Article Text

Abstract
Objective Although clinical guidelines exist, the diagnostic work-up for diagnosing inflammatory bowel disease (IBD) is complex and varies in clinical practice. This study used real-life data to characterise the current diagnostic procedures used to establish IBD diagnoses in a Danish nationwide setting.
Design Person-level data on patients diagnosed with IBD between 1 January 2014 and 30 June 2018 were linked between Danish health registers. Information on age, sex, registration of other gastrointestinal diseases, and diagnostic procedures (endoscopies, biopsies, and imaging) performed in relation to the first IBD hospital admission was analysed for the total study population and was stratified by IBD type, sex, and age.
Results The majority of the 12 871 patients with IBD included underwent endoscopy (84%), had a biopsy taken (84%), and/or underwent imaging procedures (44%). In total, 7.5% of the population (6% for Crohn’s disease and 8% for ulcerative colitis) were diagnosed with IBD despite not undergoing any of these diagnostic procedures. Patients with Crohn’s disease underwent more procedures than patients with ulcerative colitis (94% vs 92%, p<0.001). Children underwent slightly fewer diagnostic procedures than adults (92% vs 93%, p=0.004). Slightly more men underwent at least one procedure than women (92% vs 94%, p<0.001).
Conclusion For 7.5% of patients with IBD, this study did not detect any registrations of the recommended diagnostic procedures for establishing an IBD diagnosis. Further research is needed to examine whether these findings are mainly explained by limitations of the register data or also indicate shortcomings of the general approach to IBD.
- INFLAMMATORY BOWEL DISEASE
- CROHN'S DISEASE
- ULCERATIVE COLITIS
- ENDOSCOPY
- IMAGING
Data availability statement
No additional data are available. The data underlying this article were provided by the Danish Health Data Authority (Sundhedsdatastyrelsen) and Statistics Denmark (Danmarks Statistik) by permission. Data will be shared on request to the corresponding author with permission of Statistics Denmark.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Diagnosing inflammatory bowel disease (IBD) is complex, and a commonly accepted ‘gold standard’ for the diagnosis is unavailable.
WHAT THIS STUDY ADDS
Although clinical practice for diagnosing IBD largely follows international guidelines, this study could not detect any registration of recommended diagnostic procedures for 7.5% of patients.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The study provides clinicians with nationwide data on the clinical procedures used to establish a diagnosis of IBD at Danish hospitals. The study raises clinically relevant research questions that need to be addressed to validate the quality of care and the use of Danish nationwide register data to evaluate clinical practice within IBD.
Introduction
Inflammatory bowel diseases (IBDs), with the two main subtypes, Crohn’s disease (CD) and ulcerative colitis (UC), are characterised by chronic gastrointestinal inflammation.1 2 Even though the IBDs differ in clinical profile, it is impossible to differentiate between CD and UC at the time of diagnosis for 5%–15% of the patients, and patients may then be classified as having IBD unclassified.3 4 Other gastrointestinal diseases, such as irritable bowel syndrome and infectious diarrhoea, can have presentations similar to IBDs and symptoms might be unspecific. Consequently, it could take weeks or months to establish the correct diagnosis and appropriate treatment choice. Meanwhile, the disease may progress and lead to irreversible organ damage, risk of misclassification, and ineffective therapy.1 2 5–7
According to international guidelines,4–13 recommended diagnostic tools for IBD include a clinical evaluation of the patient’s medical history and a combination of endoscopic, radiological, histological and/or biochemical investigations. The diagnostic work-up is complex without a commonly accepted ‘gold standard’ and may vary in clinical practice. Only a few studies have investigated procedures involved in establishing an IBD diagnosis,14–19 which, however, is important to identify shortcomings and areas for potential improvement. The Danish nationwide health registers provide a unique opportunity for such a study.
This study aimed to use nationwide real-life data between 2014 and 2018 to describe how current diagnostic procedures are used in men and women of different ages to establish the diagnoses of CD and UC, respectively.
Materials and methods
Study population
The study population comprised all Danish citizens (children and adults) with an incident IBD diagnosis between 1 January 2014 to 30 June 2018, according to the nationwide Danish National Patient Register (DNPR). The DNPR was established in 1977, containing all information about inpatient and outpatient contacts (since 1995) with Danish hospitals.20 The DNPR is considered to have high completeness and validity of the diagnoses of CD and UC (positive predictive values=91% and 85%, respectively, for having one IBD diagnosis code).21 22 Patients were included if they had no previous diagnosis of IBD registered during the ‘washout’ period from 1977 to 1 January 2014 to ensure the ascertainment of actual incident cases.
