Article Text

Statistics from Altmetric.com
Intravenous corticosteroids have been the mainstay of treatment in severe ulcerative colitis since the landmark trials of Truelove et al in 1955 and 1974.1 2 However, as recently documented in a systematic review of cohort studies, one-third of adult patients hospitalised with severe ulcerative colitis fail to respond to such therapy.3 In comparison to adult-onset ulcerative colitis, paediatric-onset disease is more often extensive,4 5 suggesting that severe exacerbations might be more common. However, to date, only three small retrospective studies (44 patients in total) have reported the short-term corticosteroid response rate of severe colitis occurring in children.4 6 Moreover, although several investigators have developed indices predictive of steroid failure in adults, including the rules of Travis, Lindgren, Seo, and Ho,7–10 no such analyses have been performed in paediatric populations.
We retrospectively reviewed admissions of children and adolescents with active ulcerative colitis hospitalised for intravenous corticosteroid therapy at The Hospital for Sick Children (SickKids), Toronto, over a 10-year period. Specifically, we aimed to (1) determine the incidence of severe exacerbations of paediatric ulcerative colitis using both population census and patient cohort data; (2) evaluate the short-term response rates and longer term outcomes following intravenous corticosteroid therapy; and (3) evaluate predictors of response, thereby guiding timing of second-line therapy in young patients. We hypothesised that the higher prevalence of extensive disease in children compared with adults would result in a high frequency of severe exacerbations necessitating hospitalisation, and a high rate of steroid failure.
METHODS
This was a single-centre, retrospective, longitudinal cohort study approved by the local Institutional Review Board. We searched the hospital electronic database for ulcerative colitis-related admissions during the period 1991–2000, using the International Classification of Disease, ninth revision, Clinical Modification (ICD-9-CM) codes for ulcerative colitis (556.x). The charts of all potential patients were retrieved and reviewed in duplicate.
Ulcerative colitis patients aged 2–18 years were included if they were admitted to SickKids for initiation of treatment with intravenous corticosteroids. The diagnosis of ulcerative colitis was confirmed in all patients using established clinical, endoscopic and histological criteria.11 12 Patients documented to have an intercurrent enteric infection were excluded. To avoid repeated measures bias, it was decided a priori to consider only the first eligible admission for patients with more than one hospitalisation. Three major analyses were performed: (1) incidence of ulcerative colitis exacerbations requiring intravenous corticosteroid therapy; (2) outcomes with therapy; and (3) identification of predictors of steroid failure.
During the first 6 years of the study period, no paediatric gastroenterologist in the Greater Toronto Area (GTA) cared for hospitalised inflammatory bowel disease (IBD) patients outside of SickKids, and adult gastroenterologists did not independently manage children with IBD under the age of 15 years.13 Hence, younger patients with postal codes indicating residence in the GTA, who were treated at SickKids during this time period, approximated a population-based cohort.13 Patients, 15 years of age and over, and all children with postal codes indicating residence outside of the GTA, may have constituted a tertiary referral cohort, and were excluded from the epidemiological analysis. The corresponding age-matched GTA population of healthy children was derived by averaging the data from the 1991 and 1996 Canadian censuses for the GTA. Census tract was assigned according to the 1996 Canadian census and by Statistics Canada’s Postal Code Conversion File Plus.14
To estimate the prevalence of severe exacerbations among children with ulcerative colitis, we expressed the number of hospitalised GTA children as a percentage of the total number of GTA-resident children with ulcerative colitis followed by the SickKids IBD programme during the time period.
