Article Text

Abstract
Background: Dietary fat has been suggested to determine the therapeutic effect of enteral diets in Crohn's disease.
Aim: To assess the efficacy of two whole protein based diets with different fat compositions (n6 polyunsaturated fatty acids v monounsaturated fatty acids) in inducing clinical remission in active Crohn's disease compared with steroids.
Methods: Sixty two patients with active Crohn's disease were randomised to receive, for not more than 4 weeks: (a) a polymeric enteral diet containing 35 g of lipids per 1000 kcal, high in oleate (79%) and low in linoleate (6.5%) (PEN1), (b) an identical enteral diet except for the type of fat which was high in linoleate (45%) and low in oleate (28%) (PEN2), or (c) oral prednisone (1 mg/kg/day). Diets were double blindly administered. The steroid group received a conventional ward diet. Treatment failure was considered when remission was not achieved at week 4. Clinical activity and biological and nutritional parameters were monitored. Independent predictors of remission were identified by stepwise logistic regression analysis.
Results: Overall remission rates (by intention to treat) were 20% (4/20) for PEN1, 52% (12/23) for PEN2, and 79% (15/19) for steroids (overall p=0.001; p<0.0005 steroids v PEN1, and p=0.056 PEN2 v PEN1). After excluding those patients who were non-compliant during the first week (per protocol analysis), remission rates were 27%, 63%, and 79%, respectively (p=0.008, steroids and PEN2 v PEN1). After adjusting for confounding variables, PEN1 remained significantly associated with a poor response.
Conclusion: The type of dietary fat may be of importance for the primary therapeutic effect of enteral nutrition in active Crohn's disease.
- enteral nutrition
- Crohn's disease
- fat
- CD, Crohn's disease
- CRP, C reactive protein
- VHAI, Van Hees' activity index
- PEN, polymeric enteral nutrition
- NRI, nutritional risk index
- LRA, logistic regression analysis
- MCT, medium chain triglycerides
- LCT, long chain triglycerides
- EN, enteral nutrition
- MUFA, monounsaturated fatty acids
- PUFA, polyunsaturated fatty acids
- ESR, erythrocyte sedimentation rate
- CDAI, Crohn's disease activity index
Statistics from Altmetric.com
- CD, Crohn's disease
- CRP, C reactive protein
- VHAI, Van Hees' activity index
- PEN, polymeric enteral nutrition
- NRI, nutritional risk index
- LRA, logistic regression analysis
- MCT, medium chain triglycerides
- LCT, long chain triglycerides
- EN, enteral nutrition
- MUFA, monounsaturated fatty acids
- PUFA, polyunsaturated fatty acids
- ESR, erythrocyte sedimentation rate
- CDAI, Crohn's disease activity index
Three meta-analyses of randomised controlled trials comparing steroids and enteral nutrition (EN) in the treatment of active Crohn's disease (CD) showed that although steroids are more effective, the overall remission rate by intention to treat after EN is 60%,1–,3 substantially higher than the placebo response in trials evaluating drugs for CD.4–,6 Composite data from large uncontrolled and controlled series of EN in CD, after excluding non-compliant patients, also provide interesting information.7 Mean remission rate in adult patients treated for at least two weeks was 79% (42–100%; n=549) with amino acid based diets, and 70% (36–90%; n=124) with whole protein based formulas, indicating that when tolerated, EN is an effective therapy for CD.
The therapeutic mechanisms of EN in CD are unknown. Initial hypotheses suggested that the antigenicity of dietary protein would trigger bowel inflammation. Accordingly, amino acid based diets were used. However, meta-analyses failed to disclose differences in remission rates with amino acid, peptide, or whole protein based diets.1–,3 Fat composition has seldom been taken into account when comparing the effect of diets in CD. It has been hypothesised that changes in dietary fat may modify eicosanoid synthesis and other immunomodulatory mechanisms, thereby influencing disease outcome.8 Although the small sample size of trials comparing enteral formulas with different amounts of fat does not allow definite conclusions to be drawn, it has been suggested that the lower the EN fat content, the higher the remission rate obtained.8,9 Differences in the type of dietary fat may also be important as it may modulate the production of proinflammatory eicosanoids and cytokines,10,11 and the phosphatidylinositol-4,5-biphosphate and protein kinase C intracellular signalling systems.12,13 Therefore, we hypothesised that intermediate or high fat diets rich in n6 polyunsaturated fatty acid (PUFA) precursors of proinflammatory eicosanoids and cytokines would be less effective than those containing monounsaturated fatty acids (MUFA).8
To determine if the therapeutic effect of EN in active CD depends on their fat composition, we conducted a trial evaluating the ability of two whole protein based diets with different fat compositions (n6 PUFA v MUFA) to induce remission in active CD compared with steroids.
