Article Text

Abstract
Background and aims: Both environmental and genetic factors may contribute to irritable bowel syndrome (IBS). Nutrition in fetal life, an early environmental factor, seems to influence the development of chronic diseases later in life, such as coronary heart disease, hypertension, and non-insulin diabetes. This population based twin study evaluated the association between intrauterine growth, measured by weight and gestational age, and IBS. Structural equation analyses were conducted to analyse genetic and environmental sources of variation in liability to IBS.
Methods: A postal questionnaire was sent to 12 700 Norwegian twins born between 1967 and 1979. The questionnaire included a checklist of 31 illnesses and symptoms, including IBS. The influence of birth weight on developing IBS was tested in four weight groups. Disease discordant monozygotic (MZ) pairs were analysed to test the association between intrauterine growth and IBS.
Results: Concordance for IBS was significantly greater (p = 0.011) in monozygotic (22.4%) than in dizygotic (9.1%) twins. The heritability of IBS was estimated to be 48.4% among females. Birth weight below 1500 g (adjusted odds ratio 2.4 (95% confidence interval 1.1, 5.3)) contributed significantly to the development of IBS, which appeared 7.7 years earlier than in higher weight groups. In the MZ group with birth weights lower than 2500 g, twins with IBS were significantly lighter than twins without disease (190.6 g; p = 0.02).
Conclusion: The present study demonstrates that restricted fetal growth has a significant influence on the development of IBS later in life. Weight below 1500 g influences age at onset. Genetic contribution appears to be important for IBS among females.
- DZ, dizygotic
- DZF, dizygotic female
- DZL, dizygotic-like pairs
- DZM, dizygotic male
- DZU, dizygotic unlike pairs
- IBD, inflammatory bowel disease
- IBS, irritable bowel syndrome
- LRT, likelihood ratio test
- MMC, motor migrating complex
- MZ, monozygotic
- MZF, monozygotic female
- MZM, monozygotic male
- SEM, structural equation modelling
- OR, odds ratio
- twins
- population based
- restricted birth weight
- genetic factors
- irritable bowel syndrome
Statistics from Altmetric.com
- DZ, dizygotic
- DZF, dizygotic female
- DZL, dizygotic-like pairs
- DZM, dizygotic male
- DZU, dizygotic unlike pairs
- IBD, inflammatory bowel disease
- IBS, irritable bowel syndrome
- LRT, likelihood ratio test
- MMC, motor migrating complex
- MZ, monozygotic
- MZF, monozygotic female
- MZM, monozygotic male
- SEM, structural equation modelling
- OR, odds ratio
Irritable bowel syndrome (IBS) is an example of a functional gastrointestinal disorder. The aetiology of IBS is believed to be multifactorial. Many pathophysiological mechanisms have been proposed, including abnormal motility and visceral hypersensitivity.1,2 IBS is characterised by abdominal pain, bloating, and disturbed defecation with no identifiable structural cause. The prevalence of IBS in highly industrialised countries ranges from 5% to 20%, and is more prevalent among women.3
The effect of an early environmental factor, nutrition in fetal life, has been analysed in several twin studies. Convincing evidence exists to suggest that restricted development of specific fetal organs could predispose to chronic disease such as cardiovascular heart disease, non-insulin diabetes, and hypertension4–6 later in life. Fetal development consists of critical periods for development of organ systems. Barker’s hypothesis,7 the fetal programming hypothesis, proposes that lack of nutrition and oxygen supply can lead to compromised growth that may permanently affect the structure and function of physiological systems.
Twin studies are particularly useful for further resolution of these putative influences because they offer a methodology for distinguishing and estimating genetic and environmental influences on fetal development. Identical twins differ in birth weight due to unequal distribution of nutrition and blood supply between the twins in utero. By using identical twins discordant for disease, we control for genetic effects and shared environmental factors after birth. Genetic and psychological mechanisms have been hypothesised to explain familial clustering of IBS. Some twin studies,8,9,10 but not all,11 support a genetic influence on the development of IBS.
The purpose of the present population based twin study was to explore the influence of restricted intrauterine growth, by use of birth weight, and genes on the development of IBS.
