Article Text

Abstract
Objective Management of erosive oesophagitis (EE) remains suboptimal, with many patients experiencing incomplete healing, ongoing symptoms, and relapse despite proton pump inhibitor (PPI) treatment. The Study of Acid-Related Disorders investigated patient burden of individuals with EE in a real-world setting.
Design US gastroenterologists (GIs) or family physicians (FPs)/general practitioners (GPs) treating patients with EE completed a physician survey and enrolled up to four patients with EE for a patient survey, with prespecified data extracted from medical records.
Results 102 GIs and 149 FPs/GPs completed the survey; data were available for 73 patients (mean age at diagnosis, 45.4 years). Omeprazole was healthcare professional (HCP)-preferred first-line treatment (60.8% GIs; 56.4% FPs/GPs), and pantoprazole preferred second line (29.4% and 32.9%, respectively). Price and insurance coverage (both 55.5% HCPs) and familiarity (47.9%) key drivers for omeprazole; insurance coverage (52.0%), price (50.0%), familiarity (48.0%), initial symptom relief (46.0%), and safety (44.0%) key drivers for pantoprazole. Only 49.3% patients took medication as instructed all the time; 56.8% independently increased medication frequency some of the time. Despite treatment, 57.5% patients experienced heartburn and 30.1% regurgitation; heartburn was the most bothersome symptom. 58.9% patients believed that their symptoms could be better controlled; only 28.3% HCPs were very satisfied with current treatment options. 83.6% patients wanted long-lasting treatment options. Fast symptom relief for patients was a top priority for 66.1% HCPs, while 56.6% would welcome alternatives to PPIs.
Conclusion This real-world multicentre study highlights the need for new, rapidly acting treatments in EE that reduce symptom burden, offer durable healing and provide symptom control.
- EROSIVE OESOPHAGITIS
- GASTROESOPHAGEAL REFLUX DISEASE
- QUALITY OF LIFE
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Patients with erosive oesophagitis (EE) have a high symptom burden and an increased rate of lung diseases such as pulmonary fibrosis, bronchiectasis, and pneumonia, as well as Barrett’s oesophagus. Current treatment guidelines recommend proton pump inhibitors for the healing and symptom relief of EE.
WHAT THIS STUDY ADDS
Both patients and physicians are generally dissatisfied with current treatment options in EE, with most patients continuing to experience significant symptoms despite PPI treatment.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
There is a need for new treatments for EE that act rapidly to reduce symptoms and provide durable healing and symptom control.
Introduction
In the USA, approximately 20% of people experience symptoms of gastro-oesophageal reflux disease (GERD) at least once a week, with the most common symptoms being heartburn and regurgitation.1–3 GERD is classified into three different phenotypes—non-erosive reflux disease, erosive oesophagitis (EE), and Barrett’s oesophagus (BE)—on the basis of endoscopic and histopathologic appearance.4 Whether these phenotypes represent categorical or continuous subtypes is controversial.5 EE accounts for around 30% of patients with GERD,5 and is the most common endoscopic abnormality documented among patients undergoing endoscopy for the investigation of upper gastrointestinal symptoms with a pooled prevalence of 13.4% across studies.5 EE is linked to increased rates of lung diseases such as asthma, chronic obstructive pulmonary disease, pulmonary fibrosis, bronchiectasis, and pneumonia,6 and is also an important risk factor for the development of BE, a premalignant condition for oesophageal adenocarcinoma (EAC).7
Current treatment guidelines recommend proton pump inhibitors (PPIs) for the healing and symptom relief of EE.8 9 After initial healing of mucosal erosions and relief of symptoms, PPIs are recommended for long-term maintenance in EE and for indefinite treatment for those considered to have severe EE.6 9 In patients with the most severe disease (Los Angeles (LA) classification C or D), repeated oesophagogastroduodenoscopy is recommended after treatment to ensure healing, guide future treatment, and confirm an absence of BE.10
Despite the availability of different treatment options, substantial unmet needs remain in the management of EE. For example, up to 15% of patients with EE do not achieve complete mucosal healing after 8 weeks of standard PPI treatment. In addition, the symptomatic response rate for standard-dose PPI therapy in patients with EE is approximately 55%, while 20% of patients continue to experience heartburn while on standard PPI therapy.11 Relapse is typical in EE if PPI treatment is discontinued,6 and may also occur despite maintenance treatment with a PPI; one study reported relapse rates of between 10% and 41%, depending on severity/grade of oesophagitis at diagnosis.12 Even after initial healing of oesophageal erosions, symptomatic relapse occurs in over 80% of patients within 12 months of discontinuation of maintenance treatment,13 while endoscopic relapse of EE occurs in around 90% of patients regardless of initial grade of EE.14
Patients with GERD who have an incomplete response to PPI treatment report decreased quality of life.15 Among those with EE, physical health scores in one study were 8%–16% lower than those without EE,16 and 73% of patients experienced somatisation.17 There is also a high social cost of repeat medical visits throughout the course of the disease.15
Despite the abundance of reports suggesting that the management of EE remains suboptimal,5 and despite a lack of therapeutic innovation in this area for a considerable time,6 14 15 18 few studies have specifically reviewed current treatment gaps in a real-world US population from the perspectives of both patients and physicians. This study was designed to investigate the patient burden of individuals with EE through insights from patient and physician surveys, supplemented with data recorded on patients’ case report forms (CRF).