IBD was defined according to the 10th revision of the International Classification of Diseases diagnostic codes K50 (including all subcodes) for CD and K51 (including all subcodes) for UC. As IBD cases, we included those who had at least two IBD diagnoses (with the initial diagnosis registered in the period of 1 January 2014–30 June 2018) or one IBD diagnosis with an IBD-related hospital admission lasting at least 7 days. Primary as well as secondary discharge diagnoses were accepted as also used in other Danish cohort studies.23 24
The date of IBD diagnosis was defined as the date of the first hospital admission with IBD as the primary or a secondary discharge diagnosis. This date will be referred to as the ‘date of first IBD hospital admission’. Patients diagnosed with both CD and UC on the same date (n=143) were classified as patients with CD.
Linkage between the Danish health registers
The Danish Civil Registration System (DCRS) is a mandatory nationwide register established in 1968 containing all civil data for Danish citizens, including birth, death and migration dates. A unique 10-digit identification number (CPR) is assigned to all Danish citizens at birth or immigration and provides opportunities for linkage at the person level between Danish health registers.25 26
Patient characteristics related to hospital admissions
Information about patient characteristics related to the first IBD hospital admission included age, sex, and history of other gastrointestinal-related hospital admissions (online supplemental table S1) within 365 days before the first IBD hospital admission (online supplemental figure S1). Demographic data were retrieved from the DCRS. Patients were excluded if they had immigrated to Denmark less than 180 days prior to the date of first IBD and/or had no Danish address within the date of first IBD hospital admission±180 days (figure 1).
Supplemental material
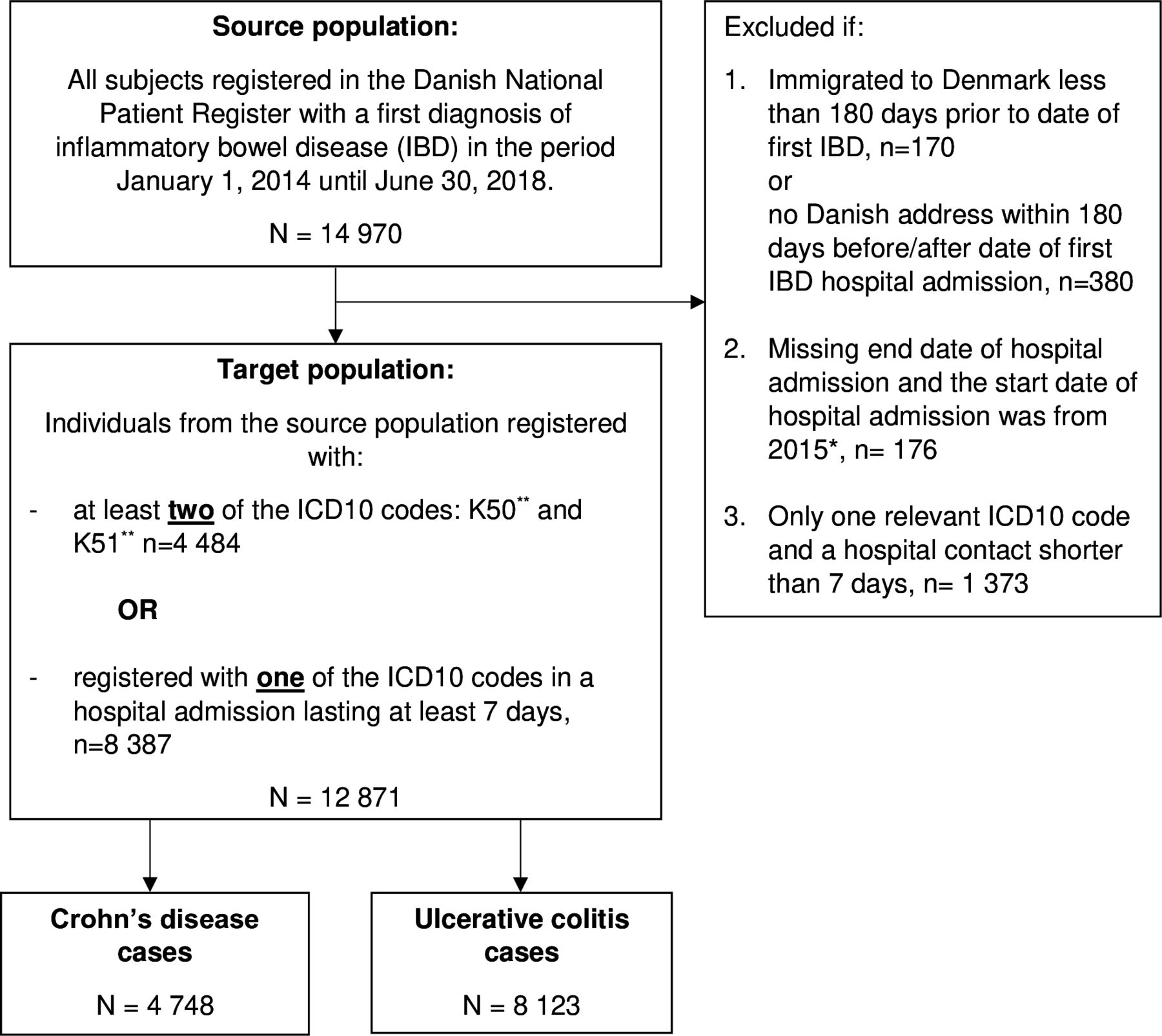
Flowchart. Patients diagnosed with both CD and ulcerative colitis at the same date (N=143) were classified as patients with CD. *From 2015, in the Danish hospital registration system, it was not mandatory to report the end date of a planned hospital admission. Therefore, we do not know whether missing end dates for planned patients with an index date after 2014 were due to an unfinished hospital admission or because the end date was not reported. **Inclusive of all subcodes. CD, Crohn’s disease; IBD, inflammatory bowel disease; ICD-10, 10th Revision of the International Classification of Diseases.
Diagnostic procedures
During 2014–2018, international guidelines4–6 8 9 27 recommended that diagnosis of IBD should, at a minimum, be based on the results of clinical procedures, including biological samples, endoscopies with biopsies and imaging, and medical history (see online supplemental table S2 for details).
Accordingly, we defined the diagnostic procedures for IBD as imaging, endoscopy, and gastrointestinal biopsy, with further subgrouping of endoscopy and imaging. A dichotomous variable was coded ‘1’ for each diagnostic procedure category (‘endoscopy’, ‘biopsy’, and ‘imaging’) and subgroups if a relevant procedure was registered at least once or otherwise coded ‘0’ (see online supplemental table S3) for the Nordic Medico-Statistical Committee (NOMESCO) codes28 used in the study.
