Article Text

Abstract
Objective Despite international guidelines recommendations to use mortality as a quality criterion for gastrointestinal (GI) procedures, recent studies reporting these data are lacking. Our objective was to report death causes and rate following GI endoscopies in a tertiary university hospital.
Design We retrospectively reviewed all GI procedures made between January 2017 and December 2019 in our tertiary hospital in Switzerland. Data from patients who died within 30 days of the procedure were recorded.
Results Of 18 233 procedures, 251 patients died within 30 days following 345 (1.89%) procedures (244/9180 gastroscopies, 53/5826 colonoscopies, 23/2119 endoscopic ultrasound, 19/911 endoscopic retrograde cholangiopancreatography, 6/197 percutaneous endoscopic gastrostomies). Median age was 70 years (IQR 61–79) and 173/251 (68.92%) were male. Median Charlson Comorbidity Index was 5 (IQR 3–7), and 305/345 procedures (88.4%) were undertaken on patients with an ASA score ≥3. Most frequent indications were suspected GI bleeding (162/345; 46.96%) and suspected cancer or tumourous staging (50/345; 14.49%). Major causes of death were oncological progression (72/251; 28.68%), cardiopulmonary failure or cardiac arrest of unkown origin (62/251; 24,7%) and liver failure (20/251; 7.96%). No deaths were caused by complications such as perforation or bleeding.
Conclusions Progression of malignancies unrelated to the procedure was the leading cause of short-term death following a GI procedure. After improvements in periprocedural care in the last decades, we should focus on patient selection in this era of new oncological and intensive care therapies. Death rate as a quality criterion is subject to caution as it depends on indication, setting and risk benefit ratio.
- endoscopic procedures
- endoscopic ultrasonography
- endoscopic retrograde pancreatography
- endoscopy
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as online supplemental information. All data relevant to the study are included in the article or uploaded as online supplemental information. Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
International guidelines recommend using mortality as a quality criterion for gastrointestinal (GI) procedures.
Recent tertiary hospital data on causes of death after GI procedures are lacking.
WHAT THIS STUDY ADDS
Mortality after GI endoscopies in a tertiary centre is around 2%.
Progression of underlying malignancies is the major cause of short-term death after GI procedures.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
In this era of new oncological therapies, improvements in patient selection criteria for GI procedures is needed.
Introduction
Gastrointestinal (GI) endoscopies are considered to be safe investigations and are widely used as diagnostic and therapeutic interventions for many pathologies. Many indicators of harm and benefit of GI endoscopies are used such as patient satisfaction, fulfilment of procedure objective and number of complications among others.1 Mortality is the rarest and most feared adverse event. Current guidelines from the European Society of Gastroenterology Endoscopy,2 the British Society of Gastroenterology3 and the American Society of Gastroenterology4 suggest using mortality as one of indicators of quality standards for GI procedures. Due to the ageing population with many comorbidities, high-risk procedures are now occurring at a greater frequency. In the literature, mortality depends mostly on indication, setting and type of procedure. It can be as high as 10% during a hospital stay after oesophagogastroduodenoscopy (EGD) for upper GI bleeding5–8 or as low as 0.13% in the 30 days following a colonoscopy for colorectal cancer screening.9 As risk and benefit profiles are heterogeneous, acceptable mortality depends on many factors and needs to be defined for each indication, setting and procedure. Events leading to death can be related to the endoscopy itself such as perforation and bleeding, to sedation such as cardiovascular and pulmonary incidents, or be unrelated to the procedure and due to the underlying disease such as malignancy, liver failure or preexisting GI bleeding.10 11 In 1995, the prospective audit of endoscopy-related deaths by the British Society of Gastroenterology revealed cardiopulmonary complications as the most prominent cause of deaths.12
However, except for several pathologies such as GI bleeding, only few studies report these data, and distribution of causes of death are still not clearly described. In addition, recent studies on mortality in tertiary centre are lacking. Our aim was to review and describe all patients who died within 30 days of an endoscopic procedure in a tertiary hospital.