Data were extracted by R.A.M., C.M.W. and C.C. using explicit standardised forms. All charts were independently reviewed by D.T. and discrepancies were solved by consensus. Data were entered into a customised database using Access® 2003 Professional (Microsoft Corporation, Redmond, WA). Intravenous corticosteroid therapy at this institution is given either as methylprednisolone 1–1.5 mg/kg/day, usually up to 60 mg daily in two divided doses, or equivalent doses of hydrocortisone (standardised in this report as methylprednisolone-equivalent dosing by a 1:5 conversion ratio). 5-ASA preparations are not prescribed to patients hospitalised for treatment of severe ulcerative colitis and antibiotics are administered to febrile children only. During the study period, available second-line drugs were ciclosporine and tacrolimus as previously described.15
Clinical and laboratory values were recorded at admission, on the third and fifth day of corticosteroid treatment, and at introduction of second-line therapy (if applicable). Outcome data were summarised at short-term (i.e. upon discharge), medium-term (i.e. 1-year follow-up) and long-term follow-up (i.e. upon transfer to adult care or most recent follow-up). Disease activity at baseline was determined using the Pediatric Ulcerative Colitis Activity Index (PUCAI), a recently developed and validated non-invasive multi-item disease activity measure (see Addendum).6 The clinical prediction rules of Travis (i.e. the Oxford index),9 Lindgren (i.e. the fulminant colitis index)10 and Seo,7 as well as the PUCAI were calculated on the third and fifth days of corticosteroid therapy. In this paediatric population, it was not possible to calculate Ho’s index8 as the item of colonic dilatation may be age dependent and there is no existing nomogram to standardise colonic width according to age. Therefore we retrieved and analysed the radiographs of our cohort. Plain abdominal radiographs, performed during the first 3 days of therapy, were independently reviewed by two paediatric radiologists blinded to the clinical and outcome data. Each radiologist completed a standardised form, including maximal supine transverse colon and small bowel luminal width, presence of free air, air-fluid levels in the upright position, portal venous air, mucosal ulcerations (i.e. thumb printing) and haustral thickening.
Statistical analyses
The proportion of steroid-refractory children (defined by the requirement of second-line drugs or colectomy during the hospitalisation) was calculated with the corresponding 95% confidence interval (CI). The others, considered steroid-responsive, were further classified with respect to steroid dependency (defined by requirement of steroid therapy for more than 6 months in the subsequent year).
Predictors of response
To determine predictors of steroid failure, descriptive univariate analysis was performed on predefined potential predictors at admission, and on days 3 and 5 of therapy. The χ2 or Fisher’s exact tests were used to compare categorical variables (such as gender and disease extent). Continuous variables (such as steroid dose, and days of bloody diarrhoea) are presented as mean ± SD or median [interquartile range (IQR)] and compared using the unpaired Student t test or the Wilcoxon rank sum test, as appropriate. To compare weight loss between responders and non-responders, analysis of covariance (ANCOVA) was used with admission weight as the dependent variable and the weight at 1 month previously as the covariate. Unadjusted logistic regression was used to obtain the corresponding odds ratio (OR) for each predictor. Multivariate logistic regression was then modelled to associate predictors with corticosteroid failure. Variable screening for predictive models based on statistical significance leads to unreliable models,16 and it has been strongly recommended that the possible predictors be set a priori based on extensive literature review and expert opinion.16 17 We selected variables that were consistently reproduced in the literature,3 modified for paediatric populations: number of bowel movements, CRP, albumin, weight loss and blood in stool. Heart rate was not selected due to the difficulty of assessment and standardisation in young children, and fever was not selected due to rarity in children with ulcerative colitis.6 18 Governed by maximising c-statistics, we tested whether modifications of the selected variables improved the model fit (i.e. counting only stools containing blood, only nocturnal stools, per cent weight loss, and change in scores since previous assessment at days 3 and 5). Time to colectomy during the entire follow-up was analysed by the non-parametric Kaplan–Meier survival estimate and strata were compared using the log rank test.
Agreement between the two radiologists was assessed using the intraclass correlation coefficient (ICC, using Shrout and Fleiss’s two-way random ANOVA model ± 95% CI19 reporting the “average measures” value in the SPSS output) for continuous variables (i.e. bowel width and number of air-fluid levels) and kappa statistics for discrete variables.
