Article Text

Abstract
Background: Hereditary non-polyposis colorectal cancer (HNPCC) is thought to arise from adenomas. HNPCC mostly occurs in the proximal colon. We investigated whether this proximal preponderance is due to a proximal preponderance of adenomas or (also) differences in transformation rates from adenomas to cancer between the distal and proximal colon.
Methods: A total of 100 HNPCC adenomas were evaluated and compared with 152 sporadic adenomas for location, size, and dysplasia. Twenty five adenomas from patients with a known mismatch repair (MMR) gene mutation were stained for expression of MLH1 and MSH2.
Results: HNPCC adenomas were more often located proximally (50% v 26%; p=0.018) and were smaller in comparison with sporadic adenomas. They were similarly dysplastic. However, all proximal HNPCC adenomas ≥5 mm were highly dysplastic compared with 17% of the larger proximal sporadic polyps (p<0.001). They were also more often highly dysplastic than larger distal HNPCC adenomas (p<0.001). Small HNPCC adenomas were, except for their location, not different from sporadic adenomas. Fifteen of the 25 “known mutation” adenomas showed loss of expression of either MLH1 or MSH2. The 10 adenomas with expression were all small with low grade dysplasia.
Conclusion: HNPCC adenomas are located mainly in the proximal colon. The progression to high grade dysplasia is more common in proximal than distal HNPCC adenomas, indicating a faster transformation rate from early adenoma to cancer in the proximal colon. MMR gene malfunction probably does not initiate adenoma development but is present at a very early stage of tumorigenesis and heralds the development of high grade dysplasia.
- hereditary non-polyposis colorectal cancer
- adenomas
- dysplasia
- mismatch repair
- proximal colon
- adenoma-carcinoma sequence
- HNPCC, hereditary non-polyposis colorectal cancer
- MMR, mismatch repair
- PBS, phosphate buffered saline
- BSA, bovine serum albumin
Statistics from Altmetric.com
- hereditary non-polyposis colorectal cancer
- adenomas
- dysplasia
- mismatch repair
- proximal colon
- adenoma-carcinoma sequence
- HNPCC, hereditary non-polyposis colorectal cancer
- MMR, mismatch repair
- PBS, phosphate buffered saline
- BSA, bovine serum albumin
For the first time, researchers have obtained indisputable data supporting the use of contemporary colorectal cancer prevention procedures in hereditary non-polyposis colorectal cancer (HNPCC) syndrome.1 These data reveal a significant patient survival advantage and a reduction in the incidence of colorectal tumours following colonoscopic screening and polypectomies. This complies with the accepted adenoma-carcinoma sequence theory that states that adenomas are a precursor in the tumorigenesis of malignant HNPCC lesions.2–,4
The malignant lesions, often occurring at a relatively young age, are well described in HNPCC. They are located predominantly in the proximal part of the colon, and there is a high incidence of synchronous and metachronous cases. Microscopically, the tumours are characterised by a Crohn's-like lymphoid reaction, a mucinous component, and poor differentiation.5–,10 Studies on adenomas in HNPCC are less consistent. When calculating the average distribution of HNPCC adenomas in the literature, 45% (range 27–70%) were located in the proximal colon.1, 9, 11–,14 Some reported an obvious propensity for right sided neoplastic lesions15 while others observed a distribution of adenomas in HNPCC patients similar to that in the general population.13, 16, 17
The adenoma-carcinoma sequence in HNPCC seems to be accelerated. This is especially illustrated by the relatively frequent occurrence of cancers within the first few years after a “clean” colon had been confirmed by colonoscopy.14, 15, 18, 19 In addition, several authors reported that HNPCC adenomas frequently have a villous component and high grade dysplasia, two assumed markers of increased risk of developing cancer.9, 11, 14, 20 However, whether this is a uniform feature of all HNPCC adenomas at every location in the colon has yet to be determined. The ratio of proximal to distal cancers in HNPCC (7:3) is higher than the reported ratio for adenomas (4:5). Thus it seems that not all HNPCC adenomas have an increased risk of malignant transformation and that there are regional differences in this respect.
In order to examine these issues, we compared adenomas resected from HNPCC patients with sporadic adenomas. More importantly, we investigated whether differences exist between proximal, distal, and rectal HNPCC adenomas.
