
Abstract
Purpose
Perforated colonic diverticular disease is associated with a high rate of late sequel and mortality. The risk of colonic perforation may relate to intracolonic pressure and mucosal barrier function in the wall of diverticula. The use of substances affecting these parameters may therefore be associated with the risk of developing a perforation. The aim was to study the effect of nonsteroidal anti-inflammatory drugs (NSAIDs), opioids, corticosteroids, calcium channel blockers, and antimuscarinics on perforation in diverticular disease.
Materials and methods
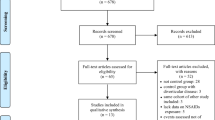
A review of 54 patients with colonic diverticular perforation—forming the case group—and 183 patients with verified colonic diverticular disease—forming the control group—was done. Patient characteristics and drug use was registered.
Results
Case group and control group were comparable with respect to sex, age, and comorbidity. In multivariate analysis, the use of NSAIDs (OR 3.56; 95% CI 1.50–8.43), opioids (OR 4.51; 95% CI 1.67–12.18), and corticosteroids (OR 28.28; 95% CI 4.83–165.7) were significantly associated with perforated diverticular disease. Acetylsalicylic acid in cardiologic dose did not affect the rate of perforation (OR 0.66; 95% CI 0.27–1.61). The use of calcium channel blockers was associated with a reduced rate of diverticular complications (OR 0.14; 95% CI 0.02–0.95).
Conclusions
The administration of NSAIDs, opioids, and corticosteroids are associated with an increased risk of colonic diverticular perforation. Acetylsalicylic acid in cardiologic dose does not affect the risk of perforation. Calcium channel blockers are associated with a reduced risk of perforation.
Similar content being viewed by others


References
Elliott TBYS, Irvin TT (1997) Five-year audit of the acute complications of diverticular disease. Br J Surg 84(4):535–539
Chandra VNH, Larson DR, Harrington JR (2004) Impact of primary resection on the outcome of patients with perforated diverticulitis. Arch Surg 139(11):1221–1224
Kriwanek SAC, Beckerhinn P, Dittrich K (1994) Prognostic factors for survival in colonic perforation. Int J Colorectal Dis 9(3):158–162
Bielecki KKP, Klukowski M (2002) Large bowel perforation: morbidity and mortality. Tech Coloproctol 6(3):177–182
Tudor RGFN, Keighley MRB (1994) National audit of complicated diverticular disease: analysis of index cases. Br J Surg 81:730–732
Morris CRHI, Stebbings WSL, Speakman CTM, Kennedy HJ, Hart AR (2002) Epidemiology of perforated colonic diverticular disease. Postgrad Med J 78:654–659
Morris CRHI, Stebbings WSL, Speakman CTM, Kennedy HJ, Hart AR (2003) Anti-inflammatory drugs, analgesics and the risk of perforated colonic diverticular disease. Br J Surg 90:1267–1272
Wilson RGSA, Macintyre IMC (1990) Complications of diverticular disease and non-steroidal anti-inflammatory drugs: a prospective study. Br J Surg 77:1103–1104
Goh HBR (2002) Non-steroidal anti-inflammatory drugs and perforated diverticular disease: a case control study. Ann R Coll Surg Engl 84:93–96
Yalouris AGRS (1987) Steroids, non-steroidal anti-inflammatory drugs, and serious septic complications of diverticular disease. Br Med J 295:1238
Mpofu SMC, Hutchinson D, Maier AE, Dodd SR, Moots RJ (2004) Steroids, non-steroidal anti-inflammatory drugs, and sigmoid diverticular abscess perforation in rheumatic conditions. Ann Rheum Dis 63:588–590
Aldori WHGE, Rimm EB, Wing AL, Willett WC (1998) Use of acetaminophen and nonsteroidal anti-inflammatory drugs: a prospective study and the risk of symptomatic diverticular disease in men. Arch Fam Med 7:255–260
Langman MJSML, Worall A (1985) Use of anti-inflammatory drugs by patients admitted with small or large bowel perforations and haemorrhage. Br Med J 290:347–350
Schiffmann LKS, Berger G, Buhr HJ (2005) Colon perforation in an adolescent after short-term diclofenac intake. ANZ J Surg 75(8):726–727