MATERIALS AND METHODS
Data are based on a population sample of twins identified from the Norwegian national birth registry, which was established in 1967. In a research programme at the Institute of Public Health,12,13 15 374 twins were born during the period 1967–1979. Postal questionnaires were sent in 1992 to twins born between 1967 and 1974, and in 1998 to twins born between 1967 and 1979. Data presented here are based on the 1998 questionnaire, which was sent to 12 700 twins where both twins were still alive with addresses in Norway and had indicated previously that they would like to participate in research (twins born 1967–75) or were newly recruited (twins born 1975–1979). Responses were received from 8045 twins (63%) and the sample included 3334 complete pairs and 1377 single responders. The questionnaire included a checklist for 31 illnesses and symptoms, including a question asking: Do you have, or have you ever had, irritable bowel syndrome (diarrhoea, constipation, and painful abdominal distension). Two other questions on gastrointestinal diseases were asked: one question with symptoms consistent with dyspepsia, where we used the phrase, recurrent upper abdominal pain, and another concerning inflammatory bowel disease (IBD), where we used the terms Crohn’s disease and ulcerative colitis. A diagnosis of IBD was confirmed by addressing the patient’s doctor. Age at onset was asked, and if symptoms were not currently present, the subject was asked to record the time of the last event. Consequently, all answers had to be given as yes or no. Age at onset and cessation of symptoms were coded as continuous variables.
Data on birth weight and gestational age were obtained from the Medical Birth Registry of Norway. Classification of zygosity was based on responses to seven questionnaire items, which have been verified in a previous study of Norwegian twins to correctly categorise zygosity with 97% accuracy.14
Of 3334 twin pairs, 138 pairs were excluded due to incomplete data. The final sample included 504 male monozygotic (MZM), 379 male dizygotic (DZM), 746 female monozygotic (MZF), 635 female dizygotic (DZF), and 932 dizygotic unlike pairs (DZU). Among these, there were 297 twin pairs for which at least one of the twins reported a positive history of IBS. This group consists of 20 MZM, 22 DZM, 77 MZF, 74 DZF, and 104 DZU pairs.
Analyses
Sex differences in the prevalence of IBS were tested using χ2 statistics. Concordance was estimated as the probandwise concordance rate defined as the ratio of twice the number of concordant pairs, divided by twice the number of concordant pairs plus the number of discordant pairs. Differences in concordance rates between MZ and DZ pairs were tested using χ2 statistics. Comorbidity of IBS with other chronic diseases was analysed in cross tabulations.
Twin studies
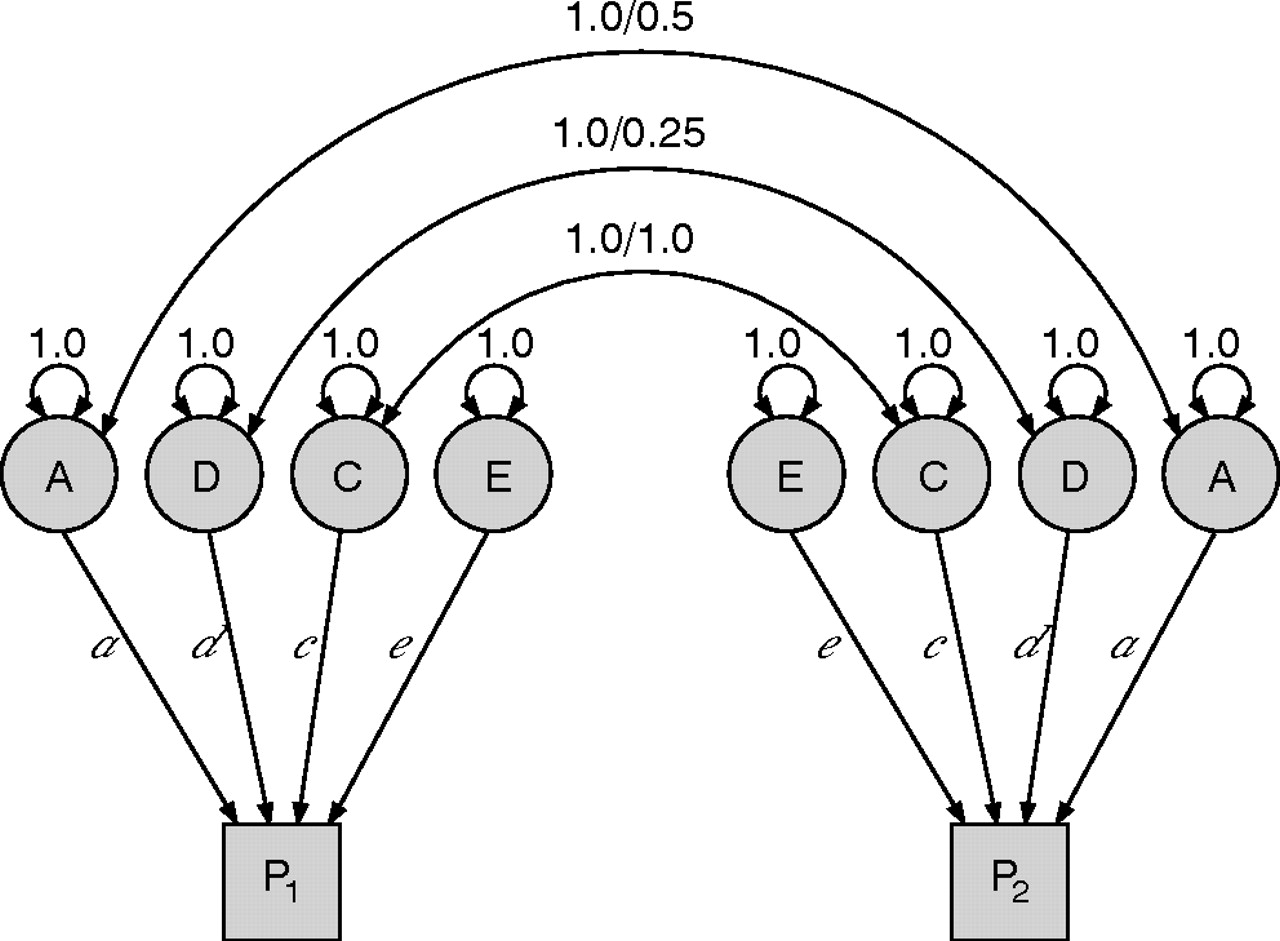