Procedure codes for endoscopy and imaging were extracted from the DNPR. In addition, information on gastrointestinal biopsies was retrieved from the Danish Pathology Register (DPR).29 30 A gastrointestinal biopsy needed to include at least one of the following: a gastrointestinal topography code (T code), a gastrointestinal morphology code (M code), and a procedure code (P code) indicating ‘endoscopic biopsy’ (online supplemental table S4). The date registered in the DPR represents the date the pathology department receives the material, which may differ by several days from the actual procedure date.29 30 In addition to biopsies registered in the DPR, NOMESCO codes for endoscopic examinations with biopsies were also included (online supplemental table S3).
DNPR contains the registration of the primary diagnosis and any secondary diagnoses assigned to every hospital encounter, for which all medical procedures are also registered with a date.20 We chose the admission date of the IBD hospital admission as the reference date and defined a registration period of 180 days before and after this date (online supplemental figure S1) to optimise the capture of relevant diagnostic procedures. In addition, a registration period after the reference date was included to capture confirmatory diagnostic procedures used after the diagnosis.
We calculated the difference in days from the patients’ first experienced IBD relevant procedure and the reference date within the registration period of ±180 days for each procedure category and all procedures together.
Additional sensitivity analyses were conducted for 365 days as the length of the registration period. Moreover, a supplemental analysis investigated the clinical characteristics of patients with no diagnostic procedures compared with patients with at least one diagnostic procedure.
Statistical methods
All categorical variables were coded as dichotomous (yes/no) outcomes (except for age groups) and were presented as frequencies. Median age was reported with interquartile ranges (IQRs). In addition, results were presented for the total IBD study population and stratified by IBD type (CD and UC), sex and the age groups ‘children’ (<17 years) and ‘adults’, including elderly (≥17 years).31 32 The likelihood-ratio test evaluated differences in categorical variables between strata. P values below 0.05 were considered statistically significant. All analyses were conducted using Stata V.17.33
Results
There were 14 970 individuals having CD or UC registered for the first time as the primary or a secondary diagnosis between 1 January 2014 and 30 June 2018. Of these, 12 871 individuals fulfilled the inclusion criteria of having at least two IBD diagnoses (primary or secondary) or one IBD diagnosis (primary or secondary) with an IBD-related hospital admission lasting at least 7 days (figure 1). There were 4748 (36.9%) CD cases and 8123 (63.1%) UC cases.
