenin gene at GSK-3β phosphorylation sites frequently occur in sporadic FGPs.8 Mutations at these sites result in stable β-catenin forms leading to aberrant Wnt signalling, an important pathway of tumorigenesis.13 Thus activating β-catenin gene mutations may be responsible for generation and/or expansion of sporadic FGPs. In our patient No I, one FGP remained even after H pylori acquisition, although its size was reduced, but it was enlarged again after H pylori eradication. Interestingly, we found an activating β-catenin gene mutation in this FGP. In contrast, we could not find any mutations in the FGPs of patient Nos I and II that completely disappeared by H pylori acquisition and did not recur even after H pylori eradication. Thus it is interesting to speculate that although H pylori infection has an inhibitory effect on the growth of FGPs, FGPs with β-catenin gene mutations somehow possess resistance to the influence of H pylori infection.
The natural history of FGPs has not been clearly established. Some investigators have reported a decrease not only in size but also in the number of polyps during observation whereas others have documented an increase in size as well as number.14,15 Thus how H pylori infection and/or alterations in the β-catenin gene influence(s) the natural history of FGPs remains to be determined.
In summary, we have described multiple FGPs regression following H pylori acquisition with concomitant appearance of corpus gastritis in two patients, indicating an inhibitory action of H pylori infection on the development and expansion of FGPs. These findings are in agreement with the fact that the prevalence of H pylori infection is very low in patients with FGPs. As we investigated only two cases, a further study in a large number of patients with FGPs is required to clarify the roles of β-catenin gene mutation and H pylori infection in the clinical course of FGPs.