Methods
Study design
A geographically representative sample of gastroenterologists (GIs) and family physicians (FPs)/general practitioners (GPs) currently treating patients with EE were recruited from community practices throughout the USA using internet panels and targeted custom enrolment. Physician recruitment was closely monitored to ensure that a balanced sample of physicians was achieved.
Eligible physicians were asked to complete a survey relating to their own demographic characteristics and those of their consulting population, as well as prescribing habits, treatment satisfaction, and patient adherence. On completion of the survey, enrolled physicians invited between one and four of their patients with EE to complete a patient survey. Questions in the patient survey were related to demographics, treatment adherence, symptom burden, and treatment satisfaction.
Finally, prespecified medical information was extracted from the respective medical records of patients who completed the survey, including patient management and treatment patterns. Thus, patient survey and medical chart data were matched for all patients.
Study population
Qualified GIs or FPs/GPs with between 4 and 40 years of experience in clinical practice in the USA (excluding Maine or Vermont) were eligible if they were responsible for the treatment and management of at least 10 (GIs) or 5 (FPs/GPs) patients with EE per month, and had fewer than 40% of their patients participating in clinical trials.
Patients were eligible for inclusion if they were between 18 and 75 years of age at the time of enrolment, provided written consent to participate in the study, could read and understand English well enough to participate in the study, had a physician-confirmed diagnosis of EE (International Classification of Diseases 10 code of K21.0 GERD with oesophagitis), and were currently being treated with a PPI for EE. Patients diagnosed with an untreated psychiatric disorder or memory problems were excluded from the study. Physicians and patients were remunerated for their time in participating in the study.
Data collection
The data in this study were derived from three distinct components: the physician survey, the patient survey, and the prespecified extraction of medical chart data from CRFs. Physician and patient surveys were completed by respondents online, and each took approximately 30 min. Data capture from medical charts took around 15 min, and was carried out by participating physicians.
The physician survey covered the physician’s demographic characteristics, consulting population, prescribing habits, treatment satisfaction, and perception of patient adherence. Responses were rated on a scale from 1 (strongly disagree) to 7 (strongly agree); ‘agreement’ was indicated by scoring 6 or 7 on the 7-point scale. The patient survey covered demographics, treatment adherence, symptom burden, treatment patterns, and treatment satisfaction. Responses were rated on a scale from 1 (not at all) to 7 (extremely); ‘agreement’ was indicated by scoring 6 or 7 on the 7-point scale. The electronic case report form (eCRF) captured information relating to patient demographics, clinical characteristics, patient management, and any hospitalisations and procedures. The physician and patient surveys are included in online supplemental material 1 available with the online version of this article.
Supplemental material
A prespecified set of exacting quality control measures were followed at all stages throughout the data collection process to maximise data quality.
Statistical analysis
Data are presented using descriptive statistics. Specifically, categorical variables are presented as frequency and percentage distributions, and ordinal variables as frequencies and percentages as appropriate. Continuous variables (eg, age, time since diagnosis, and questions with Numerical Rating Scale responses) are presented as means/medians and SDs. CIs are included where appropriate.
There was no imputation of missing data, or aggregation across questions.
Results
Study population
The survey was completed by 102 GIs and 149 FPs/GPs. In addition, 19 GIs and 28 FPs/GPs completed a patient eCRF, providing CRF data from 73 patients.
GIs treated 24.6% of their patients in hospital and 73.4% in an office setting (2.0% other setting), compared with 6.3% and 91.7% (2.0% other setting), respectively, for FPs/GPs. GIs had evaluated a mean of 57.3 patients with EE in the preceding month, compared with 35.7 patients with EE for FPs/GPs. Thirty-six per cent and 32% of GIs and FPs/GPs were licenced to practice medicine in the Mid-West compared with 28% and 24% in the North East, 19% and 25% in the West, and 27% and 26% in the South of the country, respectively. Thirty-seven per cent of physicians overall qualified for their primary specialty between 2001 and 2010, 30% between 1991 and 2000, 22% between 2011 and 2016, and 11% of physicians qualified between 1980 and 1990.