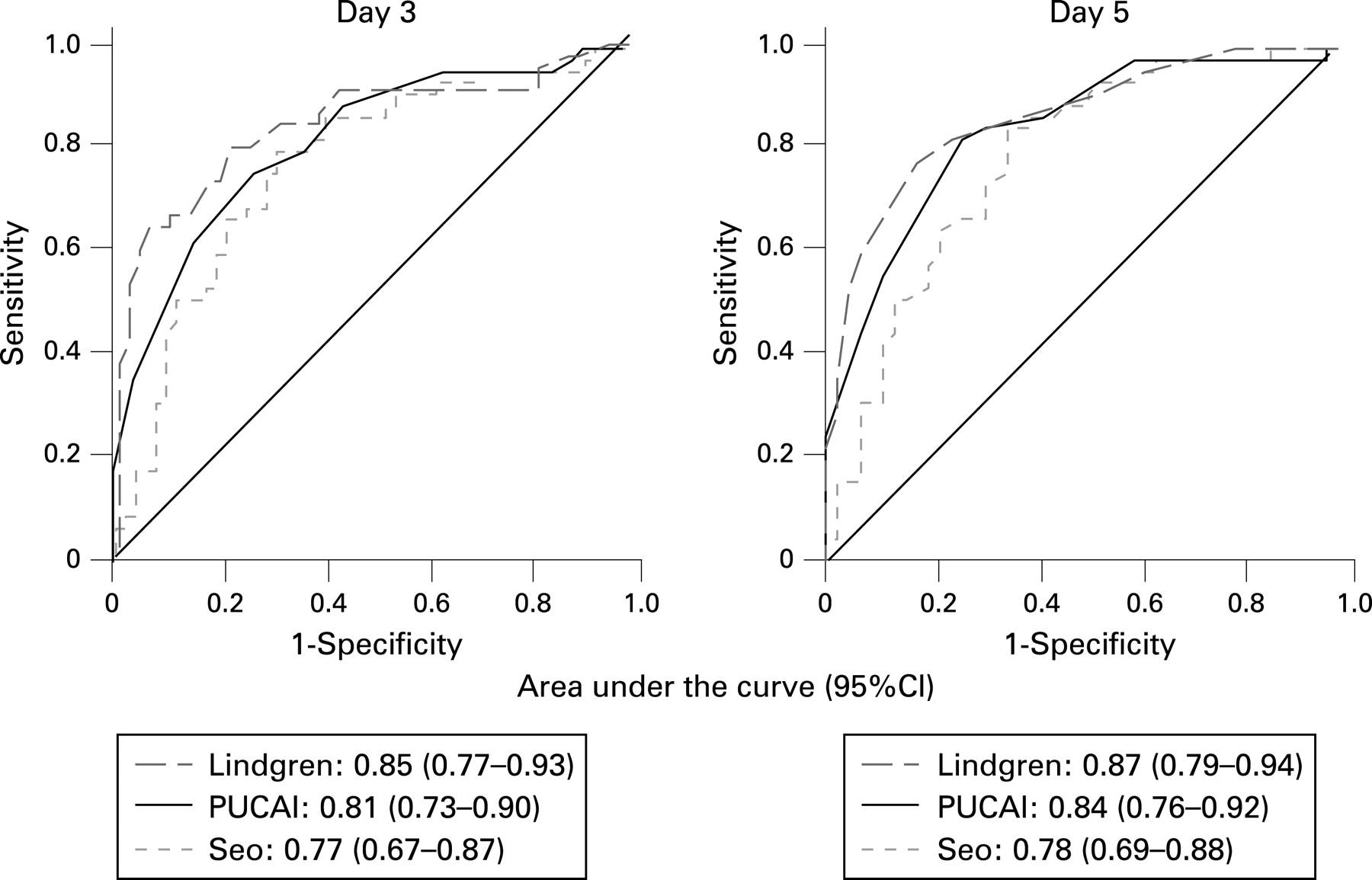
Sensitivity, specificity, predictive values and likelihood ratios were computed for the previously developed predictive indices (i.e. Travis, Seo, and Lindgren indices) as well as the PUCAI, and compared using a receiver operating curve (ROC). Tests achieving an area under the ROC curve (95% CI) of over 0.7 were considered fair tests, 0.8 was good, and those achieving over 0.9 were excellent tests. All comparisons were made using two-sided significance levels of p<0.05. Statistical analyses were performed using SAS V9.1.3 (SAS Institute Inc., Cary, NC) and SPSS V15.0 (SPSS Inc., Chicago, IL).
