Article Text

Abstract
Objective We aimed to study the prevalence of achlorhydria (AC) in a large Asian population.
Design Medical records of patients who underwent oesophagogastroduodenoscopy (OGD) with Congo red staining method at the Vichaiyut Hospital from January 2010 to December 2019 were retrospectively reviewed.
Results A total of 3597 patients was recruited; 223 were excluded due to concurrent use of proton pump inhibitors. Eighteen from 3374 patients (0.53%) had AC. Seven patients were presented with permanent AC (5F, 2M) (median age=69 years; range 58–92). Among 11 patients with temporary AC (5M, 6F: mean age 73.4 years; SD 13.2 years), all had gastrointestinal Helicobacter pylori bacterial infection and were over 45 years old. After successful treatment for H. pylori, AC was absent among patients with temporary AC. If counting only patients over 45 years of age, the prevalence of AC was 0.68% (18/2614). No adverse events arising from Congo red occurred.
Conclusion AC is relatively rare. Permanent and temporary AC were found only when they were over 55 and 45 years old, respectively. Staining Congo red on gastric mucosa can be safely and routinely incorporated into the OGD procedure for early detection of AC. We recommended a low-cost screening test such as serum vitamin B levels for screening only in patients aged 50 and over.
- endoscopy
- gastric acid secretion
- anemia
- gastrointesinal endoscopy
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Achlorhydria (AC) is relatively rare.
Prevalence of AC has been reported in only small and selective samples of patients.
Early detection of AC can prevent irreversible brain damage from pernicious anaemia which can lead to irreversible neurological deficit.
Gastroscopy has been increasingly used worldwide.
Congo red testing during gastroscopy can be simply used to identify AC on-site.
WHAT THIS STUDY ADDS
In our study, AC is only present in patients over 45 years of age.
Our prevalence of AC from a large Asian population is demonstrated to be rarer than previously reported from Western country.
Systematic use of Congo red testing during oesophagogastroduodenoscopy can be done with little to no extra burden or adverse events as shown by two-decade procedural implementation.
All patients with permanent AC in our study were aged 55 years or older at the time of diagnosis.
Given the low prevalence of the AC, although it can cause a serious complication, we recommend a low-cost screening test such as serum vitamin B12 levels for screening only in patients aged 50 and over.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE, OR POLICY
This present study shows that AC is rare, seen only in patients over 50 years of age. Screening is quick and easy with the Congo red test during an upper gastrointestinal endoscopy. The information from this current study is therefore one of the important pieces of information to be taken into consideration regarding screening policy for the disease: should doctors consider screening methods for this disease in the future? To our knowledge, no study of the disease in such a large number of Asian ethnicities has been reported before.
Introduction
Achlorhydria (AC) refers to a state in which the stomach is unable to produce hydrochloric acid, which is a significant component of gastric secretions produced by the stomach. The acid digests food and protects the body from foodborne pathogens. Gastric acid are fluids secreted by the stomach, consisting of hydrochloric acid, potassium chloride and sodium chloride. Parietal cells lining the stomach wall are the cells responsible for producing gastric acid. Various factors can damage these cells include surgery, bacteria (Helicobacter pylori), medication and certain antibodies which may lead to AC among patients.
AC can be categorised into two groups based on its causes: (1) permanent achlorhydria (permanent AC), whose condition is irreversible; and (2) temporary achlorhydria (temporary AC), whose cause or association with certain diseases can be cured. One example being infection with H. pylori in the stomach and using a proton pump inhibitor.
AC can lead to several diseases or conditions. One condition is pernicious anaemia (PA) where the process of vitamin B12 absorption has been altered. The presence of PA leads to irreversible neurological deficits, which includes the following neurological symptoms: personality changes, cognitive impairment, paresthesia, psychosis, dementia, weakness of muscle, paraplegia and urinary incontinence. Detecting AC is crucial since remedies are often available.
Diagnostic techniques for AC can be performed in a number of ways. One simple method is to diagnose while the physician is performing an oesophagogastroduodenoscopy (OGD). This method involves staining Congo red on the gastric mucosa. Congo red is pH sensitive and changes its colour from red to dark blue or black in an acidic environment which is the body’s normal condition. When patients have AC, Congo red does not change colour. Staining the gastric mucosa only takes a few additional minutes during OGD. Congo red can be completely washed off with normal rinse. The use of dye in the digestive tract is not harmful to the body.
In this current study, researchers collected data from a large referral hospital in Thailand which has incorporated Congo red staining of gastric mucosa as protocol during OGD since 1998. The procedure was performed in all patients who had undergone OGD with no contraindications for the use of Congo red for staining of gastric mucosa. The primary objective is to determine the prevalence of AC among this population with a secondary objective to identify the clinical features of patients with AC. Ascertainment of the likely cause of AC in each patient will also be investigated.