Data from 73 patients were included in this survey, 31 of whom were patients of GIs, and 42 of FPs/GPs. The mean (SD) age of patients at enrolment was 48.2 (14.2) years, and the mean (SD) age at EE diagnosis was 45.4 (13.9) years. The mean (SD) body mass index was 27.0 (5.0), and 39% of GI patients and 45% of FP/GP patients were men. Seventy per cent of patients were white, 10% were Hispanic/Latino, 8% were black or African American, 5% were mixed race, and 4% were Asian. Thirty-seven per cent of patients overall had a bachelor’s degree, while the highest educational level reached by 21% of patients was a high school diploma and general educational diploma. Fifty-eight per cent of patients were working full time, and no patients were on long-term sick leave at the time of the survey.
At the time of the survey, 81% of patients were classified as LA Grade A, 14% as Grade B, 4% as Grade C and 1% as Grade D.
Treatment patterns
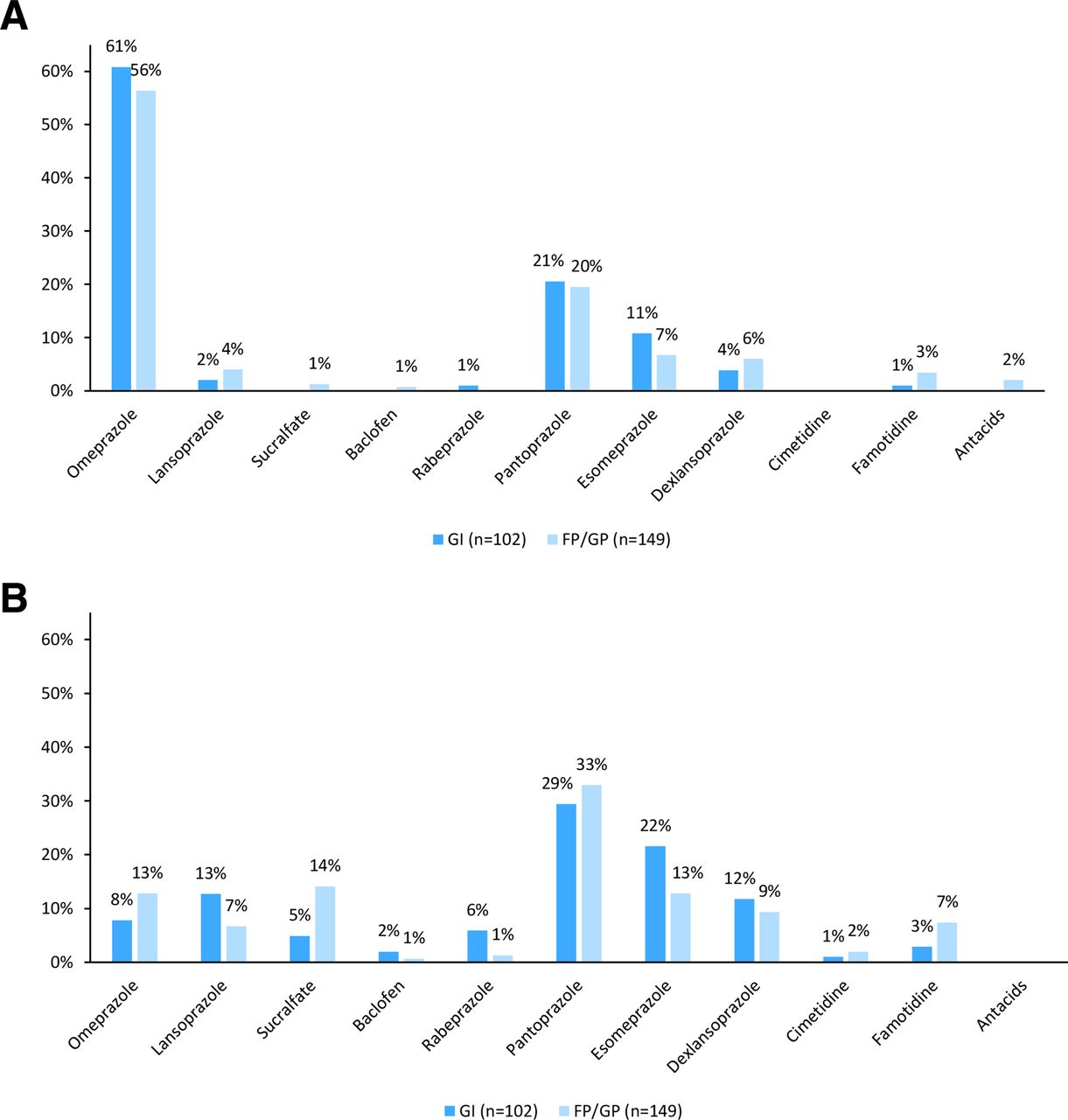
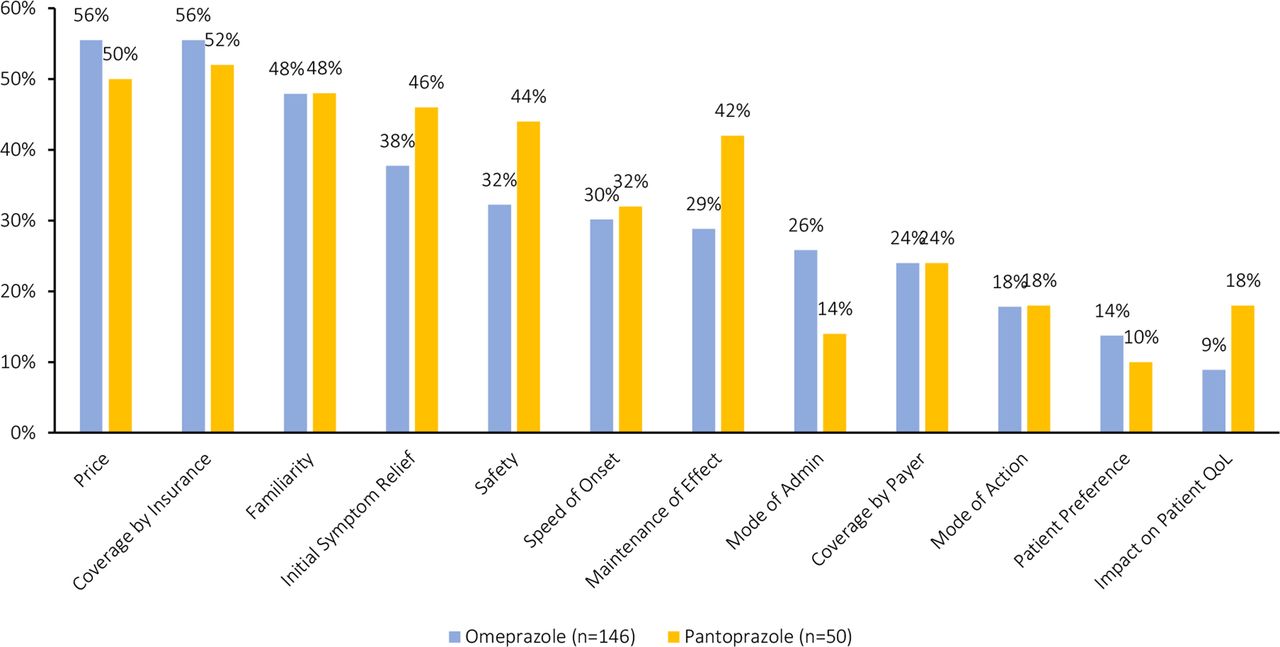
In the physician survey, omeprazole was the preferred first-line treatment option (60.8% of GIs and 56.4% of FPs/GPs), while pantoprazole was preferred as the second-line option (29.4% and 32.9%, respectively) (figure 1). In terms of first-line therapy, price (55.5%) and coverage by insurance (55.5%) were key drivers for choice of omeprazole, while coverage by insurance, price, and familiarity were key drivers for pantoprazole (52.0%, 50.0%, and 48.0%, respectively) (figure 2).
