Article Text

Abstract
Objective Gibraltar is a unique densely populated multicultural British Overseas Territory for which no population data on disorders of gut–brain interaction have existed.
We aimed to provide the first-ever assessment of prevalence of irritable bowel syndrome and functional dyspepsia in Gibraltar in relation to their diagnostic recognition and healthcare burden.
Design An internet survey was carried out in Gibraltar in 2019–2020. The study survey included demographic questions, the Rome IV diagnostic questions for functional dyspepsia and irritable bowel syndrome, relevant medical history, previous surgeries, medication use, healthcare visit frequency and a quality-of-life questionnaire.
Results 888 individuals (3.5% of all Gibraltar adults) completed the survey anonymously. Irritable bowel syndrome prevalence was 5.2% (95% CI 3.7% to 6.6%). Functional dyspepsia prevalence was 9.9% (95% CI 7.9% to 11.9%). The two conditions overlapped substantially. Women had higher mean prevalence than men of both disorders. People meeting criteria for either or both disorders were prone to surgeries, had more frequent healthcare visits, higher medication use and lower quality-of-life scores compared with people without these disorders. Diagnostic recognition by healthcare providers was low, leaving 58.3% of irritable bowel syndrome and 96.9% of functional dyspepsia individuals undiagnosed.
Conclusion This first-ever population-based study of Rome IV defined irritable bowel syndrome and functional dyspepsia in Gibraltar indicates that the prevalence rates of these disorders are similar to the recently reported data for the UK and Spain, but they remain poorly recognised despite substantially affecting the quality of life of individuals who have them in the Gibraltar community.
- IRRITABLE BOWEL SYNDROME
- FUNCTIONAL DYSPEPSIA
- QUALITY OF LIFE
- EPIDEMIOLOGY
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The Global Epidemiology Study conducted by the Rome Foundation, assessing the worldwide prevalence of disorders of gut–brain interaction (DGBI) using the Rome IV diagnostic criteria, was completed in 2019. The first published data revealed a prevalence rate of 40.3% for all DGBI in the general adult population of 26 countries using internet surveys.
DGBI have been consistently found to be female predominant in epidemiological studies throughout the years and have also often been reported to prevalent in younger individuals.
A significant healthcare burden is associated with DGBI: increased healthcare seeking, repetitive and inconclusive diagnostic test, and excess abdominal and pelvic surgeries add up to up to increased healthcare costs.
Health-related quality of life is impacted significantly in patients with DGBI, compared with the general population.
WHAT THIS STUDY ADDS
Our study is the first ever epidemiology survey on DGBI performed in Gibraltar. As far as we know, with data obtained from 3.5% of the total adult population of Gibraltar, it is also the highest population proportion ever sampled in any of the epidemiology studies on DGBI.
The study focused on the prevalence and particularities of two of the most common DGBI: irritable bowel syndrome (IBS) prevalence was found to be 5.2% (95% CI 3.7% to 6.6%) and functional dyspepsia (FD) prevalence 9.9% (95% CI 7.9% to 11.9%). These prevalence rates are similar to those in the recently reported data for UK and Spain, two countries with cultural, economic and political influence in the region.
Diagnostic recognition by healthcare professionals was poor for both disorders in our study, leaving 58.3% of people with IBS and 96.9% of those with FD undiagnosed. Based on these data, we established a doctor-diagnosis sensitivity of 56.5% for IBS and 2.3% for FD with a specificity of 89.3% for IBS and 99.6% for FD.
Healthcare burden of these disorders was significant as reflected by an excess frequency of physician visits, use of prescription or over-the-counter medication and increased number of surgical interventions. Despite these efforts, the quality of life of people with these DGBI remained significantly affected by their conditions as demonstrated with the help of the Patient-Reported Outcomes Measurement Information System Global-10 questionnaire—both on its physical and mental health components.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Gibraltar, as a cradle of different cultural groups co-existing undisturbed in their communities is a perfect setting for studying multicultural aspects of DGBI through the prism of the biopsychosocial model. Our findings suggest that general prevalence rates may differ from data from participants’ countries of origin and indicates the importance of the local circumstances in precipitating symptoms.