Within pair correlations measure twin resemblance, and the pattern of correlations across sex and zygosity groups provides insight regarding the importance of genetic and environmental influences. Monozygotic twins are genetically identical, while dizygotic twins share, on average, 50% of their segregating genes, in common with ordinary siblings. This information combined with the assumption that MZ and DZ pairs equally share environmental factors in common is utilised to resolve the phenotypic variance into genetic and environmental components. Genetic components may be further divided into additive (A, multiple small genetic) and dominant (D) genetic effects. Environmental components may also be separated into shared (C) and individual (E) environmental factors.15 Shared environment refers to environmental effects that are shared by twins and contribute to within pair similarity. In contrast, non-shared environmental effects are unique to each person and do not contribute to resemblance within the pair, also including measurement error.
Heritability
Heritability is defined as the proportion of the phenotypic variance among individuals in the population that is attributable to genetic differences.16 The within pair correlations provide a simple estimate of heritability through the formula 2× (MZcorr − DZcorr). Significantly greater MZ than DZ correlations yield a heritability estimate larger than zero, and suggest that genetic differences are important sources of variation. An MZ correlation greater than twice the DZ correlation suggests that dominance genetic factors (D) are present. This is because MZ twins are perfectly correlated for dominance effects, but pairs of DZ twins are, on average, correlated only 0.25 for these influences. An MZ correlation less than twice the DZ correlation suggests that common environment (C) is important.
Tetrachoric correlations, defined as the correlation in liability between members of twin pairs, were calculated. We used a liability threshold model15 which assumes that the underlying liability for the development of IBS is normally distributed. The liability threshold model also assumes equal thresholds within pairs and across zygosity. These assumptions were assessed using likelihood ratio tests (LRTs).17
Genetic modelling
Structural equation modelling (SEM) was used to resolve the correlations between members of twin pairs into genetic (A, D) and environmental (C, E) components. In the classical twin design, C and D are heavily confounded and are therefore estimated in separate models.
A series of models were analysed to test the significance of A, C, E, and D. This procedure compares the fits between the saturated models (ACE, ADE) and the reduced models (AE, CE) using LRTs. The purpose of the model fitting procedure is to explain the pattern of observed variance and covariance using as few parameters as possible. Recent work has shown that the LRT statistic, when testing one parameter in the SEM framework, is distributed as a 50/50 mix of χ2 distributions with one and zero degrees of freedom.18 Computation of intraclass correlations, testing of model assumptions, and variance components model fitting were conducted using the statistical modelling program Mx,19 and analysing raw ordinal data.