RESULTS
Patients
A total of 114 children were hospitalised at SickKids for treatment of acute ulcerative colitis during the 10-year study period. Fifteen in whom an intercurrent enteric pathogen was identified were excluded (including five children with Clostridium difficile infection). Descriptive statistics of the remaining 99 children are presented in table 1. Mean PUCAI scores at admission were similar in the new onset patients [PUCAI 69 (SD 12.6)] compared with patients admitted for an exacerbation of the disease [PUCAI 72 (SD 11.9)]. Of the 51 patients admitted with an exacerbation of previously diagnosed ulcerative colitis [median disease duration 14 months (IQR 8–26)], 37 (67%) were treated with oral prednisone prior to admission [median therapy duration 14 days (IQR 8–35)].
Incidence analyses
The subset of 55 children aged less than 15 years and with postal codes indicating residence in the GTA comprised 28% (95% CI, 23 to 34%) of GTA children under follow-up care for ulcerative colitis through the SickKids IBD programme during that period. The average population of the GTA between 1991 and 1996 was 4 071 888, including 819 533 children aged less than 15 years. The population-based incidence of children admitted at least once for a severe exacerbation of ulcerative colitis was 1 per 100 000 children per year, and the burden of overall admissions for steroid therapy (including repeated admissions of the same patient) was 1.6 admissions per 100 000 children per year.
Outcomes with intravenous corticosteroid treatment
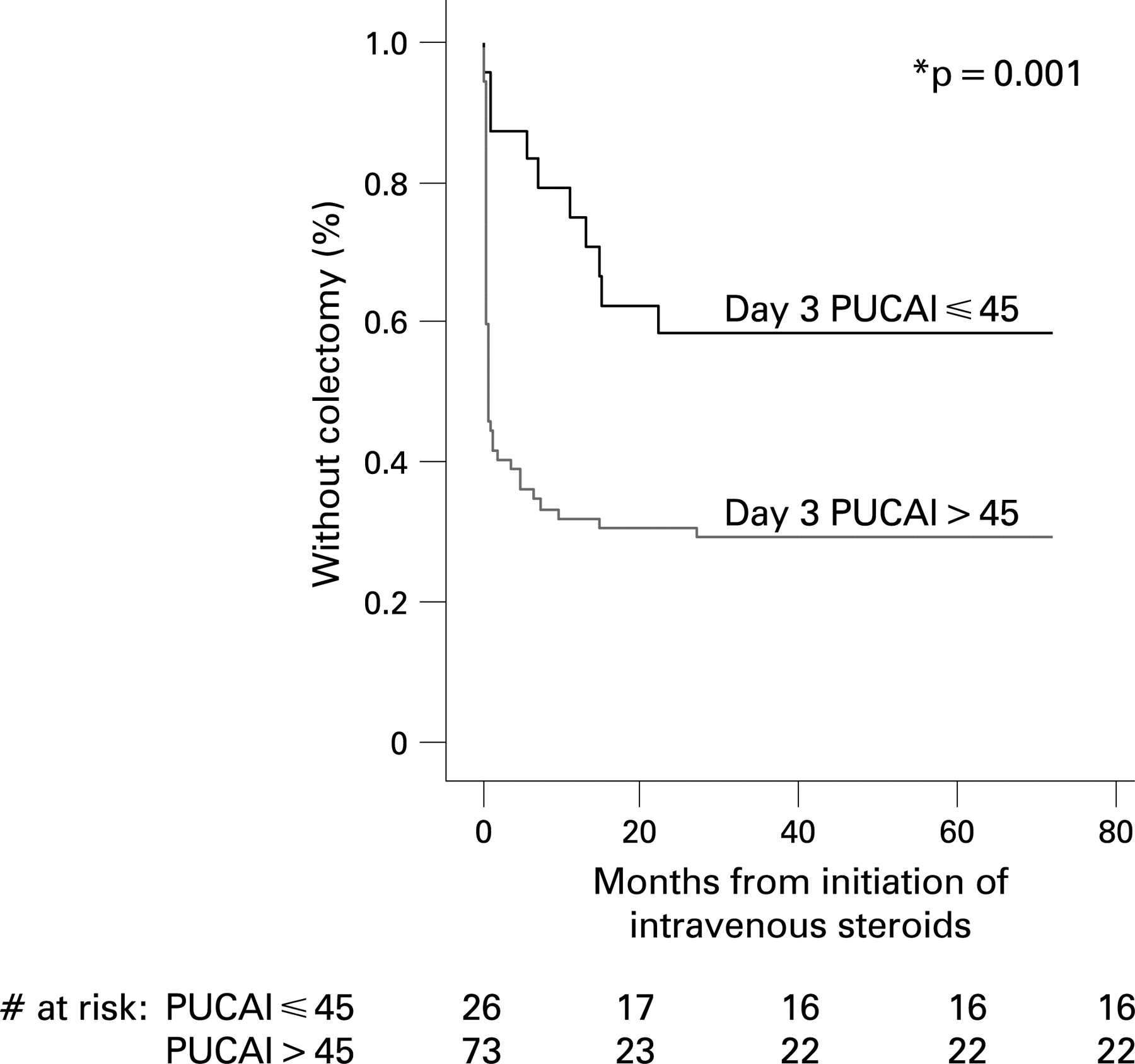
Short-term and longer-term outcomes are depicted in fig 1. Fifty-three children [53% (95% CI, 44 to 63%)] responded to intravenous corticosteroid therapy and were discharged after a median hospital stay of 10 days (IQR 7.5–14). Response rates were not different amongst new-onset ulcerative colitis patients versus those with disease in relapse (χ2, p = 0.4; table 1). The proportion of patients who responded to corticosteroids in a subgroup analysis of the 55 younger patients who resided within the GTA was identical to the full cohort [53% (95% CI, 41 to 68%)], suggesting no referral