Article Text

Abstract
Background COVID-19 has impacted on healthcare provision. Anecdotally, investigations for children with inflammatory bowel disease (IBD) have been restricted, resulting in diagnosis with no histological confirmation and potential secondary morbidity. In this study, we detail practice across the UK to assess impact on services and document the impact of the pandemic.
Methods For the month of April 2020, 20 tertiary paediatric IBD centres were invited to contribute data detailing: (1) diagnosis/management of suspected new patients with IBD; (2) facilities available; (3) ongoing management of IBD; and (4) direct impact of COVID-19 on patients with IBD.
Results All centres contributed. Two centres retained routine endoscopy, with three unable to perform even urgent IBD endoscopy. 122 patients were diagnosed with IBD, and 53.3% (n=65) were presumed diagnoses and had not undergone endoscopy with histological confirmation. The most common induction was exclusive enteral nutrition (44.6%). No patients with a presumed rather than confirmed diagnosis were started on anti-tumour necrosis factor (TNF) therapy.
Most IBD follow-up appointments were able to occur using phone/webcam or face to face. No biologics/immunomodulators were stopped. All centres were able to continue IBD surgery if required, with 14 procedures occurring across seven centres.
Conclusions Diagnostic IBD practice has been hugely impacted by COVID-19, with >50% of new diagnoses not having endoscopy. To date, therapy and review of known paediatric patients with IBD has continued. Planning and resourcing for recovery is crucial to minimise continued secondary morbidity.
- gastroenterology
- health services research
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
What is already known on this topic?
Paediatric severe acute respiratory syndrome coronavirus 2 infection is rare.
Paediatric service provision has been altered as a consequence of the pandemic.
The secondary impact of the pandemic on children and young people with chronic disease may be considerable.
What this study adds?
Sixty-five new IBD ‘diagnoses’ did not undergo endoscopy with histological confirmation (>50% all diagnoses) during April 2020.
Known patients with IBD were followed up virtually, and maintenance therapy was continued.
Recovery of services, including endoscopy, will be key to providing safe care over the coming months.
Introduction
The COVID-19 pandemic has impacted on healthcare provision worldwide. Within the UK, large parts of the medical and nursing workforce, alongside ward and operating theatre space, were redeployed to address the needs of large numbers of unwell adults with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. For the whole of April 2020, the UK population was in lockdown. Within paediatrics, we have not seen an influx of patients with COVID-19, and patient numbers presenting acutely to hospital have significantly decreased1 although there has been a recent recognition of a severe post-COVID-19 multisystem inflammatory disorder in a small subgroup of patients.2 3
While acute admissions have fallen, there is growing concern of the secondary impacts of the COVID-19 pandemic on children with chronic disease. One of the large groups of patients are those with paediatric-onset inflammatory bowel disease (IBD), Crohn’s disease (CD) and ulcerative colitis (UC). This vulnerable group of patients often present with severe disease requiring early escalation of therapy, with nutritional impairment and delayed growth being common at diagnosis.4 5 All diagnosis are usually made in line with the modified Porto criteria, requiring an endoscopic and histological assessment prior to treatment initiation.6–8 During the current SARS-CoV-2 pandemic, this has not always been possible, and delaying treatment to ensure the diagnostic pathway is adhered to is not an option in severe cases.9 Guidance from the British Society of Gastroenterology and National Institute for Health and Clinical Excellence have clearly stated that endoscopy is a high-risk procedure, and there has been a significant drop-off in paediatric and adult procedures nationally.10–12 Endoscopy in children almost always requires a general anaesthetic, and redeployment of anaesthetic teams and theatre space, alongside extensive decontamination time between cases and the need for full personal protective equipment has further impacted on endoscopy services.12 13
Adult and paediatric patients with IBD have largely been categorised as at higher risk of severe SARS-CoV-2 infection and were initially instructed to ‘shield’ from all social contact, or engage with ‘stringent’ social distancing, dependant on their therapies and disease activity.11 Despite this recommendation, the initial data on SARS-CoV-2 infection in paediatric IBD is reassuring. Although this preliminary data must be interpreted with caution,9 14 it is also supported by parallel adult IBD studies.15 There is, however, a potential for secondary harm and adverse effects, as a result of healthcare changes enforced during the lockdown. This includes reduced access to diagnostic endoscopy, difficulties in continuing day-case infusions, lack of face-to-face clinics and problems reviewing patients or performing routine blood or stool monitoring. This, with the additional concerns that patients and parental fears may reduce attendance in hospital, has the potential to cause significant harm. Particularly in paediatric IBD, delay in diagnosis and delayed treatment have the potential to significantly impact on children and young people’s health and well-being, especially impacting on growth.16 17
We performed a nationwide study of paediatric gastroenterology IBD centres in the UK, detailing the impact of the COVID-19 pandemic on the diagnosis and management of patients with IBD during the month of April 2020.