Birth weight analyses
Low birth weight was defined as less than 2500 g, and very low, below 1500 g. Birth weight was stratified into four weight classes (<1499, 1500–1999, 2000–2499, and >2500 g). Birth weight and gestational age are highly correlated, thus adjustments for gestational age were conducted. The relationship between these four weight classes and IBS, in the full sample, was studied by binary logistic regression. Crude and adjusted for gestational age odds ratios (ORs) and 95% confidence interval (CI) were calculated. Adjustment for the co-twin history of the same health problem was performed to control for common predisposing genetic factors. Tests were interpreted as significant at p<0.05. All p values were two sided.
Results from regression analyses were further explored by investigating mean birth weight difference between twins with and without IBS in the full sample when divided into four weight groups.
Age at onset of symptoms in the four weight classes was also compared. Mean duration of symptoms in twins who did not report current symptoms was estimated.
To control for genetic factors, which may contribute to both reduced birth weight and IBS, we performed a paired t test using only MZ pairs discordant for disease. In these analyses the data were split into two weight classes, below and above 2500 g, and differences in birth weight between twins with and without IBS were estimated.
This study was evaluated and approved by the Norwegian Scientific Ethics Committees and by the Norwegian Data Protection Agency.
RESULTS
The prevalence rate for IBS in the full sample was 5.4%. The lifetime prevalence of reported histories of IBS was 3% in males (n = 81) and 7.1% in females (n = 264). As reported in the modelling results below, these rates differ significantly. Mean age of onset of symptoms was 18 years for males and 17 years for females.
Of the 88.4% of twins with IBS answering the question concerning age at onset and cessation of symptoms, only 24.5% reported being free of symptoms at the present time. Mean duration of symptoms in this group was 4.7 (range 1–23) years. The majority (75.5%) reported ongoing IBS symptoms in the queries.
Concordance for IBS was significantly greater (χ2 = 12.9, p = 0.001) in monozygotic (22.4%) than in dizygotic (9.1%) twins. There was low comorbidity with the majority of other chronic diseases, except for dyspepsia, which showed an overlap of 21%. The typical chronic course of recurrent upper abdominal pain in dyspepsia was demonstrated. Seventy three per cent of twins who claimed to suffer from recurrent upper abdominal pain reported ongoing symptoms. Comorbidity was 3.5%, 1.7%, and 0.9% for IBD, rheumatoid arthritis, and ankylosing spondylitis, respectively.
Heritability
Values for the twin correlations (table 1) revealed that the MZ correlation was substantially higher than the DZL correlation, indicating that genetic effects play an important role in the liability for IBS. The DZL correlation was slightly above half the MZ correlation, suggesting that there may be some common environmental effect (C), but the broad confidence interval indicates a possible power problem. The DZU correlation was low compared with the DZL correlation, suggesting sex specific effects. DZM and DZF correlations were similar although the DZM estimate showed higher uncertainty, as reflected by the broader confidence interval due to the lower prevalence.
Prevalence, probandwise concordance, and intraclass correlations of irritable bowel syndrome stratified by zygosity, and by zygosity and sex of the pair
Stratification of the zygosity groups according to sex of the pair (five group analysis) revealed that none of the MZM pairs were concordant for IBS. Therefore, only females were considered in the variance component models.
Modelling results
Both ACE and ADE models (fig 1) were fitted, against which nested models were compared. These results are presented in table 2 and indicate that dominant genetic effects (D) do not account for any variation in liability for IBS, and could be removed from the model.
Genetics and environmental variance estimates and model fit statistics for irritable bowel syndrome

Classical twin model used in this study where the boxes indicate the measured phenotypes in twin 1 and twin 2, with the latent genetic and environmental parameters specified by circles. Genetic components are separated into additive (A) and dominance (D). Environmental components are separated into shared (C) and individual (E). The additive and dominance genetic correlations between monozygotic twins are 1. The additive and dominance genetic correlations between dizygotic twins are 0.5 and 0.25.