PATIENTS AND METHODS
Patients
Sixty two consecutive active CD patients entered the trial between January 1997 and April 1999. The study was approved by the ethics committees of the participating centres, and written informed consent was obtained from all patients.
Inclusion criteria were: (1) age 18–65 years; (2) diagnosis of CD based on established criteria14; (3) symptoms consistent with activity of the disease; (4) at least two of the following laboratory abnormalities indicative of active disease: erythrocyte sedimentation rate (ESR) >30 mm/h, haemoglobin <12 g/dl for males or 11.5 g/dl for females, platelets >350 000 cells/mm3, C reactive protein (CRP) higher than twofold the upper limit of normal range; and (5) Van Hees activity index (VHAI)15 >120.
Exclusion criteria were: (1) clinical evidence of intestinal perforation, toxic megacolon, massive gastrointestinal bleeding, complete intestinal occlusion, abdominal abscess, or mid jejunal fistulas which preclude the use of EN; (2) need for home artificial nutrition; (3) previous intestinal resection with a remnant bowel <1.80 cm with an ileostomy; (4) receiving >7.5 mg/day prednisone/prednisolone in the last month; (5) treatment with azathioprine, 6-mercaptopurine, cyclosporin, or other immunosupressors in the last three months; (6) severe extraintestinal complications (pyoderma gangrenosum, uveitis); (7) pregnancy or lactation; and (8) any serious illness that could limit life expectancy.
Study design
This was a multicentre, randomised, double blind (for EN only) study of parallel groups (involving six centres in Spain, the UK, and Germany) designed to evaluate the ability of two polymeric enteral diets to induce remission in active CD compared with prednisone. One diet was rich in n9 MUFA (oleic acid) (polymeric enteral nutrition 1 (PEN1)) whereas n6 PUFA (linoleic acid) predominated in the other (PEN2). Otherwise, the total amount of fat and other macronutrients was identical (table 1⇓).
Composition of the polymeric enteral nutrition (PEN) 1 and 2 diets
Patients were randomly assigned to receive one of the diets or steroids. In order to make the groups comparable, randomisation was stratified according to: (1) VHAI (≤170 versus >170); (2) location of disease (disease confined to colon versus other locations); and (3) new onset versus recurrent disease. Each centre had separate sets of sealed envelopes for each randomisation stratum.
Powdered diets (SHS International, Liverpool, UK) were of identical appearance and were supplied in identical coded sachets. The investigator, study staff, and patient were blinded to the diet assignment throughout the study. Patients with mild CD (VHAI ≤170) were fed as outpatients while moderate (VHAI >170 and <250) and severe (VHAI ≥250) cases were fed in hospital. Diets were sip fed in mild and moderate disease patients. Two flavouring additives (vanilla and chocolate) were available. In patients who found diets unpalatable and those with severe disease, pump assisted continuous intragastric infusion through a fine bore Silk-type feeding tube (Radius, Chicago, Illinois, USA) was used. No oral foods or fluids (except for water and weak tea) were allowed. Energy requirements were calculated using Long's equation modified by usual body weight.16 A starter regimen (80% of energy requirements on the first day, 100% by the second day onwards) was used.
Patients randomised to steroids received oral prednisone 1 mg/kg/day until remission (as defined below) was achieved. The EN groups were treated on an inpatient or outpatient basis according to the severity of CD, and were encouraged to eat a well balanced conventional diet throughout the study.