Methods
Medical records inspection
This study conducted a large single-centre retrospective examination of medical records of patients that underwent OGD at Vichaiyut Hospital in Bangkok, Thailand from January 1998 to December 2019. Inclusion criteria were patients undergoing successful OGD by means of various indications and staining of gastric mucosa with Congo red. Exclusion criteria were patients taking either a proton pump inhibitor or histamine receptor antagonist within 2 weeks before the procedure. For patients with positive Congo red results, researchers conducted a comprehensive review of patient data including the results of the OGD, results of gastric mucosa staining and clinical background information. The data were then summarised and analysed. The protocol was approved by the Ethics Committee of the Vichaiyut Hospital.
Procedure for detection of AC using Congo red
While performing the routine OGD, the following sequence of steps are taken. The physician inserts a gastroscope into the patient’s upper digestive area to check the mucosa of the stomach and duodenum to determine if there are cancerous or non-cancerous lesions. A small tube is then inserted through the instrument channel of the gastroscope to protrude into the stomach area. A 10 cc syringe containing Congo red paint is sprayed through the rubber tube on the gastric mucosa in the body of the stomach. Through visual identification, any colour change of the gastric mucosa is identified. The diagnostic criterion for AC is no change in the colour of Congo red (figure 1). If Congo red is exposed to acidic conditions, the colour will change from red (pH 5.0) to dark blue or black (pH 3.0) (figure 2; online supplemental videos 1 and 2, respectively).
Supplementary video
Supplementary video

Congo red does not change its colour because there is no acid on gastric mucosa.

Congo red changes its colour from red to dark blue or black in an acidic environment.
Monitoring and isolating patients with AC
According to protocols at Vichaiyut Hospital, patients confirmed with AC were advised that determination of the cause according to clinical information from history taking, physical examination and further inspection would be undertaken. Physicians would also recommend for patients to attend regular follow-up appointments to treat AC and its underlying causes. Further inspection recommended by the physician included pathological examination of the gastric mucosa, gastrin level, H. pylori infection and vitamin B12 blood test.
Results obtained from the examination and extracted from the patient records were studied by the researchers. The patients were divided into two groups: the first group included patients with permanent AC. Due to the unknown aetiology of permanent AC, this group of patients was treated with vitamin B12 to prevent complications such as neurological deficits and anaemia. The second group included patients with temporary AC who were treated and received follow-up examinations to determine if AC and the diseases which caused it had improved. If the physician was unable to treat the cause of the disease or the treatment took a long time, the physician would also treat AC with B12 supplements to prevent complications from such a condition.
Statistical analysis
The researchers presented demographic and clinical characteristics of individuals found with AC using counts and percentages. Prevalence calculations are presented as a number and percentage. No statistical tests were performed.
Results of study
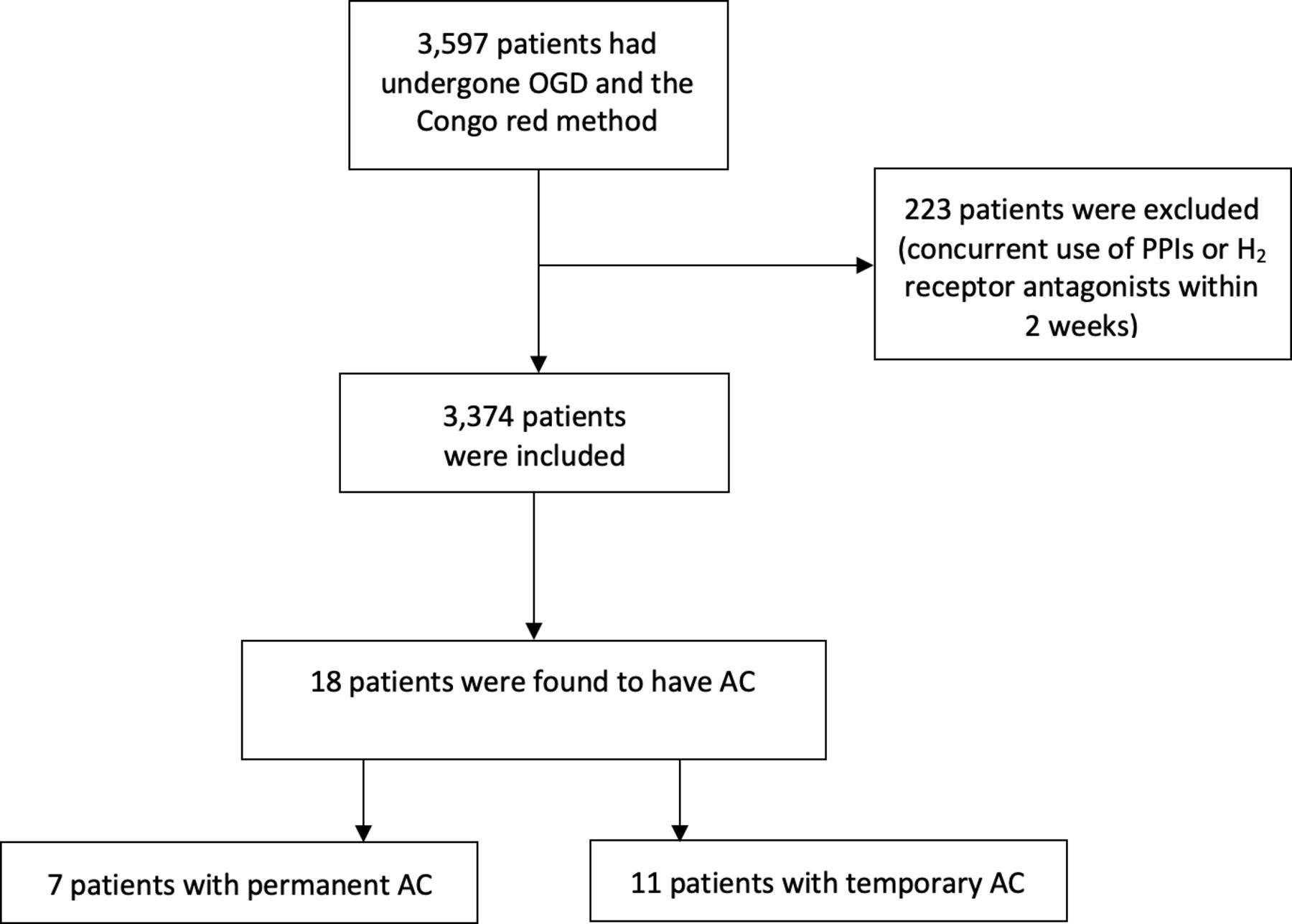