bias. Only one patient (1%) was diagnosed with toxic megacolon using standard criteria,21 and underwent colectomy 6 days following admission. Forty-six patients (46%) failed corticosteroid therapy and were treated with second-line drugs (one ciclosporine, five tacrolimus) and/or colectomy (n = 40; fig 1). Four of the six patients treated with calcineurin inhibitors, responded and were discharged without colectomy.

Twenty-two of the total 57 children, who were discharged without colectomy proved steroid dependent during the subsequent year (22% of the full cohort) (fig 1); azathioprine was initiated in 13. One year after discharge, 16 additional patients (including one tacrolimus short-term responder) required colectomy, bringing the 1-year colectomy rate to 58% (95% CI, 49 to 68%). In the total follow-up period following discharge [6 (SD 3.6) years], cumulative colectomy rate was 61% (95% CI, 52 to 71%), with only three additional patients requiring colectomy subsequent to the 1-year mark. Eighty-one children (81%) were followed until transfer to adult care at the age of 18 years.
Predictors of outcome
The following variables at both days 3 and 5 of intravenous corticosteroids were significantly associated with short-term steroid failure using univariate analysis (tables 1, 2 and 3): number of nocturnal stools, number of stools per 24 h, amount of blood in the stool, albumin, CRP, ESR and weight loss prior to admission. All 14 patients who had more than two nocturnal stools at the third day of steroid therapy (100%) and 12 of 13 patients at the fifth day (92%) required second-line therapy prior to hospital discharge (p<0.001). Similarly, 25 of the 27 patients with no nocturnal stools at day 3 (93%) and 23 of 27 at day 5 (85%) recovered without additional therapy (p<0.001). In a multivariate logistic regression, only the number of nocturnal stools and CRP (mg/dl) remained significant both at day 3 [OR 3.2 (95% CI, 1.6 to 6.6), p = 0.002 for nocturnal stools; and OR 2.4 (95% CI, 1.01 to 5.8), p = 0.049 for CRP]; and at day 5 [OR 2.8 (95% CI, 1.4 to 5.8), p = 0.003 for nocturnal stools; and OR 3.5 (95% CI, 1.4 to 8.4), p = 0.006, for CRP].