Patient characteristics related to first IBD hospital admission
Table 1 presents the characteristics of the 12 871 patients included. There was similar distribution between sexes (52.0% females), and the median age at first IBD hospital admission (with IQR) was 40 (IQR 25–27) years. Children (<17 years old) and the elderly (>60 years old) represented 6.5% and 21.2% of the patients, respectively. Children represented 9.5% and 4.7% among patients with CD and UC, respectively. In the IBD population, 35.7% (44.0% among CD and 30.9% among patients with UC) had a history of other gastrointestinal-related hospital admissions within the year prior to diagnosis.
Patient characteristics and diagnostic procedures within a nationwide cohort of patients diagnosed with IBD within the period of 2014–2018
Diagnostic procedures
Total IBD population
In total, 92.5% of the patients with IBD underwent at least one diagnostic procedure. Endoscopy and biopsy were the most frequent diagnostic procedures (84.0% and 84.3%, respectively), with enteroscopy and colonoscopy being the primary endoscopy modality (81.9% of total patients). Imaging was least used (43.9%), with MR scans and CT scans the most frequently applied modalities (21.9% and 23.2% of patients, respectively). Among the total IBD population, 70.3% had at least one registration of an endoscopic examination with biopsy in the DNPR, and 75.7% had at least one gastrointestinal biopsy registration in the DPR (table 1).
Concerning the combination of procedures (endoscopy, biopsy, and imaging) undergone by each patient during the registration period, endoscopy and biopsy formed the most frequent combination (41.9%), followed by all three procedures (36.9%) (figure 2).

Frequencies and combinations of diagnostic procedures (endoscopy, biopsy, and imaging) within the total population. The distribution of frequencies of diagnostic procedures (endoscopy, biopsy, and imaging) is presented with percentages of the total population (N=12 871) (left). The distribution of the 46% (n=5914) of the total population who underwent two procedures was as follows, according to combinations of procedure types: 41.9% endoscopy and biopsy, 2.6% biopsy and imaging, and 1.5% endoscopy and imaging (right).
CD and UC
Slightly more patients with CD underwent at least one diagnostic procedure compared with patients with UC (93.7% vs. 91.7%). Endoscopy was more frequent in patients with CD compared with patients with UC (85.5% vs 83.2%), and for imaging, the difference was also more pronounced (69.3% vs 29.0%, respectively). In contrast, biopsy was slightly more common for UC patients than patients with CD (86.1% vs 81.4%, respectively). Among endoscopy modalities, enteroscopy and colonoscopy were used most frequently for patients with CD (81.9%) and patients with UC (82.1%), followed by gastroscopy, which was used significantly more in patients with CD than in patients with UC (25.9% vs. 9.6%, respectively). The most frequently used imaging modalities were MR scan for patients with CD (43.6%) and CT scans for patients with UC (16.7%) (table 1). These differences were statistically significant when stratified according to age and sex (table 2).
Distributions of diagnostic procedures within the study population stratified on IBD type, sex and age groups
Women and men
More men had at least one diagnostic procedure compared with women (93.6% vs 91.5%, respectively). Endoscopy was slightly more frequent in men than in women (85.1% vs 83.0%, respectively), and for imaging, no significant difference was found (43.3% males and 44.4% females). However, biopsies were more frequent in men compared with women (86.2% vs 82.6%, respectively) (table 1). When stratified on IBD type and age groups, differences were statistically significant. However, no significant differences were found for overall imaging, MR scans, and capsule endoscopy (table 2).
Children and adults
The proportion of the population with at least one procedure was slightly, but statistically significantly, lower in children compared with adults (91.6% vs 92.5%, respectively). Overall, endoscopy was equally distributed between children and adults (84.6% vs 84.0%, respectively). Imaging was more frequent in children than in adults (63.5% vs 42.5%, respectively), whereas the proportion undergoing a biopsy was lower in children (83.1% vs 84.4%, respectively). Enteroscopy and colonoscopy were the most frequently used endoscopy modalities in children and adults (81.0% and 81.9%, respectively), followed by gastroscopy. However, a gastroscopy was used significantly more frequently in children (62.0%) compared with adults (12.4%). The most used imaging mortalities were MR scans in children (48.6%), and CT scans in adults (24.3%). However, only 7.1% of children had a CT scan (table 1). Differences between children and adults according to all procedure types except capsule endoscopy were statistically significant when stratified on IBD type and sex. In addition, more female children than female adults had an endoscopy, whereas the reverse was the case for male children and adults (table 2).