A review of medical records at Vichaiyut Hospital from January 1998 to December 2019 revealed that a total of 3597 patients had undergone OGD and the Congo red method. All patients met the inclusion criteria; 223 were excluded due to concurrent use of proton pump inhibitors or histamine receptor antagonists within 2 weeks before the procedure. Eventually, 3374 were recruited in the study. A total of 18 patients were found to have had AC, 7 of whom were categorised as permanent AC and 11 as temporary AC. The total prevalence of AC among subjects was 0.53% (18/3374) (figure 3)
{kind=link}
{kind=link}
{kind=link}
Diagram showing flow and number of patients involved in this current study. AC, achlorhydria; OGD, oesophagogastroduodenoscopy; PPI, proton pump inhibitor.
Clinical data on the seven patients with permanent AC are shown in table 1.
Characteristics of patients with permanent AC
Five of the seven patients (71.4%) with permanent AC were women and two (38.6%) were men. The mean age of patients at diagnosis time was 74.6 years (SD 11.9). The second patient who tested positive for H. pylori infection was categorised as having permanent AC since AC could still be detected after successful treatment for H. pylori. All patients were found to have high levels of serum gastrin (median=3000 pg/mL; range=1300–3000 pg/mL). All patients in this group were confirmed with intestinal metaplasia from pathological results from the gastric mucosa (table 2).
Light microscopic finding among patients with permanent AC
Clinical data on the 11 patients with temporary AC are shown in table 3.
Characteristics of patients with temporary AC
Five were men (45%) and six were women (55%). Patients had a mean age of 73.4 years (SD 13.2 years). All patients in this group had gastrointestinal H. pylori bacterial infection while being examined with Congo red. After treatment for H. pylori, patients were re-examined with Congo red and AC was absent.
After completing an OGD at Vichaiyut Hospital, a follow-up typically would occur 1 day after a procedure was performed. The patient would either meet the physician or would be contacted via telephone by the nursing team or medical personnel to monitor their condition. Review of all data found that no patients had complications arising from the Congo red procedure in this study.
Discussion
The present study included a large number of subjects from a single institution over a period of 10 years. To our knowledge, this present study has the largest number of participants. Past studies have a smaller population. Demographics tend to be niche populations that are more likely to be AC than the general population. It is therefore not surprising that the prevalence of AC in this current study was lower than that reported in other previous studies such as a prospective survey by Carmel et al that was conducted to determine cobalamin levels and anti-intrinsic factor antibodies in 729 people who were over 60 years of age. It was found that 14 of them were present with PA, which accounts for 1.9%. Most of the patients were asymptomatic with no anaemia.1 Bins et al studied a blood test for serum gastrin levels after patients had been fully stimulated with pentagastrin. In the diagnosis of AC in the Bins et al study, the prevalence of AC was found to be 2.5%.2 A prospective survey by Carmel et al was conducted to determine cobalamin levels and anti-intrinsic factor antibodies in 729 people who were over 60 years of age. It was found that 14 of them were present with PA, which accounts for 1.9%. Most of the patients were asymptomatic with no anaemia.3 In the Jacobson et al study, the type of population was patients with autoimmune disease.4 The prevalence of AC from other studies has been estimated at 2%, while the prevalence of permanent AC in this study was 0.19%, a rate 10 times smaller. The reason for such a difference is that the types of studies and population were different, especially in terms of the groups or characteristics of the population who participated in the study.