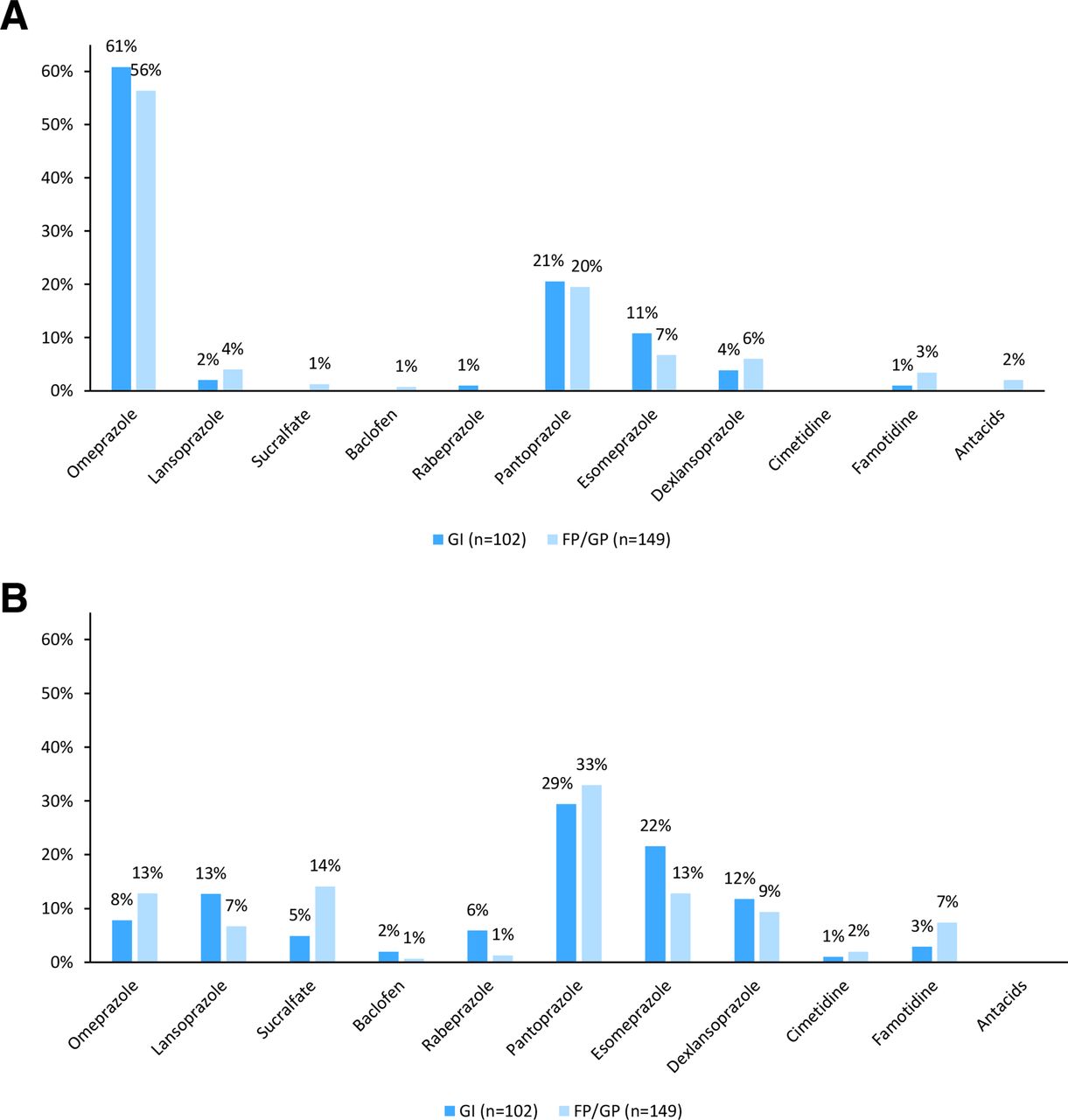
Therapy typically used (A) first and (B) second for newly diagnosed patients with EE (physician survey). Base: Physicians (251). Source: Physician survey: C1a. Which therapy would you typically use first and then second for newly diagnosed patients with erosive oesophagitis? EE, erosive oesophagitis; FP, family physicians; GIs, gastroenterologists; GP, general practitioner.

HCP reason for preferred first-line therapy. Base: Physicians preferring omeprazole (146) physicians preferring pantoprazole (50). Source: Physician survey: CQ2. Why is <show product selected as first choice in CQ1 >your preferred first-line choice for EE? EE, erosive oesophagitis; HCP, healthcare professional; QoL, quality of life.
Speed of onset was given as the reason for choosing omeprazole as first-line therapy by 32.3% of GIs and 28.6% of FPs/GPs, while 27.4% of GIs and 29.8% of FPs/GPs chose omeprazole because of its maintenance of effect.
According to eCRF data, 31.5% of patients received pantoprazole as their most recent line of therapy, while 24.7% received esomeprazole, 21.9% received omeprazole, and 15.1% received dexlansoprazole. In total, 15.1% of patients received an antacid as a component of their most recent line of therapy. According to the patient survey, 24.6% of patients took a PPI two times a day or more frequently.
In total, 72.5% of healthcare professionals (HCPs) recommended that patients add over-the-counter (OTC) therapy to their prescribed therapy. (No further details regarding the type of OTC therapy were captured.)
Adherence
Only 49.3% of patients reported taking their medication as instructed all of the time, and 67.1% of patients agreed that they would be more likely to take their treatment as advised if it worked more quickly.