This study demonstrating poor recognition of DGBI resulting ill-placed high healthcare costs and service burden is highlighting need for further education, urges for imminent practice changes that should be included in up to date guidance policies and patient pathways.
The wide spectrum of clinical presentations and overlapping disorders will need to channel management from sole practitioners to specialist multidisciplinary teams able to offer the required standard of care.
Introduction
Gibraltar is a British Overseas Territory situated at the southernmost tip of the Iberian Peninsula, bordered by Spain. With a population density of 3369 inhabitants per km2, it is the fifth most densely populated area of the world.1 Its demographic particularities reflect the racial and cultural fusion of economic immigrants of many nationalities who settled in the area.2
While disorders of gut–brain interaction (DGBI) prevalences have been formally assessed in epidemiological surveys in many areas around the world, including the Global Epidemiology Study conducted by the Rome Foundation, which surveyed populations of 33 countries for this purpose, no study has documented DGBI epidemiology in Gibraltar to date.3 Our pioneering project collected this much-needed information for the purposes of better understanding the prevalence and burden of DGBI in this unique population.
Healthcare seeking behaviour and economic burden have been repeatedly described in relation to DGBI, as their diagnosis and management remain challenging, leading to unnecessary costs and doctor visits.4 5 Due to their chronic remitting-relapsing progress, they have a great impact on an individual’s general state of well-being aside from their specific GI complaints.6
This paper examines the prevalence, diagnostic recognition, healthcare burden and quality of life of patients fulfilling the Rome IV criteria for two of the most common DGBIs, irritable bowel syndrome (IBS) and functional dyspepsia (FD), in Gibraltar.
Materials and methods
Questionnaire
A comprehensive survey questionnaire was issued in the two most commonly used languages in the territory—English and Spanish—collecting the following information:
Demographics: age, sex, place of birth, primary language and length of residence in Gibraltar.
The IBS and FD modules of the Rome IV Diagnostic Questionnaire for Adults, which identify symptom patterns consistent with the Rome IV diagnostic criteria for these two DGBI and their subtypes.7
Questions about previously received clinical diagnoses including the most common organic gastrointestinal (GI) conditions that can produce symptoms similar to IBS or FD: peptic ulcer, coeliac disease, inflammatory bowel disease and GI cancer, as well as history of bowel resection. These were used as exclusion criteria from the Rome IV IBS and FD diagnosis. Further questions enquired about previously received diagnoses of IBS and FD, as well as disorders related to GI function: gastro-oesophageal reflux disease (GERD), chronic diarrhoea, chronic constipation, diverticulosis and diabetes; non-GI conditions like fibromyalgia or migraine and history of previous surgical interventions including cholecystectomy, appendectomy, hysterectomy and other abdominal or pelvic surgeries.
Healthcare utilisation was measured by self-reported frequency of healthcare visits, previous surgical procedures and regularly used prescription and over-the-counter medications.
Quality of life was measured with the Patient-Reported Outcomes Measurement Information System (PROMIS) Global-10 questionnaire consisting of 10 items assessing the physical and mental dimensions of health.8
Questionnaire distribution and completion
Based on the latest official census from 2012, we identified the target numbers for different sex and age subgroups to get a representative sample of the adult (18+ years old) population of Gibraltar, which totals 25 178 individuals.9 Calculating with a 95% CI and margin of error of 3%, a sample size of 1024 surveys was proposed. Participants were selected randomly based on their registration with the Gibraltar Health Authority, the only major healthcare provider in the area. We have created a representative sample of the population based on their basic demographic attributes—age and sex. Eligibility criteria were set for a minimum of 5 years residency in Gibraltar.
