Article Text

Abstract
Background: The true treatment rate for hepatitis C virus (HCV) in veterans is unknown.
Aim: To determine the treatment prescription rates and predictors of treatment prescription for HCV in a large national population.
Methods: The Department of Veterans Affairs National Patient Care Database (NPCD) was used to identify all HCV-infected people between the fiscal years 1999 and 2003 using the International classification of diseases, 9th revision codes. Demographic information, medical and psychiatric comorbidities, and drug and alcohol use diagnoses were retrieved. Pharmacy data were retrieved from the Department of Veterans Affairs Pharmacy Benefits Management (PBM) database. Logistic regression analysis was used to determine the predictors of treatment for HCV in HCV.
Results: 113 927 veterans in the Department of Veterans Affairs care with a diagnosis of HCV were identified. The treatment prescription rate for HCV was 11.8%. Patients not prescribed treatment were older, more likely to be from minority races, have more alcohol and drug misuse, and have medical and psychiatric comorbid conditions. In a multivariate logistic regression model, the following factors were predictive of non-treatment for HCV: increasing age (odds ratio (OR) 0.77 for each 5-year increase in age; 95% confidence interval (CI) 0.76 to 0.78); black race (OR 0.64; 95% CI 0.6 to 0.68); Hispanic race (OR 0.88; 95% CI 0.8 to 0.96); alcohol abuse and dependence (OR 0.62; 95% CI 0.59 to 0.65); drug abuse and dependence (OR 0.78; 95% CI 0.74 to 0.82); anaemia (OR 0.18; 95% CI 0.16 to 0.21); hepatitis B infection (OR 0.72; 95% CI 0.62 to 0.83); coronary artery disease (OR 0.9; 95% CI 0.85 to 0.97); stroke (OR 0.75; 95% CI 0.67 to 0.85); bipolar disorder (OR 0.64; 95% CI 0.58 to 0.70); major depression (OR 0.72; 95% CI 0.67 to 0.77); mild depression (OR 0.56; 95% CI 0.53 to 0.59); and schizophrenia (OR 0.71; 95% CI 0.65 to 0.77). The following factors were associated with a higher likelihood of treatment prescription for HCV: liver cirrhosis (OR 1.6; 95% CI 1.5 to 1.7); and diabetes (OR 1.07; 95% CI 1.02 to 1.12).
Conclusions: A small number of HCV-infected veterans were prescribed treatment for HCV. Non-treatment is associated with increasing age, non-white race, drug and alcohol abuse, and dependence and comorbid illnesses. Reasons for non-treatment need further study.
- HCV, hepatitis C virus
- ICD-9, International classification of diseases, 9th revision
- NPCD, National Patient Care Database
- PBM, Pharmacy Benefits Management
Statistics from Altmetric.com
- HCV, hepatitis C virus
- ICD-9, International classification of diseases, 9th revision
- NPCD, National Patient Care Database
- PBM, Pharmacy Benefits Management
Hepatitis C virus (HCV) infects >1.8% of the US population and more than 170 million people are infected worldwide. The disease course is highly variable, but up to 30% of infected individuals will develop cirrhosis after 20–30 years of chronic infection.1,2 HCV is a major cause of end-stage liver disease and hepatocellular carcinoma.3,4 It is also the leading reason for liver transplantation in the US.
Treatments for HCV that result in sustained elimination of viral replication are now available. The standard of care when treatment for HCV is indicated is a combination of interferon α (pegylated and non-pegylated) and ribavirin. This combination is effective in achieving long-term viral eradication in 54–56% of HCV-infected people overall. The response rate for HCV genotype 1 is about 40%, whereas it approaches 80% for genotype 2 or 3 infection.5,6,7,8,9,10,11 Response rates are reported to be lower in HIV-coinfected people and in blacks.12,13
Even with major advances in treatment for HCV, treatment is prescribed in only a minority of HCV-infected people. Most published guidelines recommend treatment only for patients at risk of or with severe disease progression, who are likely to abstain from alcohol, and who can tolerate the common side effects associated with treatment.14–16 Studies at tertiary referral centres have demonstrated that only a minority of referred patients are recommended treatment, and most patients are not treated for HCV.17,18 Non-adherence, hazardous alcohol consumption, and presence of medical and psychiatric comorbidities are the major reasons for not prescribing treatment in HCV-infected people.17,18 Treatment prescription rates have not been determined in larger HCV-infected populations, and the predictors of treatment remain largely unknown. We undertook this study to determine the rates of HCV treatment prescription in US veterans in care who were diagnosed with HCV, and to determine the role of demographic characteristic and medical and psychiatric comorbidity on the rates of treatment.