Methods
Patients
According to the prevention guidelines of the International Collaborative Group on HNPCC (ICG-HNPCC), patients fulfilling the Amsterdam criteria and/or with a germline mismatch repair (MMR) gene mutation should undergo a colonoscopy every two years starting at the age of 25 years.21–,23 At the University Hospital of Groningen, 136 subjects belonging to 47 families participated in a surveillance programme. We included all subjects with a positive colonoscopy in our study group: 46 (24 male and 22 female) patients with a median age of 50 (range 25–78) years at polypectomy. Sixty nine colonoscopies, a mean of 1.6 per patient (range 1–5), yielded 100 adenomatous polyps (55 from men and 45 from women) over a 12 year period from 1988 to 2000. Four polyps found in a subtotal colectomy specimen were also included. Seven patients had previously been diagnosed with cancer and had part of their colon resected.
The data were compared with findings from a control group consisting of sporadic adenomas consecutively removed during sigmoido- and colonoscopy at the Endoscopy Centre, University Hospital of Groningen in 1997. Lesions from patients with a strong positive family history of colorectal cancer or patients with ulcerative colitis, Crohn's disease, or familial adenomatous polyposis were excluded. According to the protocol, patients with an adenoma detected at sigmoidoscopy should subsequently undergo colonoscopy: except for two patients, the entire large bowel was inspected in each subject.24 The group of sporadic adenomas consisted of 152 adenomas and had a similar male-female ratio as the HNPCC group (84 lesions in men and 68 in women). Mean age at polypectomy was 64 (range 24–90) years.
Location
The location of the adenomas was retrieved from endoscopy or pathology reports. The caecum and ascending and transverse colon are regarded as the proximal or right sided colon while the descending and sigmoid colon are referred to as the distal or left sided colon. The third location of the adenomas was the rectum.
Histological examination
Thin slides (3 μm) were made of each formalin fixed paraffin embedded polyp and stained with haematoxylin-eosin. Two of the authors (FEMR and HH) reviewed and scored three characteristics of the adenomas: (1) Size of the polyp—the microscopic measurement of the polyp's circumference: <5 mm (small) and ≥5 mm (large); (2) histological subtype—tubular or having more than a 25% villous component; (3) grade of dysplasia—low or high (WHO guidelines25).
The adenomas, 25 in total, which were removed from patients with a known mutation or belonging to a family with a known mutation were further analysed for MMR protein status by immunohistochemistry. Monoclonal mouse antibodies against MLH1 (clone G168-728; Pharmingen, San Diego, USA) and MSH2 (Ab-2; Calbiochem, San Diego, USA) protein products were used. The paraffin sections (3 μm) were fixed onto 3-aminopropyltriethoxysilane (APES; Sigma-Aldrich, Diesenhofen, Germany) coated slides, stretched for 30 minutes at 60°C, and dried overnight at 37°C. The sections were deparaffinised in xylene (2×10 minutes) and rinsed in 100% alcohol. The optimal antibody-antigen reaction was obtained by immersing the section in 200 μl of blocking reagent (2% block and 0.2% sodium dodecyl sulphate in maleic acid, pH 6.0; Boehringer Mannheim, Germany) and using a high pressure cooker for three sessions of five minutes at 115°C, alternating with five minutes of incubation in a humid environment. After cooling for the third time, endogenous peroxidase activity was quenched by incubation with 30% H2O2 in phosphate buffered saline (PBS) for 30 minutes. Following thorough washing in PBS, sections were immersed with the specific antibody in PBS with 1% bovine serum albumin (BSA) at a dilution of 1:500 for MLH1 and 1:100 for MSH2 antibody for one hour. Subsequently, the sections were washed three times with PBS and consecutively incubated for 30 minutes with rabbit antimouse peroxidase and goat antirabbit peroxidase diluted (1:50) in PBS-1% BSA. The sections were submerged for 10 minutes in a solution of 50 mg 3`-3`diaminobenzidine in PBS and 50 mg of imidazol with 30% H2O2, used as substrate for peroxidase. After rinsing with demi water, sections were counterstained with haematoxylin, washed with running water, and dehydrated with graded alcohol, dried, and covered with a slide.
Statistical analyses
Statistical comparisons between HNPCC and sporadic adenomas and within the two groups were made using the Mann-Whitney test when comparing a characteristic (size, type, and dysplasia) with two variables and the corrected χ2 test was used for comparisons of a characteristic (location) with three variables. A p value of less than 0.05 was considered statistically significant.