Overall, 56.8% of patients reported that they independently decided to increase the frequency of their medication (type of medication not captured) at least some of the time. Reasons given by HCPs for patients’ changes to dosing frequency without their knowledge are given in figure 3. Sixty-one per cent of HCPs believed that the main reason for patients altering treatment frequency was because the treatment was not working adequately.
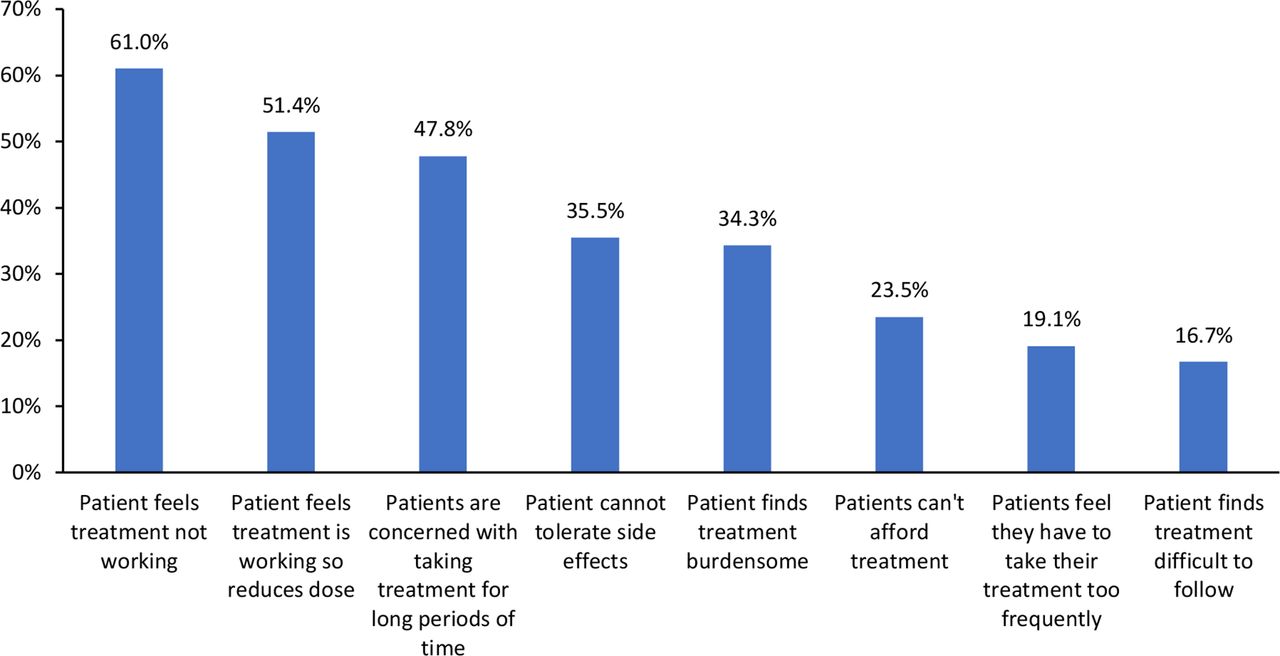
Reasons given by gastroenterologists and family physicians/general practitioners to explain why patients change dosing frequency without their knowledge. Base: 251. Source: Physician survey C4a. Reason for changing dosing frequency without your knowledge.
In total, 31.5% of patients agreed that they found food-related dosing to be burdensome, while 49.4% of HCPs would prefer a product that did not have a dosing requirement related to food intake.
Symptom burden
Although symptoms improved with treatment, many patients continued to experience a range of symptoms (figure 4A). For example, despite treatment, 57.5% continued to experience heartburn and 30.1% continued to experience regurgitation. Heartburn was the most bothersome symptom, as reported by both patients and physicians (figure 4B).

(A) Symptoms experienced as reported by patients; (B) Most bothersome symptoms as reported by physicians and patients (A) Base: All patients (73). Source: PSC_B_1a. Patients with EE. Symptoms experienced ever? PSC_B_1b. Patients with EE. Symptoms experienced in the past month? (B) Base: Patients indicating current symptoms in BQ1a (68). Source: Physicians—CRF B6 Which of these symptoms do you think are the most bothersome to your patient? Patient survey: B1c please rank these symptoms (symptoms indicated as bothersome in BQ1c) starting with the most bothersome, up to a top five. CRF, case report form; PSC, Patient self-complete.