Methods
Study design
The design was a retrospective monocentric study conducted in a tertiary care hospital in Geneva (Geneva University Hospitals, Switzerland). All EGD, colonoscopies, percutaneous endoscopic gastrostomies (PEG), endoscopic retrograde cholangiopancreatography (ERCP) and endoscopic ultrasounds (EUS) carried out between 1 January 2017 and 31 December 2019 were reviewed in our electronic health record which identified deceased patients using a filter. Date of death in the medical files was used to select patients who died in the 30 days following a procedure. Occurrence and date of death in Geneva University Hospitals is linked to the Swiss civil registration. For the years 2020 and 2021, patients were not included due to the COVID-19 pandemic.
Data collection
Data of patients who died within 30 days of a procedure were collected from their in-hospital computerised medical records. In line with the Swiss health insurance system, all in-hospital diagnoses are coded according to the International Classification of Diseases 10th revision. Demographic data, comorbidities, Charlson Comorbidity Index (CCI) and American Society of Anesthesiologists (ASA) score were collected. A diagnosis or comorbidity was considered to be present when mentioned in the last discharge summary or in the admission note. Procedure-related data such as indication, date of procedure, endoscopist and therapeutic procedure were recorded from the endoscopic information database (ENDOBASE, Olympus). The cause of death was taken from the medical records. Oncological progression cause of death was retained when death was caused by tumourous obstruction (biliary, GI, airway or vascular), compression (central nervous system, vascular or airway) or bleeding. Death of patients who were transferred to a palliative care unit due to an untreatable cancer was considered as caused by the malignancy.
Based on the WHO guidelines, alcohol consumption was defined as medium or high risk if the quantity ingested was more than 40 g/day for men and more than 20 g/day for women. When available in the medical file, the Mini–Mental State Examination and Nutritional Risk Screening 2002 score were extracted. Haemodialysis was defined as acute when initiated during the same hospital stay and chronic when the patient was on dialysis (peritoneal or haemodialysis) in an ambulatory setting prior to hospitalisation.
Examination characteristics, diagnostic presumption, final diagnosis, use of an anaesthesiologist or intensivist, use of vasopressors, and type of anaesthesia were recorded. Emergency status was defined by the physician in charge of the patient who qualified the procedure as urgent (within 48 hours), as soon as possible (non-elective, performed during hospitalisation) or elective (prescription made prior to hospitalisation or in ambulatory care). The time of the examination occurred during working hours on weekdays or outside of working hours at night-time and on the weekend; in the latter case, the gastroenterologist was called by an emergency doctor, intensivist or physician of another specialty.
Statistical analysis
Data were analysed with Excel (Microsoft Excel V.16.43.1). Qualitative data were described as frequencies and percentages, and quantitative data as medians and QRs.
Results
Out of 18 233 procedures performed between 1 January 2017 and 31 December 2019, 251 patients died within 30 days after a total of 345 (1.89%) endoscopies.
Patient demographics and comorbidities
Patients were mostly male (173/251; 68.92%) with a median age of 70 years (IQR 61–79). Two-thirds of patients were active (88/251; 35.05%) or former smokers (74/251; 29.48%) with a median pack year of 40 (IQR 30–60). A significant proportion of patients had moderate-risk or high-risk alcohol consumption (103/251; 41.04%). Most patients underwent only one procedure (186/251; 74.10%), while 18 patients had three or more procedures (7.17%).
Overall, patients had many comorbidities with a CCI of 5 (IQR 3–7), with 120 patients (47.81%) having a CCI ≥6. The most frequent comorbidities were hypertension (145/251; 57.76%), oncological or haematological disease (126/251; 50.20%), hypercholesterolaemia (80/251; 31.87%), and liver disease (80/251; 31.87%). Among patients with a malignancy, 70/126 (55.55%) had metastatic disease, 44/126 (34.92%) a single tumourous lesion and 12/126 (9.52%) haematological disease. All comorbidities and malignancy diagnoses are detailed in table 1.
Patient demographics and comorbidities
Procedure characteristics and settings
The most frequently performed procedure was EGD (244/345; 70.72%), followed by colonoscopies (53/345; 15.36%), EUS (23/345; 6.67%), ERCP (19/345; 5.51%) and PEG (6/345; 1.74%) (table 2).