Timing of first diagnostic procedures relative to the date of the first IBD hospital admission
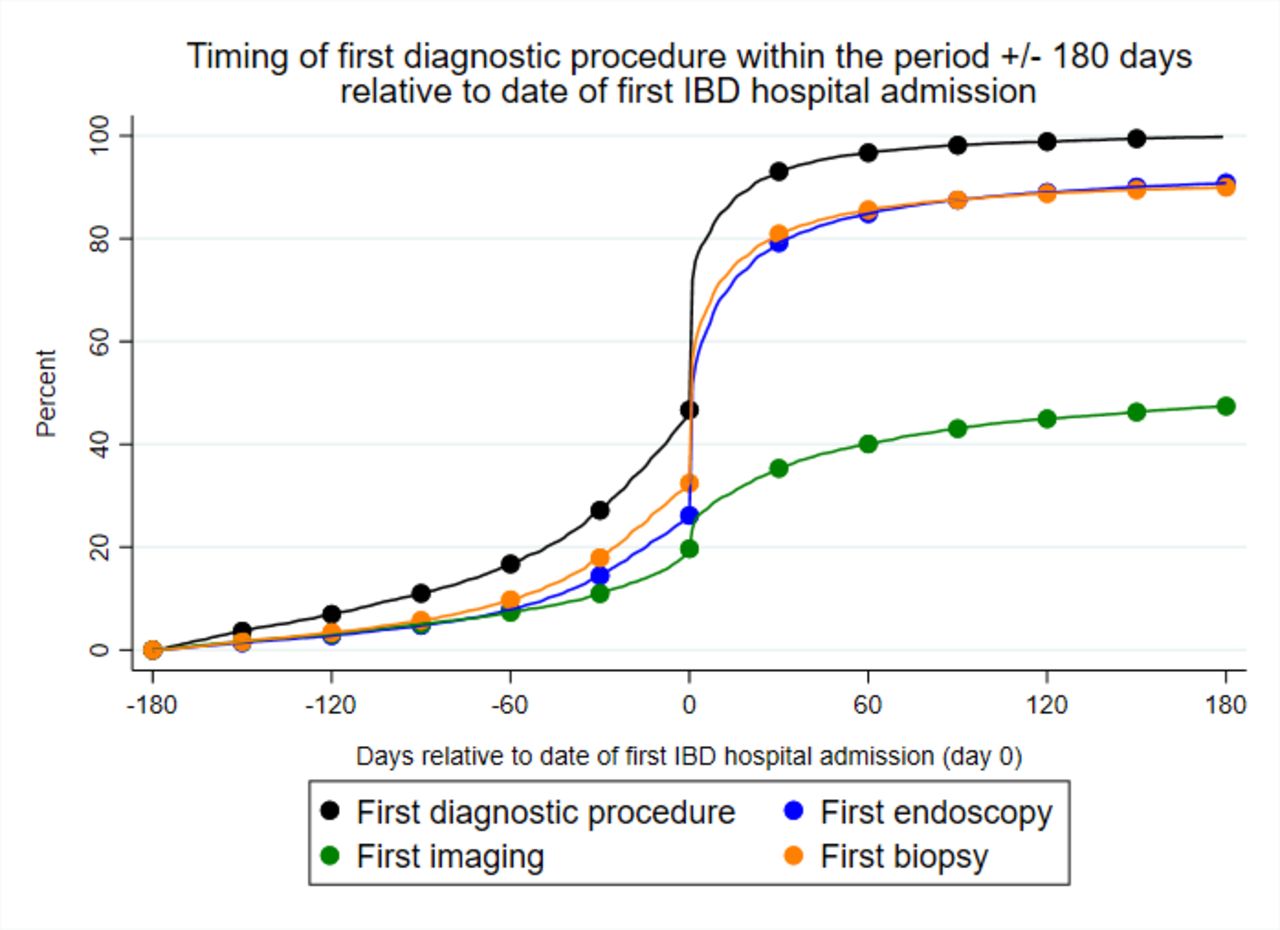
We investigated the timing of the patients’ first IBD-relevant procedure (n=11 903, 100%) within the defined registration period of ±180 days relative to the reference date. Of these, 46.9% had their first procedure before the date of first IBD hospital admission. For 25.0% of patients, the first diagnostic procedure coincided with the date of IBD hospital admission, and the remaining 28.1% underwent their first diagnostic procedure after the date of their first IBD hospital admission. Among those who underwent at least one procedure, nearly all patients (93.4%) had been examined with a procedure 30 days after the date of the first IBD hospital admission (figure 3).