Methods
This study was conducted by the paediatric gastroenterology department at Southampton Children’s Hospital in conjunction with the British Society of Paediatric Gastroenterology, Hepatology and Nutrition (BSPGHAN) IBD working group.
Selection of sites
Twenty paediatric gastroenterology centres were identified with three or more consultant paediatric gastroenterologists, reflecting the tertiary referral units for paediatric IBD in the UK. These centres were located in England and Scotland (Online supplementary data 1).
Supplemental material
Formulation of survey
Questions were formulated focusing on four areas: (1) diagnosis and management of suspected new patients with IBD, (2) facilities available for patients with IBD, (3) ongoing management of IBD including therapy and (4) direct impact of COVID-19 on patients with IBD. Questions were finalised following input from the members of the BSPGHAN IBD working group (online supplementary data 2). In order to ensure comparable data collection, responses were requested to reflect the month of April 2020 during which time the entirety of the UK was in ‘lockdown’. As paediatric IBD centres work in conjunction with a network of referring district general hospitals, we also collected data on the availability of important investigations within these networks .
Supplemental material
Distribution of survey
Survey questions were uploaded to an online format (Google Forms) and a personalised email sent to clinicans at all 20 centres. Each centre was able to complete the online survey only once. Data were collected from 5 May to 11 May 2020, with the collected data reflecting the period from 1st April to 30th April 2020. Results from questions were automatically stored. At the end of the data collection period, all results were downloaded for analysis.
Data analysis
Data are presented as mean values (range), or median value where distribution of data were not normal.
Ethical considerations
This survey was not classified as research according to the Health Research Authority decision tool. Presumed consent was gained by participating centres completing the survey.
Results
All centres completed the survey (100%). Based on Office of National Statistics data, these sites represent approximately 88% of the paediatric (aged <18 years) population of the UK, excluding Southern Wales, Northern Ireland and several smaller specialist paediatric gastroenterology centres.18
Resources available during COVID-19
Endoscopy
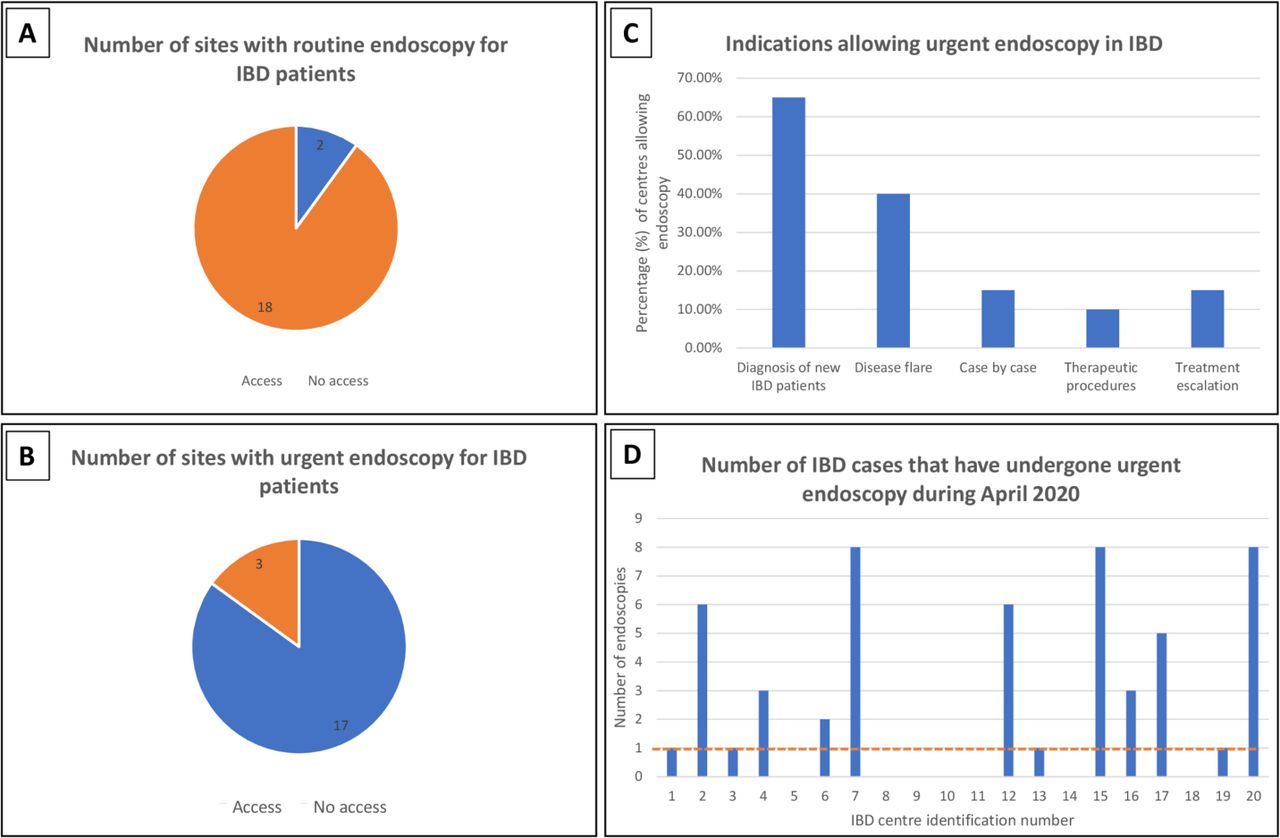