Durieux SRS, Bourgeois P (1999) Complications of colonic diverticular disease during rheumatoid polyarthritis: 7 cases. Rev Med Interne 20(1):50–53
EL A (1990) Corticosteroid-association perforation of colonic diverticula. Arch Intern Med 150(6):1337–1338
Aloysius MMKP, Lobo DN (2006) Non-steroidal anti-inflammatory drug (NSAID)-induced colonic strictures and perforation: a case report. Dig Liver Dis 38(4):276–278
Robinson MH, Wheatley T, Leach IH (1995) Nonsteroidal anti inflammatory drug-induced colonic stricture. An unusual cause of large bowel obstruction and perforation. Dig Dis Sci 40(2):315–319
Candelas GJJ, Fernandez B, Rodriguez-Olaverri JC, Calatayud J (1998) Perforation of the sigmoid colon in a rheumatoid arthritis patient treated with methylprednisolone pulses. Scand J Rheumatol 27(2):152–153
Dalla Valle RCE, Mazzoni MP, Busi N, Benozzi L, Sivelli R, Sianesi M (2005) Acute diverticulitis with colon perforation in renal transplantation. Transplant Proc 37(6):2507–2510
Beaver TMFD, Zamora MR, Badesch DB, Weill D, Brown JM, Campbell DN, Grover FL (1996) Colon perforation after lung transplantation. Ann Thorac Surg 62(3):839–843
Painter NSTS, Ardran GM, Tuckey M (1965) Effect of morphine, prostigmin, pethidine, and probanthine on the human colon in diverticulosis studied by intraluminal pressure recording and cineradiography. Gut 6:57–63
Schang JCHM, Hebert M, Pilote M (1986) How does morphine work on colonic motility? An electromyographic study in the human left and sigmoid colon. Life Sci 38(8):671–676
Frantzides CTCV, Salaymeh B, Tekin E, Condon RE (1992) Morphine effects on human colonic myoelectric activity in the postoperative period. Am J Surg 163(1):144–148
Morris CRHI, Stebbings WSL, Speakman CTM, Kennedy HJ, Hart AR (2003) Do calcium channel blockers and antimuscarinics protect against perforated colonic diverticular disease? A case control study. Gut 52:1734–1737
De Ponti FGC, Cosentino M, Lecchini S, Frigo G (1993) Calcium-channel blockers and gastrointestinal motility: basic and clinical aspects. Pharmacol Ther 60(1):121–148
Bassotti GCC, Annese V, Fiorella S, Roselli P, Morelli A (1998) Nifedipine and verapamil inhibit the sigmoid colon myoelectric response to eating in healthy volunteers. Dis Colon Rectum 41(3):377–380
Sun SGS, Kim DY, Schreiber TC, Schechner RS, Tellis VA (1997) Nifedipine protects small intestine from cyclosporine-induced hemodynamic and functional impairment. J Surg Res 69(2):295–299
O’Brien MDCM, Thomforde GM et al (1997) Effect of cholecystokinin octapeptide and atropine on human colonic motility, tone, and transit. Dig Dis Sci 42:26–33
Suchowiecky MCD, Bhasker M, Perry RJ, Snape WJ Jr (1987) Effect of secoverine on colonic myoelectric activity in diverticular disease of the colon. Dig Dis Sci 32(8):833–840
Hansen OSW (1999) Divertikelerkrankung des Kolons—Stufenkonzept durch exakte Stadieneinteilung. Langenbecks Arch Chir Suppl II:1257–1260
Painter NSBD (1975) Diverticular disease of the colon, a 20th century problem. Clin Gastroenterol 4(1):3–21
Blachut KPL, Garcarek J (2004) Prevalence and distribution of the colonic diverticulosis. Review of 417 cases from Lower Silesia in Poland. Rom J Gastroenterol 13(4):281–285
Lanas ASP, Bajador E, Esteva F, Benito R, Sainz R (1997) Evidence of aspirin use in both upper and lower gastrointestinal perforation. Gastroenterology 112(3):683–689
Campbell KSR (1991) Non-steroidal anti-inflammatory drugs and perforated diverticular disease: a case control study. Br J Surg 78:190–191
Weiner HLRA, Cooper PR (1993) Sigmoid diverticular perforation in neurosurgical patients receiving high-dose corticosteroids. Neurosurgery 33:40–43
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Piekarek, K., Israelsson, L.A. Perforated colonic diverticular disease: the importance of NSAIDs, opioids, corticosteroids, and calcium channel blockers. Int J Colorectal Dis 23, 1193–1197 (2008). https://doi.org/10.1007/s00384-008-0555-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-008-0555-4