Data collection ran between December 2019 and November 2020 with the public project name of ‘GIGA Study—Gibraltar Gastrointestinal Health Survey’. The data collection was conducted through a password-protected website connected to a secure internet survey using Qualtrics XM software, managed at the University of North Carolina, USA. A total of 5565 invitation letters were sent out by post containing a brief description of the study, 5-letter unique participant access codes and website address to complete the survey. Participants logging into the survey website gained access to the questionnaires after agreeing to participate on an electronic consent form. The data collection was fully deidentified and results were not accessible to the recruiting team until the survey closed.
Statistical analysis
For the purposes of testing relationships between questionnaire-based scales and the existence of specific health conditions, the standard practice is to use analysis of variance (ANOVA) test, assuming a normally distributed parametrical data set. As most of our data were ordinal and frequently non-normally distributed, we also performed the nonparametric Kruskal-Wallis test designed for this scenario. At a significance level of p<0.05, the result of the two approaches were the same for all comparisons. For differences found between subgroups, we used the nonparametric Dunn post hoc test to pinpoint its source. Pearson’s χ2 test of independence was used, where applicable, for frequency data in contingency tables. Descriptive analysis relied on the mean and its parametric CI. Frequency distributions were expressed as prevalence numbers and percentages. We used the statistical software R (V.4.1.0) for our analysis.
Results
A total number of 888 surveys were completed. The median completion time was 13.8 min.
Demographic distribution of surveyed population
The average response rate was 15% across all sex and age groups with females aged 25–44 being most active responders (23.9% 162/678) and males aged 18–24 being least interested (7.5% 63/841). The distribution of participants by sex was 56.1% females and 43.9% males with a mean age of 43.9 years (range 18–89).
Prevalence of DGBI
Based on the Rome IV criteria, IBS prevalence was 5.2% (95% CI 3.7% to 6.6%): 1.8% had IBS with constipation, 1.7% IBS with diarrhoea, 1.5% mixed subtype and 0.2% unsubtyped IBS.
FD prevalence was 9.9% (95% CI 7.9% to 11.9%): 6.2% of those had postprandial distress syndrome (PDS) alone, 1.9% epigastric pain syndrome (EPS) alone and 1.8% PDS +EPS.
IBS and FD overlapped substantially: FD was present in 47.8% of IBS cases, and IBS present in 25% of FD cases. Examining the relations between these subgroups, we established an OR of 10.08 (95% CI 5.36 to 18.95), p<0.0001* for people with IBS to fulfil criteria for FD as well.
Correcting the raw sample prevalence values with weights to make them equivalent to the age and sex distribution in the Census-reported Gibraltar adult population,9 prevalence estimates were 4.4% for IBS and 9.6% for FD.
These prevalence rates are similar for both IBS and FD compared with the data published for UK and Spain in the Global Epidemiology Study3 (table 1).
Prevalence rates (% and 95% CI) for all Rome IV defined DGBIs, IBS and FD and comparison in most relevant countries
Based on Rome IV diagnoses, we created the following subgroups for the purposes of further analysis:
‘IBS’ group fulfilling Rome IV criteria for IBS but not FD (n=24, 2.7%).
‘FD’ group fulfilling Rome IV criteria for FD but not IBS (n=66, 7.5%).
‘IBS and FD’ group fulfilling Rome IV criteria for both IBS and FD (n=22, 2.5%).
‘Organic GI’ group reporting organic GI conditions used as exclusions (n=49, 5.5%).
‘Non-GI’ group without IBS, FD or organic GI diagnosis (n=725, 81.8%).
Effect of sex on DGBI prevalence
Women had higher mean prevalence rates than men of both disorders: 7.6% (95% CI 5.3% to 9.9%) female vs 2.1% (95% CI 0.6% to 3.5%) male for IBS and 12.9% (95% CI 9.9% to 15.8%) female vs 6.2% (95% CI 3.8% to 8.5%) male for FD; p<0.001 for both.