COVID-19 has heavily impacted on paediatric endoscopy for IBD in the UK. Only two sites (10%) reported access to routine endoscopy for patients with IBD during April. Three sites (15%) reported no access to endoscopy for patients with IBD at all, including no urgent diagnostic endoscopy (figure 1A–D). There was significant variation across the UK in the number of procedures performed, ranging from 1 to 8 (median 1 endoscopy per site, in sites with urgent endoscopy available).

(A) Number of sites with routine endoscopy for patients with IBD, 10% of UK centres had routine endoscopy available. (B) Number of sites with urgent (emergency) endoscopy for patients with IBD, 15% of UK centres had no access to endoscopy for patients with IBD during April. (C) In those centres allowing urgent IBD endoscopy (17 sites), the most common indications were new diagnosis of IBD and review of disease flare. In 10%–15% of centres, endoscopy was allowed on a case-by-case basis to assess for treatment escalation and for therapeutic procedures (such as banding). (D) Despite urgent endoscopy being available in 17 centres, procedures were performed in only 13 sites. There was significant variation between sites (range 1–8 endoscopies), with a median of 1 scope performed in sites with urgent endoscopy available. IBD, inflammatory bowel disease.
Review and investigations
There was a significant reduction in the availability of routine investigations across the UK, including three sites that had no access to faecal calprotectin and two (10%) that had no access to either routine ultrasound or routine MRI scanning. The impact in referral networks was more profound with only 25% of networks have full access to faecal calprotectin across the referring units (table 1).
Availability of review and investigations in IBD centres and their associated networks
IBD support services
All units had access to gastroenterology (or IBD) clinical nurse specialists and dietetic support prior to COVID-19. All but one centre had specialist IBD psychology support. During April, 90% of centres retained full nursing support throughout. All centres retained dietetic support, and 95% of centres retained psychological support; however, both dietetic and psychology were frequently moved to remote or online review, similar to medical provision.
Remote reviewing of patients
An average of 94.25% of IBD follow-ups were reviewed using phone, webcam or face-to-face appointments, although this varied considerably across the UK. Three sites were only able to continue 60%–75% of follow-up appointments. Interestingly, 100% of centres were able to review patients by telephone, but only 65% of centres (13 sites) were able to use a webcam-based review system .
Diagnosis and management of new patients with IBD
There was significant impact on the diagnosis and management of patients with suspected IBD, largely driven by the lack of endoscopy availability.