Characteristics of examinations
Procedures were mostly performed on weekdays in working hours (295/345; 85.55%). Just under half of examinations were performed by trainees (168/345; 48.69%). Thirteen interventions were performed in an outpatient setting (13/345; 3.77%): 12 EGD and 1 EUS with fine-needle aspiration (FNA). Three of these procedures were performed in the emergency department, with patients being discharged on the same day.
Concerning inpatients, 136/345 (39.42%) were hospitalised to undergo the endoscopy, with 113/345 (32.75%) in an urgent setting and 23/345 (6.67%) on an elective basis. Most frequently, patients were hospitalised in intensive care units (75/345; 21.74%).
Anaesthesia
Overall, 218 patients had an ASA score ≥3 (86.85%). Four patients (1.59%) were treated by extracorporeal membrane oxygenation (ECMO) or extracorporeal circulation (ECC), while 12 (4.8%) had acute renal failure requiring dialysis.
Sedation was the most frequent type of anaesthesia performed in our centre (159/345; 46.09%), mostly with propofol. Oxygen supplementation was given to all patients with sedation or general anaesthesia. An anaesthesiologist or an intensivist was present during 276/345 procedures (80.0%). Out of the 167/345 (48.41%) procedures performed under general anaesthesia with mechanical ventilation, 40/167 (23.95%) were necessary for other reasons such as septic shock (7/40; 17.50%), postcardiopulmonary resuscitation (7/40; 17.50%), cardiovascular failure (6/40; 15.00%) and liver failure with multiorgan failure (4/40; 10.00%). Because of the high anaesthetic risk or lack of an available anaesthesiologist, 19/345 procedures (5.51%) were performed without sedation, including two incomplete colonoscopies that were interrupted due to anal and abdominal pain.
Procedure indications and type of therapeutic procedures
Suspicion of GI bleeding (161/345; 46.67%) was the leading indication and the purpose of 136/244 EGD (55.74%) and 25/53 colonoscopies (47.16%). The three most frequent diagnoses of EGD made for suspicion of GI bleeding were peptic ulcer (34/244; 13.93%), variceal bleeding (21/244; 8.61%) and portal hypertensive gastropathy (6/244; 2.46%). In 44/244 cases (18.03%), no upper GI of bleeding was found and in 7/244 cases (2.87%) bleeding sequelae was found without source identified. Other causes of upper GI bleeding were angiodysplasia or gastric antral vascular ectasia (4/244; 1.64%), neoplasia (4/244; 1.64%), oesophagitis (4/244; 1.64%), ischaemia (4/244; 1.64%), nasogastric tube lesion (4/244; 1.64%), Mallory-Weiss syndrome (2/244; 0.82%), Dieulafoy lesion (2/244; 0.82%) and lesion secondary to transoesophageal echocardiography (1/244; 0.41%).
A total of 50 examinations (50/345; 14.49%), including 28 EGD (28/244; 11.47%), 13 colonoscopies (13/53; 24.53%), 2 EUS (2/7; 28.57%) and 7 EUS with FNA (7/17; 41.17%), were performed for tumourous investigation or staging. Screening or control of oesophageal varices after ligation (38/345; 11.01%) and biliary obstruction (30/345; 8.69%) were the other major reasons for undergoing the procedures. All indications and therapeutic procedures are detailed in table 3.
Diagnosis of suspicion with the number of confirmed diagnoses, therapeutic interventions and examinations not completed for safety or technical reasons by type of procedures. Percutaneous Endoscopic Gastrostomies are not shown in this table.
Therapeutic procedures were undertaken in 96/244 EGD (39.34%) and 12/53 colonoscopies (22.64%). Coagulation, clipping or ligation made up for 70.83% of the EGD (68/96). The other therapeutic EGD were oesophageal or duodenal stent placement (12/96; 12.50%), nasogastric tube insertion (8/96; 8.33%), dilation or botox injection (3/96; 3.12%), food disimpaction (2/96; 2.08%) and polyp resection (1/96; 1.04%). Exsufflation (5/12; 41.66%), coagulation (3/12; 25.00%), polyp resection (2/12; 16.67%), colonic stent placement (1/12; 8.33%) and stent removal (1/12; 8.33%) were therapeutic procedures made during colonoscopies. One hundred and fifty EGD and 41 colonoscopies were only diagnostic. During the 24 ERCP, biliary stent placement (11/24; 45.83%) and biliary lithiasis extraction (9/24; 37.50%) were made.