When analysing for influence of sex on Rome IV DGBI diagnosis, we found an OR of 3.9 (95% CI 1.8 to 8.5), p=0.0005 for women to fulfil criteria for IBS compared with their male counterparts. A significant effect was also noted for FD, with an OR of 2.2 (95% CI 1.4 to 3.6), p=0.00126 for women compared with men (figure 1A).
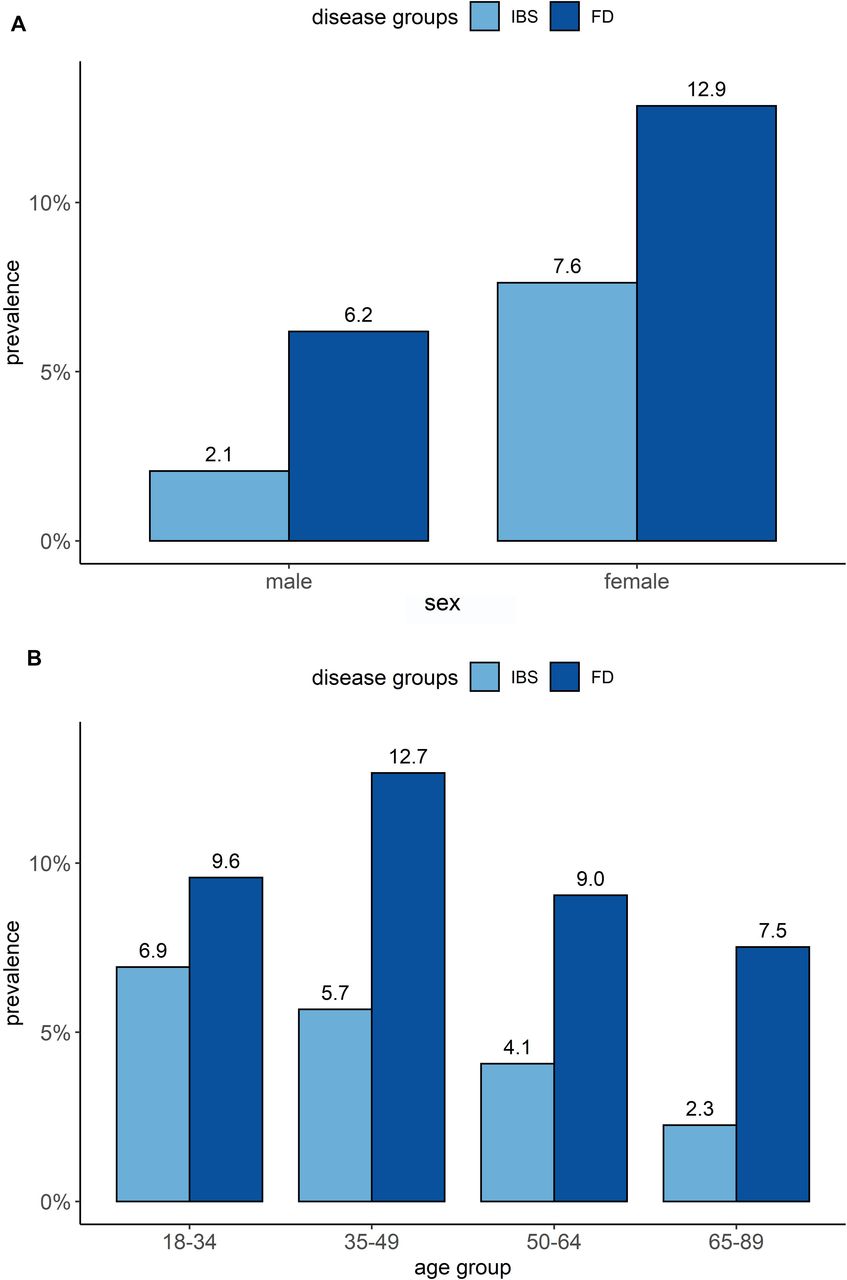
Prevalence of IBS and FD according to sex (A) and age (B). FD, functional dyspepsia; IBS, irritable bowel syndrome.