{kind=link}
{kind=link}
{kind=link}
Timing of first diagnostic procedures relative to the date of the first IBD hospital admission (accumulated percentages). The date of the first IBD hospital admission is represented by “0” on the horizontal axis. The registration period is defined as the period±80 days from the date of the first IBD hospital admission. The accumulated percentages of the patients who have undergone the respective diagnostic procedures are presented on the vertical axis. The black line represents the first diagnostic procedure performed (any of the procedures) within the defined registration period. The blue line represents the first endoscopy; the orange line represents first gastrointestinal biopsy; the green line represents the first imaging. Dots represent the percentages for each 30 days within the period. Within each of the procedure types, we see that the curve begins to stagnate after 30 days from the date of the first hospital admission, indicating that nearly all patients (who had underwent that procedure at least once) had had their first examination at that time point. IBD, inflammatory bowel disease.
Discussion
In this nationwide population-based cohort study of 12 871 patients with initial IBD diagnosis between 2014 and 2018, 92.5% of the patients underwent at least one of the recommended procedures (endoscopy, biopsy, or imaging) in the interval ±180 days before and after the date of first IBD hospital admission. Endoscopy (84.0%) and biopsy (84.3%) were the most frequent diagnostic procedures. Patients with CD underwent more diagnostic procedures than patients with UC. Children underwent slightly fewer diagnostic procedures than adults, with further differences within specific procedure types. Overall, more men underwent at least one procedure compared with women.
The major strength of this study was the use of pre-existing person-level data with a linkage between several health registers in a large nationwide population-based cohort. This strength reduces the risk of selection bias and provides wide-ranging information to describe the diagnostic procedures used for IBD. As another strength, we ensured a high positive predictive value of IBD diagnoses by requiring that cases fulfilled diagnostic criteria according to both type of diagnosis code (primary and secondary), number of diagnoses, and length of hospital course. It is a potential limitation that, unless the initial hospital admission had a long duration, the inclusion criteria of having at least two diagnoses registered at independent events made ascertainment depended on future events. This has a minor impact only, since 84% of the patients were ascertained by at least two diagnoses with a year or less between the first and the second diagnoses, and the maximum of years between first and second diagnoses was 5 years. Recent studies have used different diagnostic criteria, and no single ‘gold standard’ exists.22 23 34–36 The length of the hospital admission was used to decrease the risk of misclassification (false positives) of patients with only one diagnosis. Among those patients with only one diagnosis registered but with a hospital admission lasting at least 7 days, 618 (13.8%) were diagnosed in the last year of the inclusion period (2018). Thus, a second qualifying diagnosis may have been registered after the end of follow-up. However, the percentage of patients with only one IBD diagnosis registered was higher among patients with no diagnostic procedures compared with those having at least one procedure (62.6% vs 32.6%). This observation may indicate that the lack of procedures, to some extent, could be explained by misclassification of the IBD diagnosis.
There are further limitations to this study. First, the registration period used to capture diagnostic procedures is arbitrary and may not truly reflect the real period used for establishing the diagnosis of IBD in the individual patient. Second, the register data do not permit to establish the exact date of diagnosis. We have used the first date of admission to hospital with IBD as date of diagnosis, but this diagnosis is assigned at discharge from the hospital, which can be several days or weeks after the date of admission. Third, other relevant diagnostic information was unavailable, including detailed description of pathology of biopsies and information on the extent of disease. According to the guidelines, extent of disease could influence the diagnostic protocol.4–9 27 Moreover, the date of a biopsy requisition may differ by several days from the actual surgical procedure date. Furthermore, for this study, results from blood sample examinations were unavailable due to incomplete reporting to the Danish Laboratory Database.37 Blood sample investigations and stool tests are essential in diagnosing IBD, and future studies should include this information when investigating the complete diagnostic work-up. In addition, this study did not include data from practising specialists in gastroenterology outside the hospital system. Commonly, patients diagnosed outside the hospital system are later referred to hospitals for future control and treatment but not necessarily further clinical examinations such as endoscopy or imaging. This may offer an explanation of missing procedures. Finally, the potential for evaluating clinical practice in relation to diagnostic guidelines is challenging using register data with no information on patient symptoms’ debut and why certain diagnostic strategies were chosen.