A model with no shared environmental effects (that is, fix c to zero to obtain an AE model) yielded a non-significant reduction in fit (p = 0.41) compared with the ACE model. A model with no additive genetic effects (that is, fix a to zero giving a CE model) also yielded a non-significant reduction in fit (p = 0.08) but the difference between the models were higher (Δχ2 = 1.94), suggesting the AE model fits better than the CE model. An AE model is consistent with the estimated high MZF correlation compared with the DZF correlation (table 1), suggesting the importance of genetic effects among females. An E only model (not included in table 2) was rejected (Δχ2 = 26.15, Δdf = 2; p<0.0001). The best fit model, an AE model, estimated the heritability of IBS to be 48.4% among females, and the remaining 51.6% attributable to non-shared environmental influences.
Contribution of low birth weight
The crude OR for IBS in weight class <1500 g was 1.9 (95% CI 0.98, 3.97), and was nearly significant (p = 0.058). When adjusted for gestational age, OR increased to 2.5 (95% CI 1.16, 5.5), and the influence of the lowest weight class on IBS increased and reached significance (p = 0.019). When adjusted for co-twin’s history of the same disease, OR remained nearly unchanged at 2.4 (95% CI 1.12, 5.3; p = 0.025).
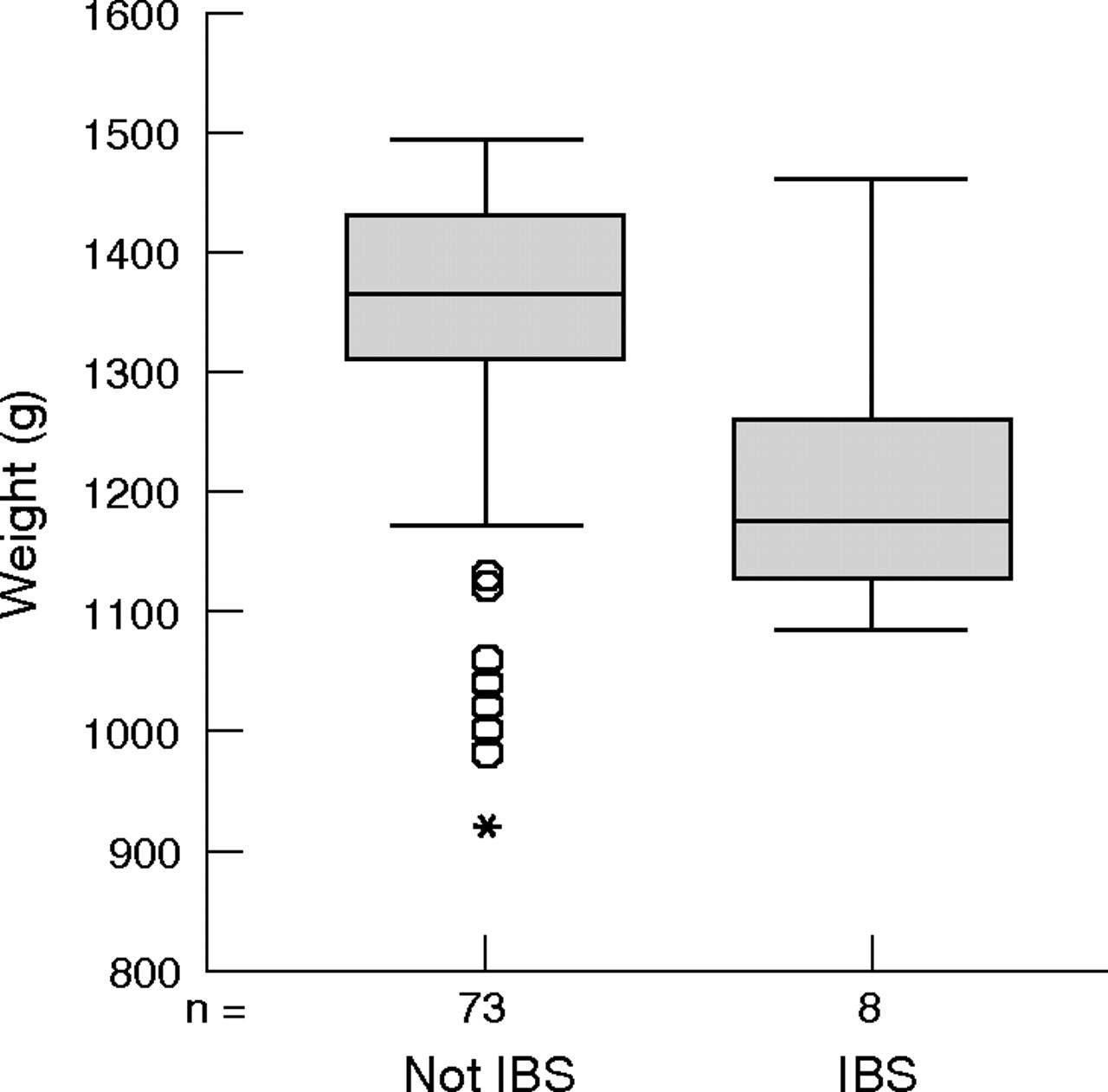
Weight class <1500 g (p = 0.025) and co-twin history of the same disease (p<0.001) were the only measures that significantly affected the risk of IBS. In the weight group <1500 g, there was a significant weight difference between twins with and without IBS, favouring the twin without disease (126.1 g; p = 0.012) (fig 2). Weight differences within the three other groups were small and non-significant between twins with versus those without IBS.