Effect of age on DGBI prevalence
DGBI were more prevalent among young people. In our sample, IBS had a prevalence of 6.9% in the 18–34 years age group, decreasing to only 2.3% in the oldest 65+ years age group. Among people meeting FD criteria, the prevalence was highest in people aged 35–49 years, 12.7%, dropping to 7.5% in the 65+ yearsage group (figure 1B).
Diagnostic recognition of DGBI by healthcare professionals and associated organic GI disorders
A diagnosis of IBS was previously established by a doctor in 116 participants, but only 26 of them currently met the Rome IV criteria for IBS (22.4%) (table 2). Despite the relatively frequent doctor-diagnosis of IBS, only 41.7% of participants meeting Rome IV IBS criteria had been recognised as such, leaving 58.3% undiagnosed. Sixty-six individuals (9.1%) in the non-GI group had previously been diagnosed with IBS.
Diagnostic recognition and received medical or surgical treatment for individuals meeting criteria for Rome IV
A doctor diagnosis of FD was much less frequent compared with IBS. Only 2 of 66 individuals (3.0%) meeting Rome IV FD criteria in the survey had been diagnosed by a doctor with FD while 13 (19.7%) were identified as IBS. Three participants (0.4%) who currently did not meet the Rome IV criteria for FD reported having received a clinical diagnosis of FD.
From the 22 participants with overlapping Rome IV IBS and FD, 16 had received a clinical diagnosis of IBS (72.7%). None of them had been clinically diagnosed with FD and 6 (27.3%) had not received any DGBI diagnosis.
Based on the above data, we established that a doctor diagnosis had a sensitivity of 56.5% for IBS and 2.3% for FD with a specificity of 89.3% for IBS and 99.6% for FD.
Healthcare burden of DGBIs
In table 2, we have listed all coexisting medical conditions enquired about in the survey and the previously described exclusions to the DGBI groups. GERD and diverticular disease were twice as prevalent in the DGBI groups compared with the non-GI group. However, due to their frequently mild, less interfering progress they were not assigned to the organic GI group.
Functional disorders of other bodily systems were much more prevalent in patients with a DGBI diagnosis. Fibromyalgia had a prevalence of 0.5% in the non-GI group, but this was increased 15 times in IBS (8.3%), 11 times in FD (6.0%) and 25 times when both conditions coexisted (13.64%). Migraine had a prevalence of 10.5% in the non-GI group but three times higher in IBS (33.3%) and was twice as frequent in FD (24.2%) or overlapping IBS and FD (18.2%).
Frequency of surgical procedures
Participants with DGBI reported having undergone an increased number of surgical procedures.
Cholecystectomy rate was 2.7 times higher in patients with FD (10.61%) versus the non-GI group (3.9%) (table 2). Similar elevated rates were observed in the IBS group (8.3%) or IBS and FD group (9.1%).
Appendectomy rate was 2.1-fold higher in overlapping IBS and FD (18.2%) versus the non-GI group (8.5%) and 1.5-fold increased in IBS (12.5%). The rate was not increased in FD (4.5%).
Hysterectomy prevalence was the highest of all surgical procedures assessed in the survey. IBS (16.7%) and overlapping IBS and FD (18.2%) patients were almost six times more likely to undergo the procedure compared with versus the non-GI group (3.2%); p<0.001. The prevalence was doubled in the FD group (6.1%).
Bowel resections were reported by eight participants (1%). These individuals were excluded from the Rome IV diagnostic algorithm due to possible false positive DGBI diagnostic results.
Other pelvic-abdominal surgeries were 3.9 times as prevalent in IBS (33.3%) as in the non-GI group (8.8%), and were increased 1.8-fold in FD (15.2%) and 2.6-fold in IBS and FD (22.7%).