Number of patients diagnosed
A total of 122 patients were diagnosed with confirmed, or presumed IBD during April 2020. Of these patients, 53.3% (n=65) were presumed diagnoses and had not undergone endoscopic or histological examination (table 2). All remaining patients were diagnosed in line with the modified Porto criteria.6 Three sites specifically reported patients with a presumed diagnosis undergoing urgent endoscopy later in the month due to no response to initial induction regimen.
Number of patients diagnosed with IBD or presumed IBD during April 2020
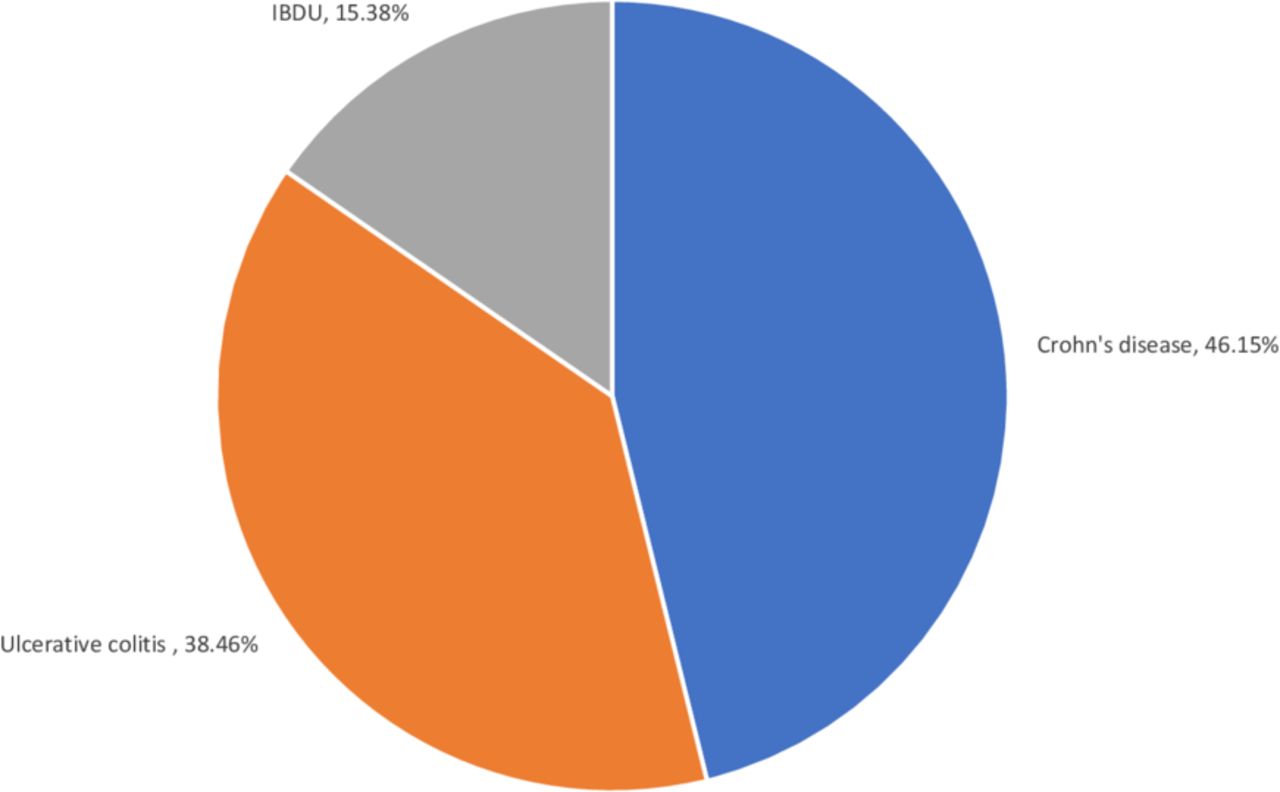
Of the patients with a presumed diagnosis of IBD, clinicians categorised 63.1% of patients as presenting with moderate to severe disease (equivalent to paediatric Crohn's disease acitvity index >30 or paediatric ulcerative colitis acitvity index >30). Presumed diagnoses were 46.1% presumed CD, 38.5% presumed UC and 15.4% with presumed IBD colitis (IBD unclassified). figure 2.
{kind=link}
{kind=link}
Presumed disease subtype in patients with a presumed diagnosis of IBD. IBD, inflammatory bowel disease unclassified.