METHODS
A cohort of HCV-infected patients was assembled from the Department of Veterans Affairs National Patient Care Database (NPCD) and the Department of Veterans Affairs Pharmacy Benefits Management (PBM) data. The assembly of this cohort has also been described in a recent publication.19 The utility and accuracy of the Department of Veterans Affairs administrative and PBM data have been previously reported by our group and by others.19–25 The NPCD contains hospitalisation records, including discharge diagnoses from 1970 onwards. The discharge diagnoses are coded according to the clinical modification of International classification of diseases, 9th revision (ICD-9). From 1997 onwards, the NPCD also contains outpatient visit records, including diagnoses and clinic visits. The PBM database contains records of all drugs prescribed to veterans by any of the Department of Veterans Affairs pharmacies, including the dose and amount prescribed. The ICD codes for diagnoses of HCV, HIV and other medical, psychiatric and substance abuse have been tested and validated in the Department of Veterans Affairs healthcare system.20,23,26
Patients were considered to be infected with HCV if they had one inpatient or two outpatient ICD-9 codes for HCV on two separate visits. We identified all veterans who were seen in the Department of Veterans Affairs healthcare system who met this definition between the fiscal years 1999 and 2003. Each patient was counted only once for the Department of Veterans Affairs fiscal year in which they were first diagnosed. We retrieved demographic information including date of birth, recorded race and sex, and information on medical and psychiatric comorbidities, and drug and alcohol abuse and dependence. Medical and psychiatric comorbidities were also retrieved using ICD-9 codes, and patients were considered to have a comorbid condition if at least one inpatient or two outpatient codes were identified. Data retrieved from the PBM included prescriptions of interferon α, pegylated interferon α, ribavirin and combinations of either type of interferon with ribavirin. Dates of prescription and cumulative duration of prescription were obtained. The doses of interferon generally used in the treatment of HCV were retrieved, and high-dose interferon α treatment (>5 million units per dose given ⩾3 times per week) was excluded, as such higher doses of interferon are not the standard doses used to treat HCV infection. Patients with a diagnosis of HIV infection were also excluded.
Prescription for HCV was defined as having received interferon α, pegylated interferon α or a combination of either with ribavirin for any duration of time. If a patient was prescribed multiple courses of treatment, only the first prescription was counted. Whether the patients actually took the treatment as prescribed was not ascertained. As depression and anaemia are well-known side effects of interferon and ribavirin treatment, respectively, we excluded the observations for these comorbidities if they were diagnosed any time after initiation of treatment for HCV.
Statistical analysis
We compared the veterans who received treatment for HCV with those who did not receive treatment. The demographic characteristics were compared using χ2 test or t test as appropriate. We used univariate and multivariate logistic regression analyses to determine the predictors of treatment for HCV in all identified patients. We used Stata V.8.2 for statistical analyses.
RESULTS
Using the above definitions, we identified 113 927 patients with HCV who received care in any of the Department of Veterans Affairs facilities between the fiscal years 1999 and 2003. The median age was 50 years (mean 51.1 years); 96.9% were male; 40.1% were white, 22% were black and 5.2% were Hispanic (table 1). In all, 44.3% of the patients had a diagnosis of alcohol abuse or dependence, and 40% had a diagnosis of drug abuse or dependence. The rates of medical and psychiatric comorbidities were as follows: anaemia 11.7%; hepatitis B 3%; diabetes 20.5%; coronary artery disease 13.5%; stroke 4.7%; pulmonary disorders (chronic obstructive disease and asthma) 19.3%; bipolar disorder 10.4%; major depression 18.4%; mild depression 32.4%; schizophrenia 9.5%; and post-traumatic stress disorder 19.7%. Cirrhosis was diagnosed in 10.4% of the patients, and 11.8% of the patients received treatment for HCV (table 1).