Incomplete examinations
Twenty examinations (5.80%) were incomplete due to technical or safety issues. The diagnosis of suspicion for these incomplete examinations are described in table 3. Almost one-fifth of colonoscopies (9/53; 16.98%) were interrupted due to insufficient bowel preparation (7/53; 13.21%) or pain during the examination with a contraindication to sedation (2/53; 3.77%). Seven EGD (7/244; 2.86%) were not performed due to the presence of food in the stomach (4/244; 1.64%), agitation (1/244, 0.41%), oesophageal stenosis (1/244; 0.41%) and intractable gag reflex despite sedation (1/244; 0.41%). Two EUS (2/24; 8.33%) were impossible to complete due to altered anatomy (1/24; 4.17%) or the presence of food in the stomach (1/24; 4.17%), while two ERCP (2/24; 8.33%) were impossible due to extrinsic and intrinsic duodenal compression or tumourous stenosis.
Characteristics and causes of death
Of the 251 patients who died, GI malignancy progression was the major cause of death (45/251; 17.93%). All other causes of death are described in detail in table 4.
Cause of death by type of procedure
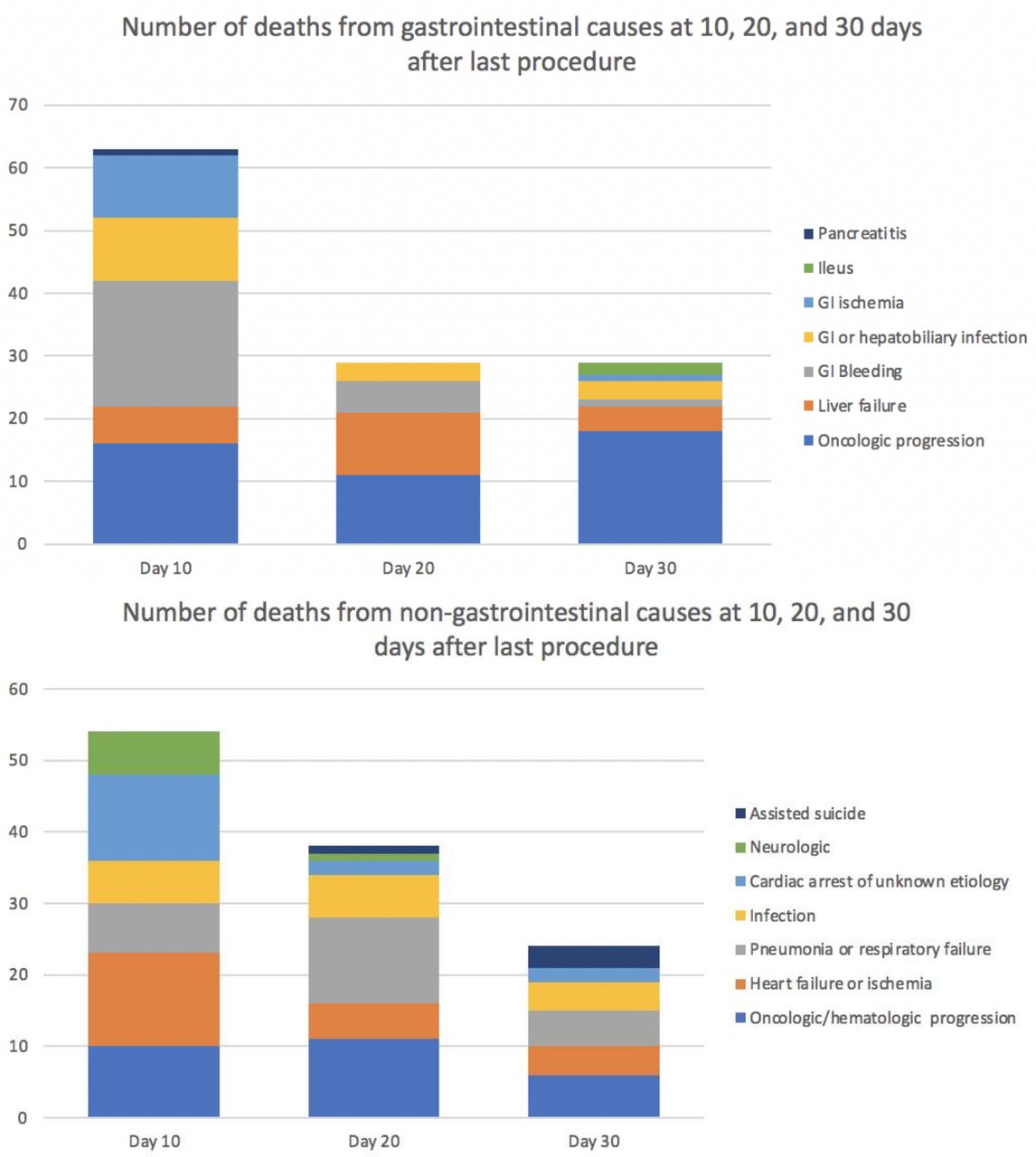
Twenty-five (25/38; 65.79%) deaths from heart failure, myocardial infarction or cardiac arrest of unknown origin, occurred within 10 days of the last procedure and 9 (23.68%) within 48 hours. Deaths due to pneumonia mostly occurred between 10 and 20 days after the last procedure (12/24; 50%). Of the neurological causes, 4 deaths due to cerebrovascular accidents occurred during the first week after the endoscopy. Two other neurological deaths were linked to cardiac arrest and massive stroke that occurred before the endoscopy (figure 1A,B) and the last was due to an unknown origin loss of consciousness. Six patients (6/251; 2.39%) died on the same day as the endoscopy: two from GI bleeding, two from GI ischaemia, one from cardiac arrest of unknown origin and one from sepsis.
{kind=link}
Number of death from gastrointestinal (top) and non-gastrointestinal (bottom) causes at 10, 20 and 30 days after last procedure. GI, gastrointestinal.