Initial treatments used for presumed IBD
The most common induction therapy in patients with presumed IBD was exclusive enteral nutrition (44.6%), used in cases of presumed CD. Intravenous and oral steroids were used rarely, potentially reflecting ongoing concerns about SARS-CoV-2 infection in patient on systemic steroids. No patients were started on therapy with anti-tumour necrosis factor (TNF) therapy at diagnosis (table 3).
Treatments used at presumed diagnosis of patients
Maintenance therapy, monitoring and surgery in patients with IBD
Biological therapy
Day-case infusion facilities for biological therapy (and iron infusions) were maintained in all centres. All sites had patients on anti-TNF therapy (infliximab or adalimumab), 19 had children actively on vedolizumab and 15 had children on ustekinumab. No biological therapy was stopped due to COVID-19 during April. Across the whole UK, only a single patient was switched from infliximab infusion to subcutaneous adalimumab due to COVID-19.
Immunomodulators and blood monitoring
All sites had patients on thiopurines, 18 had children on methotrexate and a single centre had a patient on tacrolimus. No systemic immunomodulators were stopped due to COVID-19. All centres continued blood monitoring in hospital, and 95% of centres were able to continue blood monitoring in the community through general practice sites or community nurses. Only two centres (10%) were forced to reduce the frequency of blood monitoring during April.
Surgery in patients with IBD
All centres were able to continue both intestinal and perianal surgery for patients with IBD if required. A total of 14 surgical procedures were conducted in April across seven IBD centres. This included 12 instances of intestinal surgery (including subtotal colectomy, right hemicolectomy and ileostomy formation) and two perianal procedures (abscess drainage and seton insertion).
Discussion
These data demonstrate a significant secondary impact of the COVID-19 pandemic on children and young people with IBD across the entire UK. Over 50% of children and young people presenting with a suspected diagnosis of IBD were diagnosed without a histological diagnosis due to restrictions placed on endoscopy at over 90% of centres across the UK. In contrast, the primary impact of COVID-19 on patients already diagnosed with paediatric IBD appears to be very small19 20
Our data suggest that most paediatric IBD units continued to provide an adequate service despite facing difficulties in following routine diagnostic and therapeutic pathways particularly for new patients. Interestingly, even in the 17 sites with available urgent endoscopy, only 13 had performed procedures, potentially reflecting fewer patients requiring endoscopy than usual due to patients staying home with troublesome symptoms, or the fear of attending hospital. Typically, large paediatric gastroenterology centres would have 2–4 lists per week, with 4–6 patients per list.
There has been a rapid increase in telephone and webcam review, facilitating ongoing care for almost all patients with IBD. In addition, all biological therapy and immunomodulators have been continued, reflecting British Society of Gastroenterology and the European Society of Paediatric Gastroenterology, Hepatology and Nutrition position Porto IBD guidelines that disease flare is more dangerous than continued immunosuppressant therapy.9 11
Based on recent incidence figures, we would expect approximately 4–8 diagnoses of IBD per tertiary referral site, equating to 100–160 diagnoses per month.20 21 In this study, we report 122 diagnoses, or presumed diagnoses, during the month of April. In addition, we describe presumed patients for which the clinician was uncertain of disease classification as IBD colitis, or ‘IBDU’, a diagnosis that is likely to be revised over time. Moreover, presumed patients had a reduced number of CD to UC ratio (1.2:1), compared with published data, ranging from 2.0:1 to 2.1:1.22 23 It will be important to follow-up all patients to ensure a histological diagnosis is achieved.
Diagnosing children and young people with IBD, without a histological confirmation, is controversial and only acceptable given the special circumstances we are currently finding ourselves in. While the major aim is to avoid harm, it is vital to provide adequate treatment for those requiring it. ‘Diagnosis’ without endoscopy requires a combination of blood results, radiological imaging, faecal calprotectin and exclusion of infection, followed by multidisciplinary discussion. Commencing maintenance systemic immunosuppression in children without endoscopic or histological diagnosis is an additional concern, which may become increasingly prevalent in the coming months as there will be a significant time lag before access to paediatric endoscopy returns to the prepandemic levels.