Birth weight difference between twins with and without irritable bowel syndrome (IBS) in the weight group <1500 g. Mean birth weight difference was 126.1 g (p = 0.012), favouring the twin without IBS.
Comparisons between twins with IBS in the four weight groups revealed that earlier onset of symptoms tended to be associated with lowest birth weight (fig 3). Mean difference in age at onset of symptoms between twins weighing less than (9.7 years) and greater than (17.5 years) 1500 g was 7.7 years (p = 0.004).

{kind=link}
{kind=link}
{kind=link}
Comparisons between twins with irritable bowel syndrome in the four weight (w) groups. Results revealed that onset of symptoms tended to be associated with lower birth weight. Mean difference was 7.7 years (p = 0.004).
Effect of birth weight using a co-twin control approach
In the total groups of MZ twins, 97 pairs were discordant for disease. In the three groups with birth weights less than 2500 g, for both twins the weight difference between twins with and without IBS was greatest in the lowest weight group and this difference decreased with increasing birth weight. To increase statistical power, data from the three groups with birth weights below 2500 g (44 pairs) were pooled. Results yielded a significant weight difference of 190.6 g (p = 0.02) favouring the twin without IBS in the weight groups <2500 g.
DISCUSSION
Diagnosis of IBS is still controversial, and is partly made on the basis of exclusion of other diseases. By exclusion of other diseases in the present material, it is likely that patients had IBS or IBS-like disorders. Diarrhoea, constipation, and painful abdominal distension are important components of IBS. The typical chronic course of intermittent symptoms was demonstrated, and the questionnaire on 31 additional diseases did not show comorbidity to any great extent with other chronic diseases, except for dyspepsia, which showed an overlap of 21%. The fact that patients responded selectively to the question of IBS gave the impression that they were familiar with the term, possibly as a result of a medically based diagnosis.
The number of our IBS patients may have been restricted, as a consequence of the question, to those with mostly medically diagnosed IBS, and patients with alternating diarrhoea and constipation, in addition to abdominal distension. This could explain the low prevalence of IBS (5.4%) compared with self reported population based data20 but in agreement with the US community study.21 They estimated the lifetime prevalence of IBS to be 14%, but only 3.3% were medically diagnosed.
We estimated that the lifetime prevalence of IBS in females (7.1%) was significantly higher compared with males (3%). Concordance rate between MZ twins was significantly higher than the concordance rate between DZ twins, indicating that genetic factors play an important role in the development of IBS. Comparing the twin correlation, DZU was lower than DZL, suggesting a sex specific effect. DZM and DZF correlations were similar and high compared with the DZU correlation, and may suggest that either different genes influence liability for IBS in males and females or that the magnitude of genetic effects differs between the sexes. The fact that our sample did not include any concordant MZM pairs limits our conclusions as to the nature of the sex differences but does not imply that there is no heritability in males. The number of twins was probably too small to include any concordant MZM pairs and impeded the estimation of heritability, which relies heavily on the proportion of concordance in MZ to DZ twin pairs. The best fit model estimated the heritability of IBS to be 48.4% among females. This model is consistent with the twin correlations presented in table 1, indicating that familial aggregation of IBS could be accounted for most parsimoniously by genetic factors alone among the females in our sample. The data suggest sex specific effects in the susceptibility to IBS, and may explain the difference in prevalence between the sexes.22 Both the Australian study8 and the larger US study9 estimated a significant higher concordance rate among MZ compared with DZ twins. The US study concluded with a modest genetic effect but also that social learning (parental modelling) had an equal or greater influence on the development of IBS. In the UK study,11 the difference between concordance rate among MZ and DZ twins was non-significant, and genetic modelling analysis revealed that non-shared environmental effects accounted for 75% of the variance in IBS.