The majority of patients (195/251; 77.69%) died during the same hospital stay, 37/251 patients (14.74%) died after a new admission and 18/251 patients (7.17%) died in the community or in another hospital.
Death rate by examinations
In relation to the total number of procedures, the 30-day mortality rate was the highest among patients who had a PEG (6/197, 3.05%), followed by EGD (244/9,180, 2.66%), ERCP (24/911, 2.63%), EUS with FNA (7/354, 1.98%), EUS (17/1,765, 0.96%) and colonoscopy (53/5,826, 0.91%).
Discussion
To the best of our knowledge, this is the first study to report 30-day mortality following GI endoscopies in a tertiary hospital. As mortality occurrence and date is linked to administrative civil registration, our study data are reliable. The mortality rate was low (1.89%) but more than twice as high as the 30-day mortality of all patients who went to the recovery room of our hospital after surgical or non-GI endoscopic procedures (0.8%). In our study, the majority of patients were elderly males with many comorbidities. Cirrhosis was one of the most frequent comorbidities along with hypertension and neoplasia. Alcohol consumption was frequent due to the higher risk for GI and liver pathologies. The highest mortality rate was observed after PEG insertion, mostly due to the patients’ comorbidities and the prognosis of the underlying disease, such as neurological diseases.
Of the 251 patients, no deaths were caused by haemorrhagic shock or GI tract perforation caused by the procedure. A proportion of the 66 deaths due to pneumonia, respiratory failure, myocardial infarction, cardiac arrest or cerebrovascular accident could have been precipitated by endoscopy or anaesthesia. However, due to the absence of a control group, this exact proportion is unknown.
Interestingly, neurological deaths and most cardiovascular deaths occurred within 10 days of the last procedure, and most of the pneumonia and respiratory failure deaths within 20 days. Twenty-two procedures of these 66 patients were elective due to the clinical stability of the patient or the non-urgent indication, suggesting that the procedure itself could have been a precipitating factor. One of the four patients who died of a cerebrovascular stroke had an anticoagulation withhold for an ERCP procedure.