Demographic characteristics and comorbidities in hepatitis C virus-infected veterans
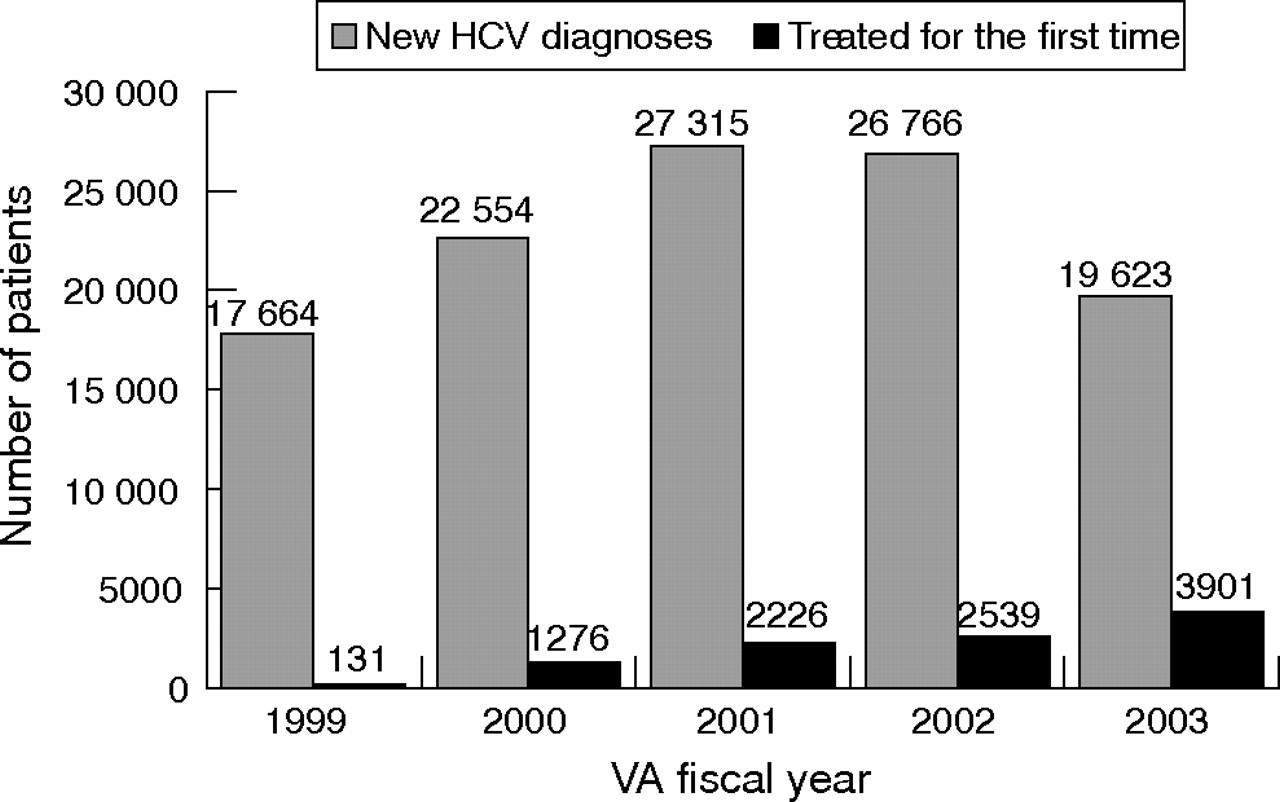
The number of newly diagnosed cases increased from 1999 to 2001, after which there was a decline in their number. The largest number of newly diagnosed cases was in 2001, when 27 315 new diagnoses of HCV were recorded. Treatment prescription for unique HCV-infected patients increased throughout 1999–2003. The highest number was recorded in 2003 (3901 unique patients treated for the first time) and the lowest in 1999 (131 unique patients treated; fig 1).
{kind=link}
Number of new diagnoses of hepatitis C virus (HCV) and number of unique patients treated for the first time in the given fiscal year. The diagnosis of HCV is incident for the Department of Veterans Affairs (VA) fiscal year in which it was first diagnosed. Treatment prescription is incident for the VA fiscal year in which it was first prescribed.