The study has several clinically relevant messages. Overall, the current diagnostic practice investigated in this study followed the diagnostic guidelines for IBD, as most patients underwent an endoscopy and had a biopsy taken. Furthermore, the most frequently used endoscopy type was an enteroscopy or colonoscopy. A gastroscopy is only recommended in cases with upper gastrointestinal symptoms.4–6 8 9 27 Worldwide, upper gastrointestinal tract involvement in adult patients with CD is less than 5%–8% of patients,1 17 which may explain why less than 20% underwent a gastroscopy. However, a gastroscopy was more frequently used in children than in adults, according with more CD cases among children and the recommendation of upper gastrointestinal endoscopy as routine in children.38 Imaging (CT scan, MR scan, and small bowel ultrasound) is recommended in CD and should be routine for children6 8 38 (online supplemental table S2). The results probably reflect the number of patients suspected of CD as the imaging procedures were used around double as frequently in patients diagnosed with CD compared with UC. Still, 29% of UC cases had imaging, which could be due to the uncertainty of the diagnosis. According to guidelines, MR and ultrasound are also preferred to CT scans4–6 8 9 27 to minimise radiation exposure despite the higher costs and requirements for experienced staff.
Even though the recommendations for IBD diagnostic procedures do not include gender disparities, we found significant differences in the frequencies of endoscopic procedures and biopsy, dependent on IBD type and age.
To our knowledge, this is the first nationwide, register-based cohort study examining the procedures that patients with IBD undergo during the diagnostic work-up. Only a few other smaller cohort studies have investigated clinical procedures used in relation to IBD diagnosis or subsequent follow-up.17–19 For example, another Danish population-based cohort study of 513 patients diagnosed in 2003–2004 reported that 100% of patients with CD and 97% of patients with UC underwent at least one clinical procedure (endoscopy, CT scan, MR scan, ultrasound, or X-ray) during a 10-year follow-up period after diagnosis.19 A European (Western countries, including Denmark) population-based cohort study of 711 patients with IBD diagnosed in 2011 reported colonoscopy in 90% of CD cases and 82% of UC cases, and CT and MR scans in 38% and 19% of CD cases, respectively, and only 5% and 2% of UC cases.18 These studies also found that most patients underwent endoscopy; patients with CD underwent more endoscopic procedures compared with patients with UC; and imaging was used more than twice as frequently in patients with CD compared with patients with UC. Neither of these studies stratified the results according to age or sex.
Importantly, we could not detect any registrations of the recommended diagnostic procedures for a substantial number of the patients. Thus, more than one-third of children had not undergone imaging, although this is recommended as routine practice, and 16% of the total patients with IBD had not undergone an endoscopy. Furthermore, gastroscopies were significantly more frequently used in children with CD than adults with CD. Most of these conundrums may be explained by the methodological limitations in this study, that is, incomplete register information and registration failures. Other explanatory reasons may be related to the patient’s hospital admission and disease trajectory. A supplementary analysis investigated further the 968 (7.5%) patients (online supplemental table S6) for potential misclassification of IBD. Such patients might initially be referred to hospital with a diagnosis of IBD, but subsequently considered to have other diagnoses (including irritable bowel syndrome (IBS) or infectious enteritis) due to subsequent finding of normal calprotectin levels or stool positive for microbes, but without deleting the IBD diagnosis. We found that 23 (only 2.4%) of patients with no diagnostic procedures had a diagnosis of IBS or infectious enteritis within 180 days after the first IBD diagnosis. Alternatively, the diagnosis of CD may have been established exclusively because of acute bowel surgery for suspected appendicitis before or at the date of diagnosis. Since 22 (only 2.3%) of patients with no diagnostic procedures had bowel surgery before or at the date of first IBD diagnosis this is an unlikely explanation for the lack of registered diagnostic procedures. A total of 606 (62.6%) patients with no diagnostic procedures had been registered with only one IBD diagnosis but a long hospital admission, compared with 32.6% among those having at least one procedure. Of those 606 patients, 83.2% were diagnosed at an IBD-relevant hospital department (including medical gastroenterology, internal medicine, surgical gastroenterology, surgery, and paediatrics) (results not shown). In these patients, a wait-and-see approach might have been chosen and disease progression or the need for further examinations may never have occurred, at least not within our defined registration period. Among patients with at least two IBD diagnoses, the median days between first and second diagnoses in patients with no diagnostic procedures was 273.5 days (IQR 70–558) and much longer compared with patients with at least one diagnostic procedure (median 41, IQR 11–183). This finding