RESULTS
Considering the two entire groups of adenomas (table 1⇓), a significant difference was observed in location, size, and histology of HNPCC adenomas compared with sporadic adenomas (p=0.018, p<0.001, and p=0.010, respectively). HNPCC adenomas had a proximal propensity (50% v 26% of sporadic adenomas). The adenomas showed a wide range of sizes in both groups. The median size of HNPCC adenomas was 2.0 mm (range 0.5–34) while sporadic adenomas had a median size of 5.5 mm (range 0.5–45). HNPCC adenomas were more often tubular in comparison with sporadic adenomas. Even though the HNPCC adenomas were more often small and tubular, they were similarly dysplastic as the larger and more often villous sporadic adenomas.
Characteristics of hereditary non-polyposis colorectal cancer (HNPCC) and sporadic adenomas
The proximal propensity was more evident in highly dysplastic HNPCC adenomas: high grade dysplastic HNPCC adenomas were more often (55%) located proximal to the splenic flexure while only six (15%) of the high grade sporadic polyps were right sided (p<0.001).
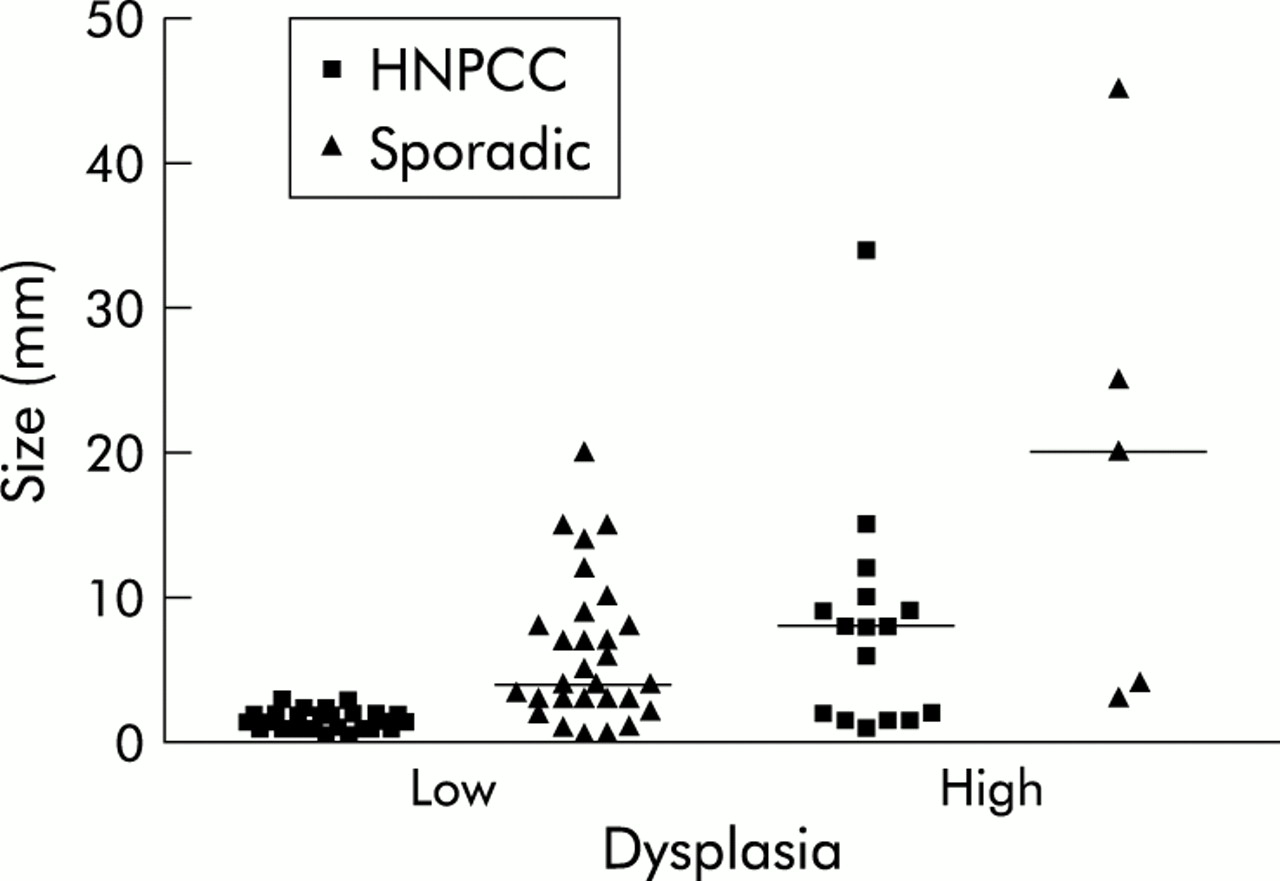
In the proximal colon, HNPCC adenomas were smaller in comparison with sporadic polyps (p=0.025) but they were more often highly dysplastic (36% v 13%; p<0.020) (fig 1⇓). When comparing size as well as dysplasia at one location (tables 2, 3⇓⇓), the difference between the HNPCC and sporadic adenomas was clearly apparent. Larger HNPCC polyps (≥5 mm) in particular, in the proximal colon, were more often highly dysplastic (p<0.001): in fact, all HNPCC adenomas ≥5 mm were highly dysplastic. In the sporadic lesions this was not observed: only 25% of the large sporadic polyps at this site had high grade dysplasia.