Medication use related to existing DGBI
Multiple-choice questions enquiring about types of medication used regularly helped map the differences in use between the groups (table 2.).
In accordance with the predominant symptoms, medications for constipation, diarrhoea or bloating were consumed much more commonly by people in the IBS group. Although similar proportions were noted in the FD group as well, the latter group mainly stood out with greater use of antiacid medication. Medicine use was highest in the overlapping DGBI group.
Regular use of prescription analgesics was twice as frequently reported by people with IBS or FD compared with non-GI individuals and five times more by those in overlapping IBS and FD group. This was associated with a similar pattern of excess over-the-counter pain medication use.
Psychotropic agents, neuromodulators and sleeping tablets were almost 10 times more frequently used in the overlapping IBS and FD, and 2–3 times more often in IBS or FD, when compared with the non-GI groups.
Frequency of healthcare visits
Half of the population surveyed reported attending a healthcare facility a few times a year (47.7%) and only 5.0% of them once a month or more (table 3).
Quality of life (PROMIS Global 10 score and 95% CI) and healthcare utilisation (% and 95% CI) in individuals meeting criteria for Rome IV IBS, FD or both disorders compared with individuals not meeting criteria for neither disorder or diagnosed with organic GI disease
In the non-GI group, 3.3% reported seeing a doctor at least monthly. In the DGBI groups, this proportion increased threefold (10.6%) in FD, fivefold (16.7%) in IBS and in excess of 10 times in overlapping IBS and FD, of whom 31.8% reported visiting doctors at least monthly.
Quality of life
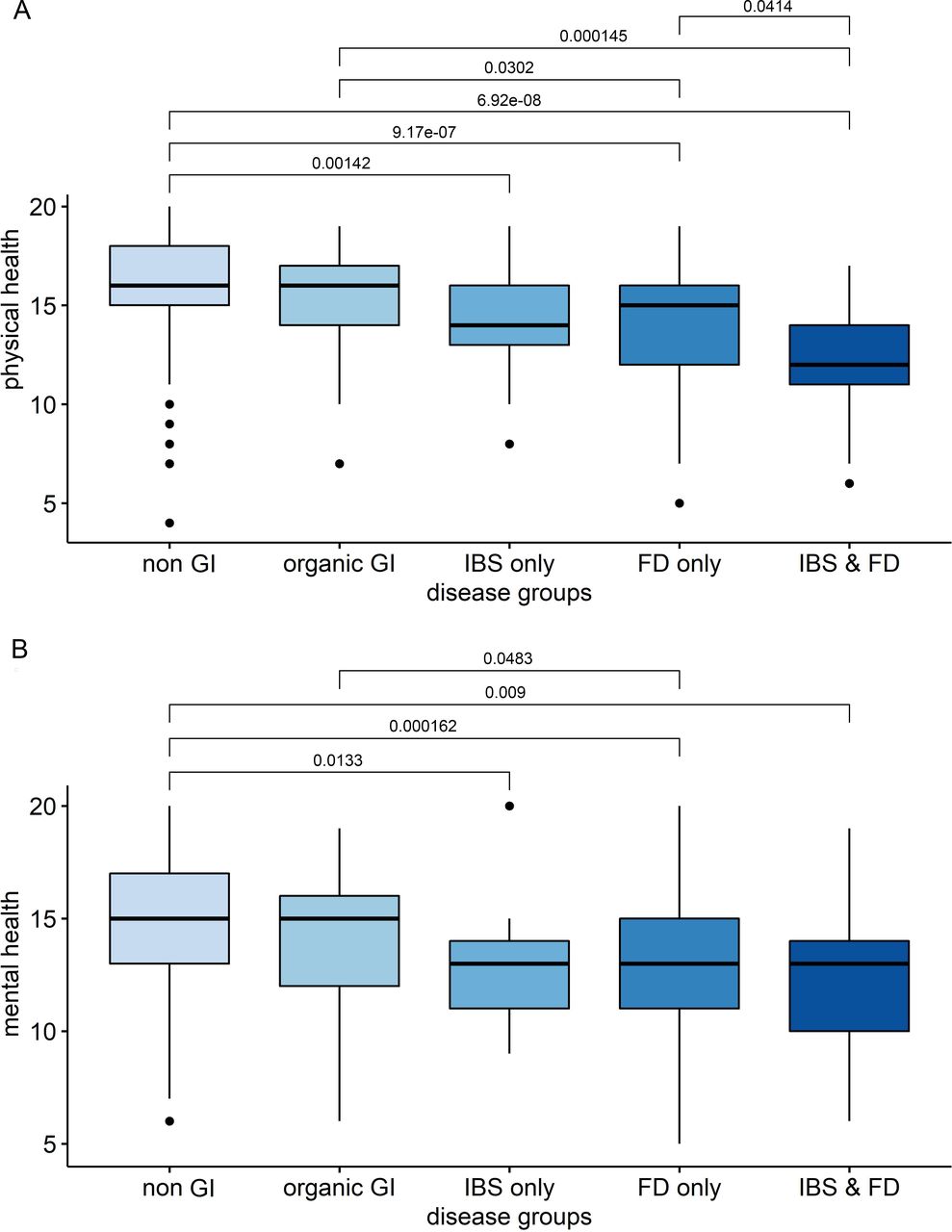
The participants’ quality of life, measured with the PROMIS Global-10 questionnaire, showed statistically significant differences between groups on both the Physical Component Scores and Mental Component Scores (table 3.).