In contrast to older12 publications and in line with more recent ones,13 14 cardiopulmonary deaths are less frequent compared with those associated with the progression of underlying malignancies. Preprocedural evaluation with improved knowledge of anaesthetic risks, intraprocedural and postprocedural patient monitoring could have contributed to this change.15 However, presence and availability of an anaesthesiologist and type of sedation is heterogeneous between countries and hospitals.16–18 Most frequently in Switzerland19 and in our hospital, endoscopists are solely responsible for anaesthesia and can use propofol for patients with ASA score 1 or 2 and low risk procedures. An anaesthesiologist is present for ASA scores 3 and 4 patients or for high-risk procedures such as foreign body removal or upper GI bleeding. In our study, due to high ASA scores and numerous critically ill patients, anaesthesia was undertaken by anaesthesiologists or intensivists in 80% of procedures. As anaesthesiologists cannot be present for all endoscopies, especially in private practice,16 careful preprocedural anaesthetic risk evaluation is mandatory. For ASA 1 and 2 scores patients, studies showed safe non-anaesthesiologist-administered propofol with no increase in cardiopulmonary events.17 19–21
New chemotherapies and immunotherapies that improve the prognosis of oncological patients could encourage us to perform invasive procedures later in the oncological course. By the definition, we used for the oncological cause of death, we excluded as much as possible patient who died from a procedure complication. However, for few causes such as pneumonia in pulmonary cancer or bacterial translocation in GI cancer, the procedure could have hastened the death. In our study, the diagnosis of malignancy was known before the endoscopy in 38/82 (46.34%) of patients who died of an oncological or haematological cause. Among them, 21/38 (55.26%) were at a metastatic stage. Thus, as described by other authors,22 some procedures could seem excessive or even futile as oncological mortality might reflect an expected disease progression. Similarly, we performed six endoscopies in four patients with ECMO or ECC. In such cases, patient survival depends mostly on the underlying disease and the selection of patients by intensivists and/or oncologists. Due to the existence of new therapeutics in non-GI specialties, it is becoming increasingly difficult for on-call GI physicians to evaluate and individualise the benefits of an endoscopy. This study highlights the role of the GI physician in informing patients and families about the risks and the importance of a multidisciplinary approach to select the patients who will benefit from a GI procedure, especially in oncology and geriatrics.
A remarkable aspect of our study is the proportion of incomplete colonoscopies due to insufficient bowel preparation. It has been described in previous studies and observed in the practice of every GI physician that old age, severe illness, hospitalisation and many comorbidities are risk factors for insufficient bowel preparation.23 In our study, the three most frequent causes of death after colonoscopy were congestive heart failure or myocardial infarction, cardiac arrest of unknown origin and pneumonia. As previously described, these causes point to the potentially deleterious effect of the procedure. Indeed, more than other procedures, the risk of colonoscopies frequently outweighs their benefit due to the proportion of non-contributive examinations in old or frail patients. For these patients, a CT colonography should be favoured to avoid anaesthetic risk. However, in our study, most frequent colonoscopy indications needed a potential therapeutic procedure (25 GI bleeding, 3 volvuli) or biopsies (2 colitis). For 13 tumourous suspicion indications, only 3 colonoscopies found a tumourous lesion, 3 had an insufficient bowel cleansing and 7 had no lesion. This suggests that CT colonography could have been used as a first step in those patients to avoid deleterious anaesthetic effect and select patient who have a higher benefit of colonoscopy for biopsies.
In previous data and according to a meta-analysis published in 2016, the pooled 30-day PEG mortality rate was reported to be 5.5%, which is similar to our data.24–26 In our unit, as shown by Stein et al,27 the 30-day mortality rate after PEG insertion has decreased in the last decade. In comparison, in 2011 and 2012 in our centre, 122 PEG were performed with a 30-day mortality rate of 8.96% (12/122) (personal data) compared with 3.05% in this study despite a stable number of PEG insertions (65.6 per year in 2017–2019 vs 67 per year in 2011–2012) and the use of the same insertion technique.26 The cause of this change remains elusive to us. It is most probably due to a better selection of patients and an improvement in the information given to our colleagues of other specialties as well as to patients and their families about the low benefit–risk ratio of PEG insertion in the presence of specific conditions such as dementia. In our hospital, nutrition team is usually not involved in the decision. Multidisciplinary discussion with nutritionist could further improve patient selection.