Aminosalicylates, rectal steroids, azathioprine, 6-mercaptopurine, cyclosporin, other immunosupressors, and parenteral nutrition were not allowed during the trial. Antidiarrhoeal agents were permitted when necessary.
Compliance with EN or steroids was checked at each visit by counting unopened diet sachets and from patient diary cards. Patients consuming <80% of the prescribed treatment dose throughout the study, or those who interrupted therapy for more than three consecutive days were considered non-compliant.
The primary end point was induction of remission, as defined by a VHAI <120 achieved after no more than four weeks on therapy. During treatment, patients were monitored weekly, and earlier completion was permitted if remission was achieved before this deadline. Treatment failure was defined as any of the following: (1) failure to decrease VHAI by 10% from baseline at week 2; (2) failure to achieve remission at week 4; and (3) development of severe disease complications (toxic megacolon, occlusion, perforation, massive gastrointestinal bleeding) during the trial. Treatment failure prompted the patient's withdrawal from the trial. In addition, patients were free to withdraw from the study at any time without giving a reason.
Biological activity parameters (ESR, CRP, serum fibrinogen), VHAI, Crohn's disease activity index (CDAI), nutritional risk index (NRI),17 per cent ideal body weight to height index, serum albumin, and handgrip strength were monitored weekly throughout the study. NRI (which includes albumin and weight loss) was used to define malnutrition (NRI <97.5) as described previously.17 Patients were required to complete a diary card the week before each visit to provide data for CDAI calculation and compliance assessment.
Statistics
The sample size was calculated to prove the hypothesis that PEN1 (MUFA diet) was more effective than PEN2 (n6 PUFA diet) in inducing remission in active CD. A 50% remission rate was expected with PEN2. A sample size of 40 patients per diet group was estimated to demonstrate a 30% increase in remission rate with PEN1 (80%) with a 5% type I error and a 20% type II error. Forty additional patients in the steroid arm were included as gold standard controls.
To protect against an obvious lack of efficacy of one of the diets, a stopping rule was defined. Failure to achieve a remission rate >33% in any of the arms, when at least 15 patients per arm had been included, and with highly significant differences (p<0.01) among groups, justified stopping the trial. An external observer was required at this time to decide whether or not the stopping rule should be applied. Investigators were blinded to the results of this interim analysis if the stopping rule was not applied.
Results were analysed on an intention to treat and per protocol (that is, excluding patients non-compliant with EN during the first week of therapy) basis. Results are expressed as mean (SEM) or percentage with 95% confidence intervals (CI). Differences in qualitative variables were assessed by χ2 statistics. Parametric or non-parametric (Kruskall-Wallis) one way ANOVA was used for quantitative variables. A stepwise logistic regression analysis (LRA) was performed to identify independent predictors of remission as per protocol. Only variables showing significant differences (p<0.05) between responders and non-responders in the univariate analysis were included in the LRA.
Statistical analyses were performed using SPSS for Windows (SPSS Inc., Chicago, Illinois, USA).
RESULTS
Patient characteristics
The trial was prematurely terminated because the stopping rule was applied after 62 patients had been included (20 treated with PEN1, 23 with PEN2, and 19 with steroids). Groups were homogeneous at baseline (table 2⇓). Nine patients who received EN (five PEN1, four PEN2) were excluded before completing one week of treatment due to poor tolerance (n=1) or refusal to continue (n=8). These patients did not differ clinically from evaluable cases (table 3⇓). After one week of therapy, all patients were compliant. In the diet groups, 19 patients were sip fed as outpatients and 24 were tube fed as inpatients. Five initially tube fed patients were changed to sip feeding later on. Actual daily EN intake was 2307 (76) kcal/day for PEN1 and 2266 (95) kcal/day for PEN2.