Table 2 shows a comparison of treated and untreated patients. In all, 10 077 patients were prescribed treatment and 103 850 patients were not prescribed treatment for HCV. Treated patients were younger, less likely to be of black race, less likely to have a diagnosis of alcohol or drug abuse or dependence, and less likely to have anaemia, hepatitis B virus infection, diabetes, coronary artery disease, stroke, pulmonary disease, bipolar disorder, major depression, mild depression, schizophrenia and post-traumatic stress disorder (all comparisons, p<0.001). Treated patients were more likely to have a diagnosis of cirrhosis and to have had a liver biopsy.
Comparison of veterans prescribed treatment for hepatitis C virus with those not prescribed treatment
In a multivariate logistic regression model, the following factors were predictive of non-treatment for HCV: increasing age, black or Hispanic race, alcohol abuse or dependence, drug abuse or dependence, anaemia; hepatitis B infection, coronary artery disease, stroke, bipolar disorder, major depression, mild depression, and schizophrenia. Liver cirrhosis and diabetes were associated with a higher likelihood of treatment prescription for HCV (table 3).
Factors predicting prescription for hepatitis C virus treatment (logistic regression analyses)
DISCUSSION
The rate of pharmacotherapy for HCV in veterans was previously unknown. We found that 11.8% of HCV-infected veterans receiving care at Department of Veterans Affairs facilities were treated for HCV infection between the fiscal years 1999 and 2003. To our knowledge, this is the largest study of this nature, and we studied all people identified in the Department of Veterans Affairs system, rather than a geographically localised or convenience sample. Our results, from among unselected veterans diagnosed with HCV, are consistent with other smaller studies conducted in referral clinics, although the treatment rate in our study was about one third of that found in selected subpopulations of HCV-infected individuals referred to specialty clinics.17,18
However, these data need to be interpreted with caution. Our study does not take into account the eligibility for treatment for HCV infection. Indeed, about 15–25% of HCV-infected people clear the viraemia spontaneously and are not candidates for treatment. Others have minimal evidence of liver disease from HCV and may reasonably decide to forgo or defer treatment.
However, other patients fall outside the recommendations of published guidelines owing to ongoing disorders or other comorbid conditions from substance misuse. Some veterans in our cohort may have received treatment at non-Department of Veterans Affairs facilities but were classified as not treated in our study. However, considering the cost of treatment, and the fact that treatment in the Department of Veterans Affairs is available to the veterans regardless of their ability to pay, it is unlikely that a large number of veterans would have received treatment outside the Department of Veterans Affairs system.
Treated patients were younger and more likely to be white. Racial disparities in prescription and utilisation of clinical care have been reported in veterans and non-veterans for various medical and surgical conditions.27–30 Conversely, most studies suggest that black race is associated with a poorer response to treatment for HCV, which may affect patients’ and providers’ decisions regarding treatment for HCV.13,31 Whether this is the reason in veterans has not been studied.
Patients with medical and psychiatric comorbidities (for example, anaemia, hepatitis B coinfection, coronary artery disease, stroke, diabetes, pulmonary disease, bipolar disorder, major or mild depression, and schizophrenia) were less likely to have received treatment for HCV. Ribavirin is associated with a dose-dependent haemolytic anaemia, and in patients with pre-existing anaemia or coronary artery disease, providers may be hesitant to prescribe treatment that may exacerbate the condition or precipitate complications. Whether anaemia in our patients was a direct consequence of HCV treatment is not known. Depression is a well-known side effect of interferon treatment, which may precipitate new-onset depression or exacerbate pre-existing depression, and is a major concern when making treatment decisions for HCV-infected people. We excluded anaemia and depression if they were first diagnosed after initiating treatment for HCV to remove the confounding of treatment-induced anaemia and depression.
In the logistic regression model, increasing age, minority race, drug and alcohol abuse and dependence, anaemia, hepatitis B, coronary artery disease, stroke, bipolar disorder, major and mild depression, and schizophrenia were associated with a lower likelihood of HCV treatment prescription. Active drug and alcohol abuse are relative contraindications to treatment for HCV, and the high rate of these may have contributed to overall low rates of treatment prescription in our study. Age, race, mild depression and schizophrenia are not absolute contraindications to treatment fpr HCV, even though the response rates may be lower in some groups—for example, black people with chronic HCV infection. Patients with cirrhosis were more likely to be prescribed treatment, which may reflect relatively advanced disease in these people. Decompensated cirrhosis is a contraindication to treatment. However, we could not assess whether the patients with cirrhosis in our study had stable or decompensated cirrhosis.