The prevalence of IBS in our study (5.4%) was comparable with the US (3%) and Australian study (5%) but much lower than the UK study (17%). Both selection of twins and the criteria used to define the IBS group might be explanatory factors.
The Rome II criteria were used only in the UK study, thereby including a relatively large and different cohort of IBS compared with other studies. This could explain why no genetic influence was found.
The UK study had a female bias (90% of both MZ and DZ twins were females) and was based on volunteers following a media campaign and on a twin registry. Selection bias due to both the method of recruitment and the fact that they had only a 56% response rate might explain the high concordance rates in both the MZ (28%) and DZ (27%) twin pairs.
Only gender (male), which questionnaire was received first, and low birth weight were associated with decreased possibility of participating in our study. Responses to the questionnaire were received from a larger percentage of females (70%) than males (56%), and may explain in part the predominance of IBS among females.
Difference in birth weight in our cohort of complete twin pairs and non-responders was 29 g (95% CI 9.3, 49.4; p = 0.004) and could lead to a slight underestimation of the OR for IBS. The trend in birth weight difference was the same in all weight groups, and therefore unlikely to influence our analyses based on the full sample. Analyses based on co-twin control design would not be affected because they rely on the within pair difference of birth weight in MZ twins discordant for IBS.
This study differed from the three other studies in its use of data on birth weight and gestational age. We wished to explore the influence of nutrition in fetal life, using birth weight as an indicator, on the development of IBS. Our results cannot be used as a basis to explain the importance of non-shared environmental factors for the development of IBS. Restricted birth weight represents only part of this load.
Maturation of the gastrointestinal tract is a dynamic process that is still in progress at birth. Impaired fetal growth could affect both the gut immune system and maturation of the enteric system and its neuropeptides, and thereby influence bowel motility.
Berseth23 used continuous perfusion manometry in preterm and term infants to assess the influence of gestational age on small intestinal motility. They showed that small intestinal motor activity is immature in preterm infants caused by lack of the phase three migrating motor complex (MMC). MMCs, which consist of regular phasic propagating activity in the small bowel, are essential in the movement of food through the intestine. In term infants, MMCs were identified, but differed from adults by shorter duration, suggesting that further maturation occurs during infancy. Cunningham and colleagues24 suggest that maturation of intestinal motility parallels maturation of the central nervous system by showing an association between constipation and neurodevelopment impairment in prematurely born children.
Birth weight <1500 g, but only when adjusted for gestational age, had an independent significant influence on the development of IBS. This result suggests that restricted fetal growth in pregnancy, rather than prematurity, contributes to IBS. Age at onset of symptoms in the lowest weight group (9.7 years) was significantly lower compared with twins weighting more than 1500 g (17.5 years) and might propose a different pathogenesis for the development of IBS in this group. We must assume that medical attention has been sought more often than usual for these children, caused by the early age of onset of IBS. Social learning from anxious parental responses to abdominal complaints from their children and increased healthcare seeking might be explanatory factors, as well as gut immaturity or neurological injury, for their development of IBS.
By using only identical twins discordant for IBS (co-twin control design), we showed that restricted birth weight affected the liability for IBS in the lowest weight group. In the co-twin control analysis, the lowest birth weight group was set to <2500 g to increase the statistical power. Consequently, the risk of IBS between birth weights 1500 g and 2500 g is uncertain. Nevertheless, discordant twin growth is associated with increased risk of morbidity. Several other studies have come to the same conclusion,25–27 that restricted growth is only related to increased risk of morbidity when birth weight is below 2500 g.
In conclusion, we found that a genetic contribution appeared to be important for IBS among females. Moreover, the present study demonstrated for the first time that restricted fetal growth significantly affected susceptibility to IBS later in life. Birth weight less than 1500 g influenced age at onset of symptoms. These results may suggest a new classification of patients into subgroups based on age at onset of symptoms, sex, familial resemblance, and birth weight, to improve our understanding of the pathophysiological mechanisms of IBS.
REFERENCES
Footnotes
-
Conflict of interest: None declared.