Patient characteristics at baseline in the polymeric enteral nutrition (PEN) 1 and 2 groups and the steroid group
Clinical characteristics of patients excluded during the first week because they were either non-compliant or refused to continue in the trial
Response to therapy
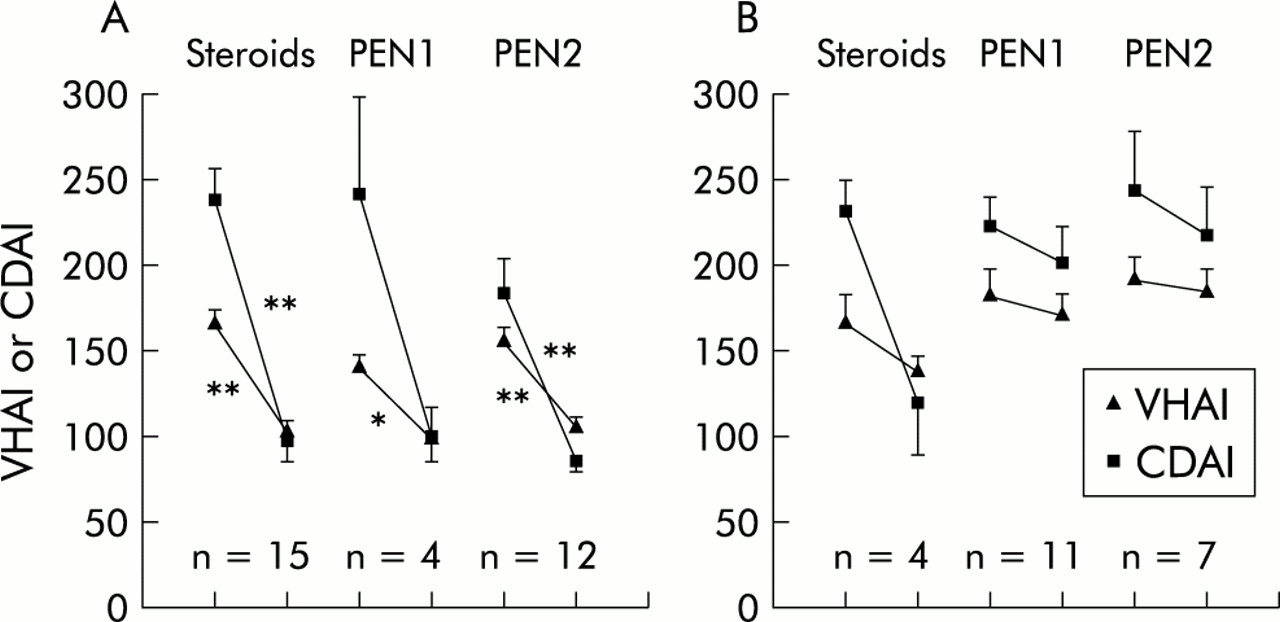
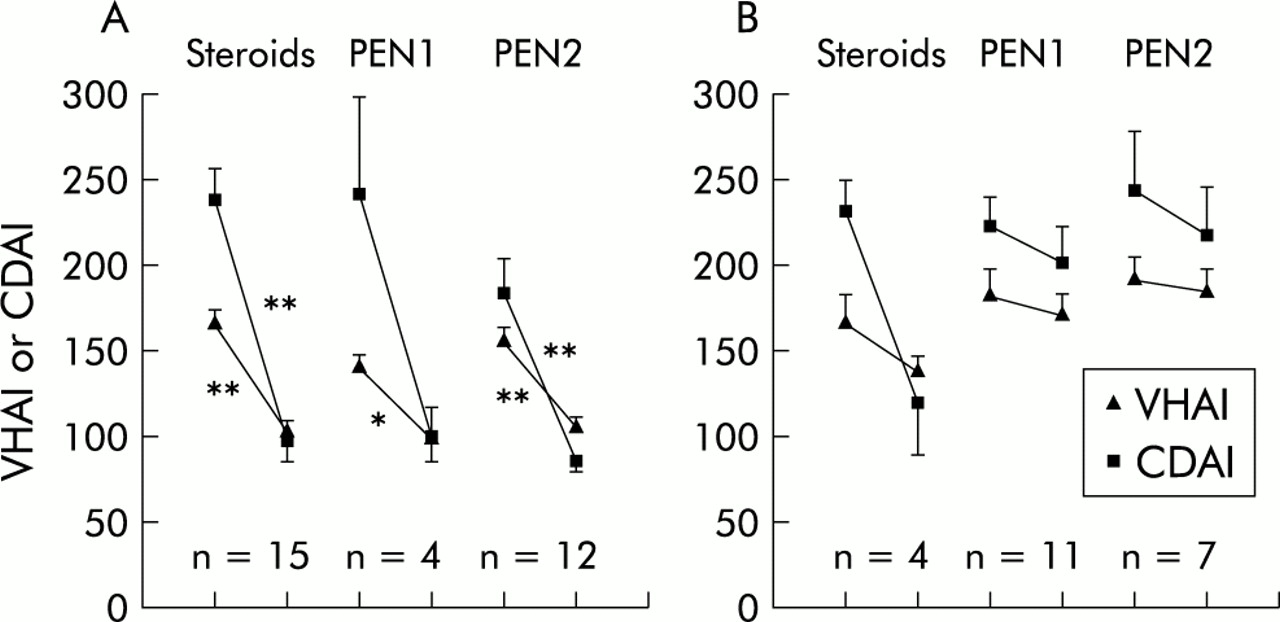
Remission rates for intention to treat were 20% with PEN1 (4/20), 52% with PEN2 (12/23), and 79% with steroids (15/19) (overall p=0.001; p<0.0005 steroids v PEN1, and p=0.056 PEN2 v PEN1). In the per protocol analysis, remission rates were 27%, 63%, and 79%, respectively (overall p=0.008; p=0.005 steroids v PEN1, and p=0.045 PEN2 v PEN1). Among responders, the time to achieve remission was similar with all treatments (PEN1 15.5 (5.5) days; PEN2 15.2 (1.7); steroids 13 (1.7) days; p=0.67), as were changes in activity indices, biological inflammatory parameters, and nutritional variables (table 4⇓). Mean VHAI and CDAI scores at baseline and at the end of the trial in responders and non-responders are shown in fig 1⇓.
Per cent change in clinical activity indexes, biological parameters of inflammation, and nutritional parameters in those patients who achieved clinical remission in the polymeric enteral nutrition (PEN) 1 and 2 groups and the steroid group
{kind=link}
Values for Van Hees' activity index (VHAI) and Crohn's disease activity index (CDAI) at baseline and at the end of the trial in patients who achieved remission (A) and in those who did not achieve remission (B) after administration of polymeric enteral nutrition (PEN) 1, PEN2, or steroids. Values are mean (SEM). *p=0.02, **p<0.005.
Univariate analysis showed that sex, new onset/recurrent disease, VHAI, disease location, and treatment were predictors of response. These variables were included in a stepwise LRA which showed that after adjusting for confounding variables, PEN1 treatment was still significantly associated with a poor response (odds ratio 0.12; 95% CI 0.02–0.63). In addition, a VHAI >170 was unfavourably related to remission (odds ratio 0.05; 95% CI 0.006–0.41).