Dysplasia of hereditary non-polyposis colorectal cancer (HNPCC) adenomas by location and size
Dysplasia of sporadic adenomas by location and size

{kind=link}
Distribution of proximal hereditary non-polyposis colorectal cancer (HNPCC) and sporadic adenomas by size and dysplasia (the horizontal lines indicate median size).
In the rectum, large HNPCC adenomas were also more often highly dysplastic in comparison with sporadic adenomas ≥5 mm. However, this difference was only borderline significant (p=0.084). HNPCC adenomas in the distal colon were smaller than distal sporadic lesions (66% v 39% <5 mm; p=0.047), mostly tubular (72% v 59%; NS), and nearly always low grade dysplastic (86% v 63%; p=0.020).
A significant difference was not only observed between the HNPCC and sporadic groups but also between the large HNPCC adenomas at the three locations. The large proximal HNPCC adenomas were more often highly dysplastic (100% were highly dysplastic) than HNPCC adenomas in the distal colon (22%; p=0.001) whereas a borderline significant difference was detected between proximal and rectal adenomas (75% highly dysplastic; p=0.07). The large HNPCC adenomas in the rectum were also significantly more often highly dysplastic in comparison with the HNPCC adenomas in the distal colon (p<0.03).
Eleven adenomas belonged to patients with a proven MLH1 mutation while 11 adenomas were removed from patients with a proven MSH2 mutation. Three adenomas were from two subjects who had not undergone genetic testing but a MLH1 mutation had been detected in their families. In total, 15 adenomas, eight low grade and seven high grade dysplastic, showed loss of expression of either MLH1 or MSH2. The three adenomas from the two patients who had not undergone genetic testing all showed loss of MLH1 staining, corresponding to the known mutation in their kindreds. Eight adenomas with loss of MLH1 expression were located in the proximal colon and two were situated in the rectum. Loss of MSH2 expression was observed in three distal, one proximal, and one rectal polyp. The 10 adenomas, all from proven carriers, that had normal expression of MMR proteins were small and low grade dysplastic. Three of these adenomas were located in the proximal colon, four in the distal colon, and the remaining three were located in the rectum.
DISCUSSION
Our results differ from previous studies concerning morphological descriptions of adenomas in patients at risk of HNPCC. The results support the accelerated adenoma-carcinoma sequence of carcinogenesis in HNPCC but at the same time strongly suggest that lesions at different locations, proximal or distal in the colon or in the rectum, behave differently in this respect. More specifically, similar to the high frequency of hereditary non-polyposis colorectal carcinomas proximal to the splenic flexure, HNPCC adenomas have a right preponderance, although less so than carcinomas, and these right sided adenomas are more prone to malignant conversion compared with left sided adenomas.
The large group of HNPCC adenomas included in this study is representative of the Groningen HNPCC population as they comprise all the available benign neoplastic lesions consecutively removed over a 12 year period. The majority of HNPCC adenomas were obtained during surveillance examinations while sporadic adenomas were acquired during colonoscopy to diagnose clinical symptoms such as rectal blood loss, diarrhoea, and abdominal pain. The groups are thus not readily comparable and this probably explains why the HNPCC adenomas were smaller, more often tubular, and not more dysplastic than sporadic adenomas, findings in contrast with reports in the literature.9, 11, 20, 26, 27 It is noticeable however that the small and tubular HNPCC adenomas were not less dysplastic than the larger and more often villous sporadic cases, as would be expected.27 To reduce the discrepancy arising from comparing adenomas obtained through surveillance and diagnostic colonoscopies, we also evaluated only the index HNPCC adenomas, those adenomas found during the first colonoscopy (data not shown). The characteristics of these index neoplastic lesions did not differ from those of all HNPCC adenomas reported in the present study. In accordance with Green's observation, they were mostly small and tubular.28 The same team of gastroenterologists performed all colonoscopies. The number of small (<5 mm) HNPCC and sporadic adenomas in all sections of the colon illustrates the thorough endoscopic search in both groups throughout the entire colon. Nevertheless, we cannot exclude the fact that greater care was taken in the examination of the colons of HNPCC subjects than of those of other patients.