Mainly, indications for the procedures (table 3) are justified and reasonable. However, high number of comorbidities, proportion of incomplete colonoscopies and oncological progression as the leading cause of death suggest that selection of patients could be improved. As this study is undertaken in a tertiary hospital, it reflects a selection of patients who are frail and comorbid. However, death rate for other anaesthetic procedures (0.8%) including high risk cardiac, neurological and thoracic surgeries, is much lower than after GI procedures. Thus, to lower the postprocedural mortality in tertiary hospitals, patient selection could be the most efficient one. Now, prospective studies including all patients who undertake a GI procedure are needed to identify risk factors.
The main limitation of our study is its retrospective data collection and the absence of a control group. Due to its retrospective nature and the high number of other procedures, comparisons with patients who did not die were not possible. This feature reflects the complexity of recording mortality data in each hospital. Despite the relevance and recommendation regarding the collection of precise data on mortality as an indicator of quality standards for endoscopies, it is rarely performed due to the physicians’ lack of time and the high number of patients seen in GI units for short procedures. This highlights the necessity for hospitals to implement a system for the automatic collection of data in a prospective manner. Added to the retrospective manner, our data are subject to caution as the single centre setting can induce patient selection biases.
Another limitation is the small sample size for certain type of procedures. As our aim was to evaluate death during 3 years after every procedure, EUS and ERCP had a small occurrence of death. It is thus difficult to conclude on mortality after such procedures, and more studies are needed.
As mortality is a rare adverse event, especially in non-tertiary hospital, information about death causes is less useful for the majority of gastroenterologists in private practice. In other settings, other quality markers such as patient satisfaction, adenoma detection rate, unplanned adverse events and appropriateness of procedure indication should be used on daily basis.1 28
As our data are from a tertiary transplant hospital, they cannot be extrapolated to other practice settings. Given that patient deaths are mostly caused by underlying diseases, the mortality rate of GI endoscopies is strongly dependent on the expertise of other specialties. This study emphasises the difficulty of using the mortality rate as an indicator of quality standards.
Conclusion
In our study, we showed that the progression of underlying malignancies unrelated to the procedure was the leading cause of death in the 30 days following a GI endoscopy in our tertiary hospital. Following various improvements in anaesthesia and monitoring in the last decade, we should focus our attention on oncological patients and define who can benefit from endoscopies in this era of new chemotherapies and immunotherapies. All conditions that put patients at high anaesthetic risk should be reviewed by the gastroenterologist and, if in doubt, an anaesthesiologist should be sought to evaluate the need of an anaesthesiologist for the procedure. Gastroenterologists must discuss with physicians of other specialties, patients and families about the risk and benefit profiles, which are very heterogeneous due to different settings and indications. However, more prospective studies from tertiary hospital are needed to identify risk factors to improve the patient selection.
As the underlying pathologies of patients and the hospitalisation setting seem the most important factors leading to death, this suggests that the use of the mortality rate as a quality standard indicator for GI procedures is subject to caution, as it depends mostly on other specialties and the types of patients hospitalised in each centre.
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as online supplemental information. All data relevant to the study are included in the article or uploaded as online supplemental information. Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval was given by the Cantonal Commission for Research Ethics in Geneva, Switzerland, in agreement with the amended Declaration of Helsinki.
References
Footnotes
Contributors OC: collected the data, conceived and designed the analysis, interpreted the data, performed the analysis, wrote the paper, LS: collected the data, reviewed and edited the paper. PB: collected the data, reviewed and edited the paper, LB: conceived and designed the analysis, NG: collected data and contributed data analysis, CB: collected data, J-LF: Guarantor of the study, conceived and designed the analysis, interpreted the data, wrote and edited the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.