Treatment satisfaction
In total, 58.9% of patients believed that their symptoms could be better controlled (58.0% of patients with LA Grades A/B and 75% of patients with LA Grades C/D). Physicians believed that better control could be achieved in 34.8% of their patients. In addition, 55.6% of patients overall (56.2% with LA Grades A/B and 50.0% with LA Grades C/D) considered that they would be very satisfied if they only had to take a PPI one time a day, while 47.9% of patients overall (44.9% with LA Grades A/B and 100.0% with LA Grades C/D) would feel more satisfied if they could reduce the need to supplement with an OTC therapy. Only 28.3% of HCPs agreed that they were satisfied with current treatment options.
Treatment goals
Patient attitudes to treatment are summarised in online supplemental table 1. Overall, 83.6% (82.6% with LA Grades A/B and 100.0% with LA Grades C/D) wanted long-lasting treatment options, while 69.9% (68.1% with LA Grades A/B and 100.0% with LA Grades C/D) reported that better initial healing of oesophagitis would make them feel hopeful that the treatment would resolve their problem.
Other statements that most patients agreed with were ‘I want whatever works fastest’ (61.6%); ‘Fast healing is important to me’ (58.9%); ‘I would welcome new treatment options’ (58.9%); ‘If a treatment relieves symptoms quickly, I have more belief in its long-term efficacy’ (57.5%); ‘I would like a treatment with better long-lasting effect than proton pump inhibitors’ (53.4%). In addition, 35.6% of patients desired better maintenance rates than PPIs. Only 43.8% of patients completely agreed that their current treatment was a lasting solution for their EE.
Physician attitudes to treatment are summarised in online supplemental table 2. In total, 69.7% felt that it is important to have treatments offering strong initial and ongoing symptom relief, while 66.9% agreed that better initial symptom relief would increase adherence. Fast symptom relief for their patients was a top priority for 66.1% of physicians. Other key findings were that 55.8% of HCPs would prefer a treatment with better long-term maintenance, 59.0% thought that a treatment with a new mechanism of action would help patients, 56.6% would welcome an alternative to PPIs, 58.2% reported that faster healing is important. In addition, 49.4% of HCPs agreed that faster healing would make them believe that treatment would resolve the problem.
Only 54.2% of HCPs agreed that their patients with EE’s treatment goals were achievable with current treatments. Improvement in overall symptoms (73.3%) was selected as the top treatment goal by both GIs and FPs/GPs (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Most important treatment goals as reported by physicians and patients. Base: 251. Source: Physician survey D1aa. Most important treatment goals. EE, erosive oesophagitis; FP, family physicians; GP, general practitioner.
Discussion
EE can be a debilitating condition with a substantial symptom burden that has a considerable impact on the day-to-day lives of patients. It is also a risk factor for BE and EAC. Appropriate therapy for patients with EE is important to improve their quality of life, and to attempt to reduce the risks of complications associated with EE. Almost all patients with EE require long-term acid suppressive therapy; thus, ensuring adequacy of disease control is important. Rapidity of onset and durability of efficacy are important therapeutic goals.
Although acid suppression with PPI therapy has traditionally been the mainstay of treatment of GERD, shortcomings in this approach have driven research into alternative therapies.21 The gamma-aminobutyric acid-B agonist, baclofen, has proven efficacy in PPI-refractory GERD, but its use has been limited by side effects and an inconvenient three times daily dosing regimen.21 Research into selective serotonin type 4 receptor agonists such as reverexepride and prucalopride and dopamine D2-receptor antagonists including domperidone has been disappointing, suggesting that kinetics have no added value in the management of refractory GERD.21 However, vonoprazan, a potassium-competitive acid blocker (P-CAB), available in Japan since 2015, has demonstrated rapid, strong, and continuous gastric acid suppression.22 23 The more recent availability of new P-CABs, including keverprazan24 and tegoprazan,25 has allowed standard treatment for acid-related conditions to evolve and improve.21 26 In addition to pharmacological approaches, multidisciplinary care management programmes including dietary, weight loss, exercise and behavioural interventions, are valuable and are being increasingly used in the management of EE.27
This study provides real-world evidence from all aspects of a patient’s journey to assess current practices and outcomes from current clinical practice in the USA. The population enrolled in this study consisted predominantly of patients with LA Grade A (81%) and Grade B EE (14%). The notable predominance of Grade A and B EE is not unexpected in real-world clinical practice; patients who may have severe EE (Grades C and D) will heal or partially heal with empiric or current PPI use, so their underlying severity may not be known.3 28 29 Our results therefore highlight the impact of the disease on this clinically relevant population that is already being managed with the current standard-of-care.