Ethnicity is likely another factor since Asians have been found to have a lower prevalence of AC than other races according to past studies and our study was exclusively an Asian population. Data indicate that the prevalence of the disease varies between races. In a study of 156 patients in Europe, 73 patients were European in origin, mean age among black women (53±1) was lower than that of all the others, and another study found that Latin-American people with pernicious anaemia were both significantly younger than white men and women.1 5
One interesting information from the results of this study is that permanent AC is found only in the population aged 55 years and over, but including temporary AC, it is found only in the population aged 45 and over. This is an important issue because if we look at PA as a disease that causes disability and may be the cause of death, and if we can diagnose in the first place before the patient has consequences of neurological diseases, treatment would be very easy with the cheap cost of treatment. Therefore, we should have a plan for screening for AC at an appropriate age of patients. However, there may be some objections that, given the low prevalence of the disease, screening tests are not appropriate. Nevertheless, if we look closely, we will find that screening for AC is very simple and cheap if not counting the endoscopic examination, which is the method used in this present research. Another interesting method is to test vitamin B12 levels, which is easy, inexpensive and patients do not need an endoscopy. Considering this study’s data which found that this disease is found only in patients aged 45 years and over, we may therefore have future studies to study whether it is worthwhile or not that we will only screen for AC in patients aged 50 years and over by using a cheap and easy way to do it in general such as checking vitamin B12 levels, but at the same time, if the patient is required to undergo a gastroscopy, we may consider using Congo red test used in this current study. Nevertheless, the data presented in this current study, in fact, do not support that Congo red screening is appropriate as the very low detection rate suggests that it is not worthwhile. It seems to be more reasonable for us to suggest that vitamin B12 screening may be an appropriate routine test in those with risk factors with age more than 50 years.
This present study showed the use of the Congo red method during OGD, which is a very convenient way of diagnosing AC from gastric mucosa. The process can be carried out with ease and safety, taking only an additional few minutes during an OGD. The results are also immediately produced and reportable. Using Congo red is a safe method because it causes no adverse event. In terms of the efficacy of AC detection, a prospective study by Tóth et al assessed the efficacy of the Congo red technique in 106 patients with the maximal acid output of less than 6.9 mmol/hour in men and 5.0 mmol/hour in women. The accuracy of the Congo red method was as high as 0.98 (95% CI 0.93 to 0.99).6 Moreover, using endoscopic findings from OGD alone is not sensitive enough to detect early stages of gastritis that have AC conditions such as early staged autoimmune gastritis. The use of Congo red in combination with OGD can help endoscopists better diagnose AC and be more sensitive.7 8
Other methods that can be used to diagnose AC were reported as follows. Measuring vitamin B12 level is another method which can detect patients with vitamin B12 deficiency. It is not the most efficient way because the threshold for vitamin B12 deficiency is a value of less than 100 pg/mL, while simply being below average is less than 200 pg/mL.9 10 Examination of parietal cell antibodies and intrinsic factor antibodies is also useful in detecting patients with AC and PA, with intrinsic factor antibodies being more specific but less sensitive than anti-parietal cell antibodies. The sensitivity and specificity of anti-parietal cell antibodies were found to be at 81% and 90%, respectively, while sensitivity and specificity of anti-intrinsic factor antibodies were 27% and 100%, respectively.11
In conclusion, results from this study which used the Congo red technique to detect AC during gastroscopy indicated that such a method could be easily used to diagnose AC. Nevertheless, given that the prevalence of AC in this current study was low, using vitamin B12 level in the high-risk group as a screening test seems to be more reasonable than the Congo red test. While the prevalence of AC in this current study was much less than that of AC reported in other studies, the characteristics of the population were different both in terms of ethnicity and types of population that were examined. The methods of testing were also different. Future prospective studies should be conducted to explore the benefits of using simple methods such as vitamin B12 level to detect AC in the population over 50 years old.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors KP: guarantor, data curation, formal analysis, writing—original draft, writing—review and editing. YS: data curation, writing—review and editing. CL: writing—review and editing. NN: data curation, writing—review and editing. YV: writing—review and editing. PK: data curation, formal analysis, writing—original draft, writing—review and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.