The third day of corticosteroid therapy may serve as a screening day to identify non-responders;9 10 hence, high sensitivity is desired to prepare selected patients for second-line therapies. By the fifth day, second-line therapy may be executed and, thus, high specificity is required. Cut-offs were chosen to follow this rationale (table 4), except for the Travis rule, which is designed as a fixed dichotomous rule at day 3. The prediction of colectomy by the PUCAI was significant not only by discharge, but also on long-term follow-up (fig 3).
All four evaluated indices (i.e. PUCAI, Lindgren, Seo, and Travis) significantly differentiated the responders from the non-responders at days 3 and 5 of therapy (tables 2 and 3). The cross-sectional scores of all indices had a better discriminative performance than their change over time (i.e. from baseline to day 3 or 5, and from day 3 to day 5). Receiver operating characteristic (ROC) curves of the indices were plotted (fig 2) to compare their overall discriminative performance. Since the Travis score is a categorical variable it could not be plotted with the others. There were no differences in the accuracy of the prediction rules before and after 1996, the year when the Travis rule was first published, suggesting that the decision to proceed to second-line therapy in our paediatric cohort was not confounded by the knowledge of the adult predictors.
Abdominal radiographs were performed in 46 children during the first 3 days of corticosteroid therapy. There were no radiographs with free air, pneumatosis intestinalis or portal venous air and only two with overt mucosal ulcers. There was a good agreement between the two blinded radiologists for transverse colon width [ICC 0.85 (95% CI, 0.72 to 0.92)], small bowel width [ICC 0.76 (0.57–0.87)] and number of air-fluid levels [ICC 0.90 (0.81–0.94)], but only fair agreement for abnormally thickened haustra (kappa 0.42; p = 0.004). The mean of the two evaluations was used for further analyses. The distribution of colon luminal width of children older than 11 years of age was similar to data previously published in adults,22 23 with width of up to 60 mm [mean 36 (SD 19) mm] evidence in the absence of clinical and laboratory criteria of toxic megacolon (fig 4A). In contrast, the upper width range in younger children was 40 mm [27 (SD 11) mm; p = 0.039, Student t test, compared with older children). None of the radiographic variables were associated with response to corticosteroid therapy, including bowel width (fig 4B), number of air-fluid levels (p = 0.58; Wilcoxon rank sum test), and thickened haustra (p = 0.39; χ2 test).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
We have presented novel data concerning the prevalence of acute severe exacerbations in children with ulcerative colitis, and have examined response and predictors of response to conventional corticosteroid treatment in a sizeable paediatric cohort. Several studies have documented a greater prevalence of extensive colitis in paediatric-onset ulcerative colitis4 6 compared to adults, of whom only one-third are reported to have macroscopic disease proximal to the splenic flexure.5 Exacerbations requiring hospitalisation, therefore, might be expected to occur more frequently in children, but this burden of illness among paediatric patients has not been previously assessed. It is generally accepted that the lifetime risk of acute severe ulcerative colitis among adult patients is approximately 15%.24–26 As hypothesised, we have documented a greater likelihood of hospitalisation for treatment of acute disease in our paediatric population-based cohort.