There were several important findings from this study. First, in terms of treatment patterns, 58% of HCPs indicated they preferred omeprazole as the ideal first-line therapy, while in practice, newly diagnosed patients typically received either omeprazole, pantoprazole, or esomeprazole. In addition, 59% of patients and 35% of HCPs believe better control could be achieved. Seventy-two per cent of HCPs were not completely satisfied with current treatment options. Further, although 25% of patients took a PPI at least two times a day, nearly 60% still continued to experience heartburn. Interestingly, 73% of HCPs recommended that patients supplement prescribed therapies with OTC medications, presumably because of incomplete symptom resolution with prescribed therapies.
Both HCPs and patients would welcome new treatment options, with both groups expressing the need for treatments that act more quickly and have a longer effect than those currently available. While 84% of patients wanted long-lasting treatment options, only 44% completely agreed that their current treatment was a lasting solution for EE. In addition, 56% of HCPs would prefer a treatment that provided better long-term maintenance of healing, but only 54% agreed that their patients with EE’s treatment goals were achievable with current treatment options. Fast healing was desired by 62% of patients and 58% of HCPs. However, there may be some disconnect between concepts of healing and symptom control since both groups reported that they would be more likely to believe in long-term efficacy if a treatment were to act quickly to relieve symptoms.
The importance of a rapid treatment effect is supported by the finding that 67% of patients would be more likely to take a treatment as advised if it worked more quickly. The main reason given by doctors for why patients altered treatment frequency was that they felt that the treatment was not working. As 51% of patients were not fully adherent (and 57% of those independently changed their dose), measures to improve treatment adherence may improve outcomes.
A substantial gap remains between the expectations of physicians and patients. The real-life perceptions of patients with EE raises two important points. First, there is a need for improvement in education around EE, particularly among patients, with respect to the outcomes that can currently be achieved with existing treatments. It also mandates the need to manage patient expectations more clearly when initiating treatment. A disconnect exists between healing and symptom resolution which could be mitigated by HCPs spending more time counselling their patients, or focusing on this aspect of the patient journey. Second, there is a clear unmet medical need to improve the current management of EE with additional treatment options that control symptoms more effectively, and that might also mitigate the risk of serious complications.
Strengths and limitations
The major strength of this study is that it reflects real-world clinical practice, and is based on the clinical decisions that physicians make in everyday practice. However, a number of limitations should be noted. For example, although physicians were recruited on the basis of predefined inclusion and exclusion criteria, participation may have been influenced by willingness to take part, the infrastructure to do so, and the remuneration offered. This may have yielded a relatively non-representative sample of clinicians. Similarly, reliance on physicians to recruit patients who had recently consulted may have led to selection bias, with less satisfied patients being more likely to respond to the survey. In addition, patients who consult their physicians only infrequently may have been under-represented in the sample.
The population enrolled in this study was relatively small, and consisted predominantly of patients with LA Grade A (81%) or B EE (14%). This predominance of Grades A and B EE is consistent with real-world clinical experience given the empiric use of PPIs, which is likely to underestimate the prevalence of severe EE at time of diagnostic endoscopy.3 28 29 Our results therefore highlight the impact of the disease on this clinically relevant population being managed with the current standard-of-care. However, only 5% of severe oesophagitis the patients were included in the study had severe EE, which is on the low side for Western countries. Further studies should aim to recruit larger numbers of patients to allow more robust conclusions to be drawn.
The cross-sectional design of the study means that information captured from both physician and patient surveys represents a single point in time. Therefore, components of the study cannot be used to demonstrate cause and effect. However, the eCRF captured historical data relating to patients’ disease history, allowing an overview of the patient’s disease journey over time.
Finally, this study is also limited by the fact that the quality of data collected depends to a large extent on the accurate reporting of information by physicians and patients.
Conclusion
This real-world multicentre study highlights important aspects of EE management throughout the patient journey, and reveals a need for new treatments that act more quickly to improve symptoms and that offer effective maintenance of healing, allowing patients to reach more of their treatment goals.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Western Institutional Review Board, Protocol number 20203206. Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors CWH, SJS, MFV, AMF, SB: Consulted on study design, results interpretation and analysis of data, drafting of the manuscript, and critical analysis of the manuscript; CA (guarantor): Contributed to study design, data collection, analysis and interpretation of results, and drafting of the manuscript, and critical analysis of the manuscript; RJ, CP: Contributed to analysis and interpretation of the results, drafting of the manuscript, and critical analysis of the manuscript.
Funding Financial support for the study was provided by Phathom Pharmaceuticals. Phathom Pharmaceuticals participated in the interpretation of the data, review, and approval of the manuscript.
Competing interests CP and RJ are employees of Phathom Pharmaceuticals. All other authors are consultants to Phathom Pharmaceuticals.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.