Liver biopsy is recommended to assess the degree of liver disease and to make treatment decisions. In our study, a minority of untreated patients underwent liver biopsy. This suggests that the decision not to treat was based on criteria other than liver biopsy in most patients. Whether non-invasive markers were used to assess liver injury or whether these patients have other contraindications to biopsy or treatment is not known.
The number of new diagnoses of HCV increased between 1999 and 2001. This is probably a reflection of the effort by the Department of Veterans Affairs in raising awareness and increasing testing among the veterans. In 2002–3, this number dropped, which may indicate “testing fatigue” by the providers or that most infected people had already been diagnosed. The number of treated people increased throughout 1999–2003. This is probably attributable to increased awareness and designation of HCV as a national priority by the Department of Veterans Affairs, as well as to increasing confidence of the providers with more data now available regarding efficacy of treatment and associated side effects. Availability of pegylated interferons and the associated ease of administration compared with the older standard interferon may also have led to the increasing number of infected veteran being treated.
Certain limitations to this study must be taken into account when interpreting the results. These include an analysis of administrative databases and the fact that patients were identified using ICD-9 codes. However, the accuracy of the ICD-9 codes has been tested in the Department of Veterans Affairs healthcare system. Diagnostic code agreement and κ values for HCV were validated in the Veterans Aging Cohort Study 3.20 Compared with the HCV antibody test, the sensitivity and specificity of the codes were 74% and 98%, respectively, and positive and negative predictive values were 96% and 84%, respectively. The agreement in these readings was 88% and the κ value was 0.74. Kramer et al23 also reported the positive predictive value of the ICD-9 diagnosis to be 94% and the negative predictive value to be 90%. In the Veterans Aging Cohort Study 3, 880 of the 881 participants were correctly identified as having HIV when compared with chart abstractions and antibody test, providing a high level of sensitivity. Other ICD-9 codes have also been validated against chart reviews. For example, the sensitivity, specificity, agreement and κ values have been reported as follows:
-
alcohol abuse and dependence: sensitivity 68.7%; specificity 92.9%; agreement 85.1%; κ = 0.64.
-
drug abuse and dependence: sensitivity 68.7%; specificity 92.9%; agreement 85.1%; κ = 0.64.
-
depression: sensitivity 44.8%; specificity 90%; agreement 68%; κ = 0.35.
-
diabetes: sensitivity 64%; specificity 99.2%; agreement 95.8%; κ = 0.72.26
We did not determine how many untreated people were actually eligible for treatment. Treatment prescription was determined from pharmacy records, and whether the patients actually took any of the drugs prescribed is unknown. Additionally, some patients may have received treatment outside a Department of Veterans Affairs facility and would have been missed in our counts.
Designation of race is problematic in the Department of Veterans Affairs administrative data, with different methods used at local sites to determine the race, including patient report and observer determination by the person registering the patient at the local Department of Veterans Affairs facility. This may lead to different racial categories entered on different visits. Such discrepancies may have contributed to a large number of unknown/other racial categories in our study.
Despite these limitations, our study has considerable strengths. This report provides the first robust estimates of treatment rates for HCV in a broad, non-selected clinical population. Although rates of treatment are available from clinical trials or specialty referral clinics, those studies are generally geographically limited or represent highly selected patients. Thus, those estimates are not applicable to general patient populations with HCV. Our data represent national rates for a large cohort of US veterans. Although we cannot determine the reasons for non-treatment, this does provide a good estimate of actual treatment rates and should serve as a reference for other large integrated healthcare groups. Reasons for non-treatment in veterans and non-veterans need further study to determine whether there are any modifiable factors associated with non-treatment for HCV, and whether treating those people would favourably alter outcomes.
In conclusion, a small number of HCV-infected veterans are prescribed treatment for HCV. Non-treatment is associated with increasing age, minority race, drug and alcohol use, and medical and psychiatric comorbid illnesses. Reasons that affect patients’ and providers’ decisions regarding treatment for HCV require further study.
REFERENCES
Footnotes
-
Published Online First 27 September 2006
-
Funding: This study was funded by National Institutes of Health/National Institute on Drug Abuse (DA016175-01A1, AAB).
-
Competing interests: None.