Nutritional status
At entry, malnutrition was more frequent in the EN groups than in the steroid group, although differences were not significant (PEN1 80%; PEN2 78%; steroids 55%; p=0.17) (table 2⇑). Three patients on steroids and seven in each diet group were severely malnourished (NRI <83). Only one patient in the PEN2 group remained mildly malnourished after remission. Per cent increase in NRI was similar among groups (table 4⇑).
Adverse events
In addition to the nine patients who withdrew within the first week (see above), eight patients on PEN1, seven on PEN2 , and 10 on steroids reported therapy related adverse events (table 5⇓) which were always mild and did not require treatment discontinuation. However, the amount of diet prescribed had to be slightly reduced in three patients.
Summary of patients with adverse events (AE) in the polymeric enteral nutrition (PEN) 1 and 2 groups and the steroid group
DISCUSSION
This is the first trial which has compared the effect of two enteral diets with identical macronutrient distribution, but different qualitative fat composition, on induction of remission in active CD. Our hypothesis was that a high fat EN (≈30% of energy as fat) with predominant MUFA would be more effective than a diet with mostly n6 PUFA, as excess of the precursor linoleic acid, which is converted to arachidonic acid, results in an increase in strong proinflammatory eicosanoids and cytokines.10 Surprisingly however, the MUFA diet was significantly less effective than the n6 PUFA diet, the remission rate of the former being similar to the placebo response in recent trials.4–,6 However, this is the first trial to show that fat may play a key role in the primary therapeutic effect of EN in active CD.