is compatible with a wait-and-see approach at the first IBD hospital admission without initial diagnostic procedures in patients with mild IBD symptoms. On the other hand, we found in an additional analysis that 414 (42.8%) of the patients with no diagnostic procedures had received IBD-related medical treatment within 180 days after their first IBD diagnosis (online supplemental table S5 and online supplemental table S6), which could indicate a certain degree of severity of the disease. Since it is generally expected that medical treatment in IBD would not be initiated without proper diagnostic evaluation, it is unlikely the mild symptoms and a wait-and-see approach could explain most of cases with missing procedures. Other possible explanations for missing procedures include that endoscopy is not recommended in patients with severe, active disease due to the risk of bowel perforation.5 6 8 9 27 38 That, in Europe, may comprise up to one-third of patients at diagnosis.39 In this study, though, data were lacking on the extent and severity of disease. Also, diagnostic endoscopy may not have been performed due to patient preference. The absence of imaging may potentially be explained by logistic challenges and a lack of experienced staff. Further studies are warranted to explain the reasons and clinical implications of the deviations found in our study from the international recommended guidelines.
Among patients who underwent at least one procedure, 53% did not undergo diagnostic procedures during the period before their first IBD hospital admission (figure 3). This is compatible with the finding that 37% of patients with IBD had no diagnostic procedures in the year before hospitalisation.14 Some patients might have been asymptomatic until the IBD diagnosis was given at a hospitalisation with acute symptoms. Other cases may be explained by mild symptoms and a wait-and-see approach as described previously. Moreover, if a patient, in the period after initial diagnosis, responded very well to medical treatment, there may have been no need for further examinations. When expanding the registration period from ±180 days to 365 days before and after the first IBD diagnosis, more patients had undergone at least one diagnostic procedure (n=12 183 (94.7%)) (online supplemental table S7). This indicates that the diagnostic period, for some patients, exceeds 180 days before and after the first IBD hospital admission. There is a need for further research to investigate whether the omission of performing diagnostic procedures relates to shortcomings in the general clinical approach to IBD or may be explained by unique patient characteristics.
Conclusion
In conclusion, this nationwide study using real-world data to describe current IBD diagnostic practices in Denmark shows that clinical practice for diagnosing IBD largely follows international guidelines as most patients undergo endoscopy with or without biopsy. However, for 7.5% of patients, no registrations of the recommended diagnostic procedures were detected. While some of these patients may have well-founded IBD, the main part may be false-positive due to misclassification or to shortcomings of register data. This study cannot exclude that the missing procedures were performed in private practice. Therefore, further research is needed to investigate the explanations and the clinical implications underlying the lack of diagnostic procedures and to examine the extent to which this is due to shortcomings in the general approach to IBD or unique patient characteristics.
Data availability statement
No additional data are available. The data underlying this article were provided by the Danish Health Data Authority (Sundhedsdatastyrelsen) and Statistics Denmark (Danmarks Statistik) by permission. Data will be shared on request to the corresponding author with permission of Statistics Denmark.
Ethics statements
Patient consent for publication
Ethics approval
The study was register-based and approved by the Danish Data Protection Agency (19/46593) and the Danish Patient Safety Authority.
Acknowledgments
We thank Caroline Moos for language editing services.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
TJ and VA contributed equally.
Contributors NFR: design of the study, acquisition, preparation, analysis and interpretation of data, and drafting the manuscript. AG: design of the study, preparation, analysis and interpretation of data. AKP and DLW: data management support and figure generation. ATI: data management, preparation, analysis and interpretation of data. GIM and TJ: design of the study. KHA: design of the study and interpretation of data. VA: conception, design of the study and interpretation of data. All authors provided substantial contribution in revising the manuscript critically for important intellectual content and approved the final version to be published. TJ and VA contributed equally as last authors. VA is responsible for the overall content as the guarantor.
Funding This work was supported by the Hospital of Southern Jutland (grant number not applicable), the Research Unit of Molecular Diagnostic and Clinical Research (grant number not applicable), the University of Southern Denmark, the Danish Beckett-Fonden [grant number 20-2-6128] and the Danish Knud and Edith Eriksens Mindefond to NFR (grant number not applicable).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.