Equally surprising is the extreme paucity of previously published data concerning corticosteroid response rates among children with acute severe ulcerative colitis. A previous meta-regression reported a weighted short-term colectomy rate of 29% in pooled data concerning 1991 patients hospitalised with acute ulcerative colitis.3 Only three previous small studies, however, evaluated the outcome of admissions for severe paediatric ulcerative colitis. One (n = 11) reported a lower rate of colectomy than in adults (10%); the other two (n = 13 and n = 20) reported higher rates (45%, 46%).18 27 28 Our 46% steroid-refractory rate, in a much larger cohort, confirms that response to intravenous steroids may be poorer in children than in adults. Similar to recent outcome studies of paediatric ulcerative colitis treated with corticosteroids (mostly ambulatory), we observed a high proportion of steroid dependency during 1-year follow-up.29 30 The poorer response of children compared with adults may be explained at least in part by the higher proportion of extensive colitis in childhood onset ulcerative colitis. Disease extent has been consistently associated with severe disease course.2 31–34 Interestingly, our colectomy rate after 1 year remained remarkably stable, supporting data from a population-based study that documented most of the ulcerative colitis-related admissions during the first few years of diagnosis.35
Among this patient cohort, response did not vary with corticosteroid dosage in the range administered. This confirms our heterogeneity-controlled meta-analysis that found virtually no correlation between steroid dose (at or above equivalent of 60 mg methylprednisolone daily in adults), and the proportion of patients failing therapy.3 Moreover, clinical trials that assessed continuous versus bolus36 or pulse dosing37 of intravenous steroids in ulcerative colitis failed to identify differences in response. Similarly, in ambulatory adult patients with moderate exacerbations of ulcerative colitis, 40 mg of prednisolone was as effective as 60 mg daily with less toxicity,38 and once daily was as effective as multiple daily doses.39 More research is required to unravel the mechanisms of corticosteroid resistance, as bioavailability of corticosteroid does not seem to play an important role.40
Untreated severe ulcerative colitis attacks in adults were previously associated with a 24% mortality rate,1 41 but timely introduction of medical therapy reduced this rate to 1%.3 Although some case series suggest that prolongation of steroid therapy (i.e. beyond 2 weeks) is effective in eventually achieving remission, this approach is associated with increased toxicity, discomfort and cost.28 42 Adult clinical guidelines, therefore, recommend that second-line therapy be initiated if no response to corticosteroids is noted within several days of initiating intravenous therapy.8 18 34 41 43 44
To give clearer direction concerning implementation of second-line therapy, adult investigators have developed measures predictive of steroid failure.7–10 In a prospective analysis by Travis et al, stool frequency of >8/day or 3–8/day and C-reactive protein (CRP) >45 mg/l on the third day of therapy had a PPV of 85% for colectomy.9 Lindgren et al10 45 developed the fulminant colitis index (stool frequency/day+0.14×CRP mg/l) with a PPV of ∼70% at a cut-off score of >8 at day 3 of therapy. Ho et al developed an index based on stool frequency, albumin level and colonic dilatation.8 Ours is the first study to compare these predictive tools head-to-head. We selected low cut-offs of the prediction rules at day 3 (i.e. high sensitivity), to identify patients to be prepared for second-line therapy (e.g. for treatment suitability for infliximab, calcineurin inhibitors, and/or surgical consult), and higher cut-offs (i.e. high specificity) on day 5 to guide execution of the planned therapy in the 40–50% of patients in whom the risk for colectomy is >90%. This approach should guide appropriate escalation of therapy earlier in the disease course and shorten the overall hospital stay. The subset of patients not fulfilling these conservative cut-offs may be treated for several more days with continued corticosteroids. We examined the predictive ability of the PUCAI developed originally as an evaluative and discriminative tool.6 The novel data from the present retrospective analysis suggest that a PUCAI score of >45 on day 3 should dictate planning of second-line therapy and PUCAI >70 on day 5, should prompt the execution of the planned therapy.
This study provides the first descriptive data concerning abdominal x rays in children with severe ulcerative colitis but who do not fulfil the clinical criteria for toxic megacolon.21 The distribution of colonic luminal width in children above 11 years of age follows the published data from adults, in whom a width of up to 60 mm may occur without clinical or laboratory criteria for toxic megacolon.22 23 46 In contrast, colon dilatation of more than 35–40 mm was unusual in younger children. Unlike adult studies,8 31 32 47–50 we found no associations between radiographic appearances and outcome. Adolescents (>11 years of age) with a transverse colon luminal width of 40–60 mm were still very likely to respond to therapy.
Childhood-onset extensive ulcerative colitis is an IBD phenotype associated with significant morbidity. This study, although retrospective, has highlighted the short-term response rates and longer term outcomes in an otherwise understudied group of patients. The population-based sub-analyses reduced the risk of referral bias. Documentation of steroid response rates and predictors of response in children are important, so that much-needed novel therapies may be tested in appropriate patients. We have generated data concerning the predictive value of the PUCAI and other predictive measures, when employed in children. Cut-off scores suggested by this study will be re-examined in an ongoing prospective multicentre study of severe paediatric ulcerative colitis, wherein additional serological and genetic factors associated with acuity and response to treatment, will also be assessed.
REFERENCES
Footnotes
Competing interests: None.
Linked Articles
- Digest