Mean Physical Component Scores were highest (16.0) in the non-GI group. The organic GI group had a similar score (15.4). We saw significant decrease in single DGBI (14.0) both in IBS and FD and even greater decrease in overlapping IBS and FD (12.2). Kruskal Wallis test: p<0.001, χ2=69.57, df=4; ANOVA: p<0.001. By using Dunn’s test, IBS and FD and FD groups separated well from the organic GI and non-GI groups separated from all DGBI groups (figure 2A).

{kind=link}
{kind=link}
PROMIS 10—physical (A) and mental (B) quality of life measure between subgroups. Horizontal bars represent statistically significant differences (p<0.05) between the mean scores of disease groups, on the Dunn post hoc test (non-parametric)—Benjamini-Yekutieli adjustment. FD, functional dyspepsia; GI, gastrointestinal; IBS, irritable bowel syndrome; PROMIS 10, Patient-Reported Outcomes Measurement Information System.
The Mean Mental Component Score showed a similar pattern. The non-GI and organic GI groups had similar scores (14.7 and 14.2), while they were decreased for IBS (13.0) and FD (12.9) and lowest in the IBS and FD group (12.5). Kruskal Wallis test: p<0.001, χ2=36.11: p, df=4; ANOVA: p<0.001. Dunn’s test showed good DGBI group separation from the non-GI group. (figure 2B)
Discussion
There has been a long-standing interest in the field of DGBI research in understanding to what extent DGBI prevalence and associated biopsychosocial factors vary in different populations around the world. These differences were hard to evaluate in the past due to different survey methodologies and use of varying diagnostic criteria. To remedy this, the Rome Foundation recently carried out a Global Epidemiology Study of DGBI, using a uniform research questionnaire including the Rome IV diagnostic questionnaire to survey population samples in 33 countries around the globe.3 Our group used a similar methodology to produce the first ever data available on two of the DGBI in Gibraltar. Due to these similarities, our findings on DGBI prevalence rates for Gibraltar can be directly compared with those of national population findings in that study. Managing to survey 3.5% of Gibraltar’s general adult (age 18+) population, we have achieved a representative sample, that is, as far as we know, the highest proportion of a population sampled in any epidemiology study of DGBI. These aspects are the most important strengths of our study.