Our results are based on a sample smaller than was initially estimated as the study was prematurely terminated because the predefined stopping rule was applied. In spite of this, we believe we can be confident of the lower efficacy of the MUFA diet as the groups were homogeneous at entry, and remission rates were lower with this diet in all subgroups of patients analysed (data not shown).
Failure of the MUFA diet was unexpected. In a previous study, we found that high fat oleate based EN was as effective as steroids in inducing remission in active CD (80% on an intention to treat basis).18 These data, and review of the results with EN in other trials, led us to hypothesise that diets with either very low total fat or high in MUFA would be particularly effective in CD.8 Middleton and colleagues9 compared two high fat oleate based enteral diets and obtained 68% and 50% remission rates by intention to treat (92% and 55% after excluding non-compliant patients). As in our study, oleic acid was almost the sole fatty acid (67% of total fat) in the diet with the lowest remission rate. The authors performed a meta-analysis of published studies and suggested that the beneficial effect of EN was inversely related to the amount of dietary long chain triglycerides (LCT).9 In the present study, there was no difference in the amount of LCT between diets, arguing in part against this hypothesis, and suggesting that qualitative changes in dietary fat may also be important. However, the possibility that low fat diets could be better than high fat diets deserves investigation.
The reasons for the discrepancies between the results of previous studies using MUFA diets and those of the present trial are elusive. Cell culture studies have shown that the immunomodulatory effect of fat varies when cells are incubated with isolated fatty acids or with fatty acid mixtures.19 Thus the pro- or anti-inflammatory effect of fat could depend more on a certain fatty acid profile than on a single fatty acid. In the present trial, the proportion of oleic acid in the MUFA diet was particularly high (79% of total fat). It seems evident from this and Middleton's study that oleic acid does not have any anti-inflammatory effect per se in active CD. High fat oleate based diets associated with high remission rates in previous studies contained moderate amounts of both oleic acid and saturated fat (about 40% for both), including a substantial amount of medium chain triglycerides (MCT), and had low amounts of linoleate.9,18 In addition, the source of oleic acid in the best performance diet from Middleton's study was canola oil, which also contains a substantial amount of α-linolenic acid (the precursor of n3 PUFA).9 In this regard, it should be noted that recent experimental studies suggest that MCT (coconut oil) and n3 PUFA (fish oil) have anti-inflammatory effects, oleic acid (olive oil) has a neutral or, at best, mild anti-inflammatory effect whereas linoleic acid (safflower oil) has a proinflammatory effect.11 These effects must be explored further using different fatty acid mixtures in both animal and human studies.
The source of oleic acid in the present trial was synthetic trioleate whereas in our previous study olive oil was used.18 Olive oil contains phenols and other non-fatty compounds with potent antioxidant capacity whereas seed oils are in general devoid of these.20 Therefore, the different effects of vegetable oils may also be ascribed, at least in part, to their different antioxidant capacity.
The modest remission rate associated with our n6 PUFA diet compares well with what we anticipated from published meta-analyses.1–,3 Although it did not differ from the value obtained with steroids (p=0.11), this was clearly due to the small sample size. Nevertheless, the remission rate with the n6 PUFA diet was similar to that obtained with budesonide, a drug currently used for the treatment of ileocolonic CD.6,21,22
In summary, this study suggests that the type of fat in EN may be of importance in inducing remission in active CD, and that an excess of synthetic oleate in the enteral diet may preclude this effect or even be detrimental in these patients.
Acknowledgments
We are grateful to SHS International (Liverpool, UK) for manufacturing the diets and to Dr Xavier Alvarez for his technical assistance. This work was presented at the 101st Annual Meeting of the AGA, San Diego, May 21–24, 2000.