Newly diagnosed CD paediatric patients have long been started on exclusive enteral nutrition as a first-line therapy.24 This induction strategy now appears to have further benefits and was used in nearly 45% of patients with presumed IBD in this study. This strategy presents the additional benefit of not exposing patients to systemic immunosuppression for 4–8 weeks while considering the options for maintenance immunosuppression or biological therapy. Despite this, we are now entering a period where immunomodulatory and biological therapy will need to be started, and the ability to conduct a full disease assessment prior to starting treatment may continue to be limited.
Across all ages, there is concern about the effects of SARS-CoV-2 infection in patients with pre-existing conditions and those on immunosuppressants, especially steroids.25 Interestingly, early data from Wuhan detailing the experience of managing IBD during the initial outbreak demonstrated that the Chinese Society of Gastroenterology guidelines were to stop all immunosuppressant maintenance therapy although patients were still treated with steroids (n=18) or exclusive enteral nutrition (n=15) to induce remission.26 Similarly, initial data from Wuhan and South Korea on paediatric IBD demonstrated lower levels of infection in this group of patients.9 More recent data from Italy, reflecting the experience of 79 IBD patients with COVID-19, indicate that active IBD and increased age, as opposed to treatment, was associated with poorer outcomes.27 Another study from Italy monitored 522 patients with IBD, including ~10% aged <18 years, and reported no cases of COVID-19. Patients were continued on normal therapy for the duration of the 1-month observation period.14 The largest study published to date, from the SECURE-IBD dataset, indicated only 29 patients aged <20 years were diagnosed with COVID-19 worldwide, with only three requiring hospitalisation.28 There were no cases of ventilated paediatric patients and none died.
As data continue to emerge on the effect of SAR-CoV-2 infection on patients with IBD, it is important to begin to contextualise patient risk. There is potential for widespread secondary harm through inadequate or incorrect diagnosis, undertreatment due to concerns regarding immunosuppression, and a delay in presentation. In children, the major risk now appears to be lack of endoscopy capacity and reduced resourcing in referral networks. It is clear these issues are likely to present ongoing challenges in both paediatric and adult practice for many months, as endoscopy capacity is unlikely to recover immediately, although services are gradually being reinstated.12 Assessment of services in the recovery phase will be required.
Many children presenting with IBD are unable to wait for weeks or months before starting therapy due to adverse, irreversible, impacts on growth and severity of symptoms.29 Guidance on safe diagnosis and management, along with starting maintenance therapy, will need to be updated as we progress through this pandemic. Despite these issues, this pandemic also allows the potential for improvement of care in several areas. Virtual appointments, virtual multidisciplinary discussions and improvement of networks by remote collaboration all provide the opportunity for better care within specific situations, with the potential to minimise lost school time by rationalising hospital attendance where possible.30 Further data on patient and family preferences will need to be gathered over the coming months.
Conclusion
These data provide the first insight into the secondary impact of COVID-19 on paediatric patients presenting with a new diagnosis of suspected IBD and on patients with an established diagnosis of IBD. Over 50% of patients were unable to undergo normal diagnostic procedures in April 2020. We must now ensure that resourcing for patients with IBD is adequate in the recovery phase. Despite additional challenges, care for known patients with IBD has been largely maintained, with no patients missing infusions, surgery continuing and remote reviews now commonplace. In coming months, additional challenges will present, including management of treatment escalation and longer term disease activity monitoring. We will need to remain mindful of preventing harm to patients and continue data collection in order to monitor practice and facilitate recovery of normal services.
Acknowledgments
Contributors: Marcus KH Auth (Liverpool); Loveday Jago (Manchester); Andrew Fagbemi (Manchester); and Edward Gaynor (GOSH).
References
Footnotes
Twitter @james__ashton, @RMBeattie50
Contributors JJA, JK and RMB designed the study. JJA, JK, CS, DD, FT, TP and RMB designed, or inputted, to the survey questions. All authors contributed data. JJA wrote the manuscript with JK and RMB. All authors commented on the manuscript and approved the final version for submission.
Funding The study was supported by the British Society of Paediatric Gastroenterology, Hepatology and Nutrition IBD working group. JJA is funded by an action medical research training fellowship and by an ESPEN fellowship. RH is supported by a National Health Service Research Scotland Career Researcher Fellowship.
Competing interests RH has received consultancy or speaker’s fees and travel support from Nutricia and 4D pharma. All remaining authors declare no competing interests related to this manuscript.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. All available data are available in the manuscript.