A further strength derives from the epidemiology principles followed during the survey administration. Participants were selected and invited based only on their demographics, eliminating any bias related to their health history.
The relationship of sex and age to DGBI prevalence in our results was generally in line with the existing literature suggesting that these disorders are more common in young individuals, gradually diminishing with age and have female predominance.10
FD was a much less frequent diagnosis than IBS in the medical history of our participants even though our data show it is more prevalent in Gibraltar than IBS when identified by Rome IV criteria. This could highlight once more how the lack of using Rome criteria in the daily clinical practice can leave patients wrongly or undiagnosed, potentially resulting in inadequate medication use with little therapeutic success or patient satisfaction. The high rate of coexisting GERD in this cohort can further confound the clinical picture.
Patients with DGBI are prone to have surgeries. Studies from as far back as 1928, when Ryle has described a 36% increased rate of appendectomies in patients suffering with IBS, have highlighted this relationship.11 Our study found similar relationships with DGBI, with twofold increased cholecystectomy and appendectomy rates in line with data presented in literature.12 Higher than previously documented,13 hysterectomy rates were more than fivefold and other abdominal–pelvic surgeries were more than threefold increased in the DGBI groups. This could derive from a limitation of our study, not collecting information on coexisting gynaecological pathology (ie, endometriosis).
Our data have reiterated the existing findings in literature about the significant burden these conditions carry. Despite of the significant extra costs and additional procedures, the quality of life of people with IBS and FD in the general population remains poor and their condition poorly understood.6
The main limitations of our study derive from its design. An anonymous cross-sectional internet based survey relies completely on the honesty and recall of the individual. Computer literacy can be a limiting factor in certain age groups. Investigators had no access to medical records and could not perform tests in order to ascertain diagnoses. However, excluding individuals reporting medical history suggestive of organic reasons behind GI symptoms from DGBI diagnosis analysis groups compensated for this to some degree. Nonetheless, it is likely that some inaccuracies in diagnostic classification resulted from this.
The outbreak of the COVID-19 pandemic reached global proportions soon after the launch of the study in December 2019. Gibraltar, due to its somewhat isolated position, emerged relatively unscathed from the first wave of the pandemic, thanks to the rigorous public health measures introduced. When numbers of infections started to increase again in November 2020, we decided to close data collection to avoid any interference.14
This first-ever population-based study of Rome IV defined IBS and FD in Gibraltar indicates that the prevalence rates of these disorders are similar to the recently reported data for the UK and Spain. These disorders represent a significant burden on the healthcare system due to multiple doctor visits, increased use of prescription medications and frequent surgical procedures. Due to their poor diagnostic recognition, most of the healthcare costs will remain ill placed as reflected by the poor quality of life scores. The study highlights the need for further medical education and urges imminent practice changes in line with the available guidance policies. The wide spectrum of clinical presentations and overlapping nature of these disorders will need to channel management from sole practitioners to specialist multidisciplinary teams able to offer the required standard of care.
Since most of these results have been mirrored by findings from other countries, the problems here highlighted are generalisable.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
The Gibraltar Medical Ethics Committee approved this study on 16 October 2019. There is no reference or ID number on the approval. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
Authors are grateful to the Rome Foundation Mentorship Program. Special thanks to Dr Gustavo Camino, Clinical Psychologist, Mental Health Department, Gibraltar, Dr Sohail Bhatti, former Director of Public Health, Gibraltar and his colleagues for their support and Victor Elliot and Shayla Rosa, student nurses at University of Gibraltar, School of Health Studies for their work.
Footnotes
Contributors DBK: guarantor, planned the study, conducted survey, wrote and submitted the manuscript. AS: conducted survey, helped with data collection. AGH: statistical analysis, illustrations. OP: planned the study, designed webpage for data collection, corrected manuscript, provided mentorship.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.