The prevalence and grade of dysplasia of adenomas in the general population differ with regard to sex, age, and geographic region.27, 29, 30–,35 Any bias was minimised by including the same male to female ratio of adenomas in both groups. A sufficient number of age matched subjects however was not available. The histological characteristics of our control group were similar to those of Griffioen et al in another Dutch clinical investigation.36 The results from the control group also correspond to findings of several other studies.37, 38 However, other reports, mainly autopsy and surveillance studies, favour a substantially higher frequency of low grade dysplastic sporadic polyps and a lower frequency of villous lesions.17, 27, 30, 33 The proportion of proximal adenomas varies in the literature between 11% and 40% (Griffioen et al 17%36).
The essential role of the proximal colon in the pathogenesis of HNPCC is evident from numerous reports of the high incidence of right sided (interval) carcinomas in HNPCC patients.1, 6–8, 10, 12, 14, 39–,42 In accordance with this, we found that HNPCC adenomas were located more often in the proximal colon than sporadic ones. The proximal propensity suggests alteration in the initiation of neoplastic growth in HNPCC in comparison with the general population. A recent report on the presence of microsatellite instability in both hyperplastic and dysplastic aberrant crypt foci in the colons of HNPCC patients also suggests a possible role for MMR dysfunction in the initiation of neoplastic lesions in HNPCC.43 However, Leach and others proposed that the adenomas in HNPCC develop on a sporadic basis only to provide a substrate for defective DNA MMR genes.44
We therefore attempted to substantiate Leach's theory or the “initiation” proposal by performing immunohistochemistry for gene products of MLH1 and MSH2 on adenomas from subjects with a known mutation. In accordance with most reports, absence of immunohistochemical staining was seen in two thirds of HNPCC adenomas—that is, in 44% of low grade and in all high grade dysplastic adenomas.45–,50 Thus our data strongly suggest that DNA repair deficiency is not responsible for the initiation of an adenoma but determines the subsequent progression of the lesion. Although MMR dysfunction is not the first event, it is surely a very early occurrence in the tumorigenesis of HNPCC lesions and it heralds development to high grade dysplasia.
Our results illustrate that the proposed accelerated adenoma-carcinoma sequence in HNPCC is probably site specific—that is, limited to the proximal colon. While the group of HNPCC adenomas as a whole did not exhibit features of increased susceptibility to malignant conversion in comparison with sporadic adenomas, a difference was observed within the group of adenomas proximal to the splenic flexure. The large (≥5 mm) HNPCC adenomas in the proximal bowel were highly dysplastic suggesting more advancement in the malignant transformation than sporadic polyps of a similar size at this location. This and the fact that nine of the 15 HNPCC adenomas that showed loss of protein expression were located in the proximal colon emphasise the predilection of the proximal colon for tumorigenesis in HNPCC. Characteristics of HNPCC adenomas at specific sites in the large bowel have had limited attention to date as authors have only reported results on HNPCC adenomas in general. In contrast, sporadic adenomas have been described with regard to location. The National Polyp Study observed an increased frequency of high grade dysplasia in adenomas located distal to the splenic flexure but attributed this mainly to increased size and a villous component rather than to location per se.27 Nusko et al reported that sporadic right sided adenomas have a lower risk of becoming malignant compared with sporadic left sided adenomas.51 The reason for the reverse situation in HNPCC is still unclear.25, 52–,54
In conclusion, half of the HNPCC adenomas were located in the proximal colon but this does not fully explain the proximal propensity of cancers. Our data showed that progression to high grade dysplasia was more common in proximal than in distal HNPCC adenomas, indicating a faster transformation rate from early adenoma to cancer in the proximal colon. MMR gene malfunction probably does not initiate adenoma development but is present at a very early stage of tumorigenesis and seems to herald the development of high grade dysplasia. At this time there is no explanation for this site specific behaviour of HNPCC lesions or for the susceptibility of epithelial cells in the proximal colon to somatic MMR gene mutations.
Acknowledgments
This study was supported by the Dutch Cancer Society, grant RUG 98-1660.
REFERENCES
Linked Articles
- Commentaries