Article Text

Abstract
Background and objective Appendectomy may modulate the risk of inflammatory bowel disease through an effect on the gut microbiota. This study investigated the associations between appendectomy and incidence of Crohn’s disease (CD) or ulcerative colitis (UC), with an emphasis on the influence of age and time post appendectomy.
Methods This cohort study included 400 520 subjects born in Québec in 1970–1974 and followed until 2014. Administrative health data were used to ascertain appendectomy and cases of CD and UC. Cox proportional hazards models with time-dependent variables (appendectomy and time elapsed post appendectomy) allowed for the estimation of HRs and 95% CIs.
Results A total of 2545 (0.6%) CD cases and 1134 (0.3%) UC cases were identified during follow-up. Appendectomy increased the risk of CD (HR=2.02; 95% CI: 1.66 to 2.44), especially when performed at 18–29 years of age. The risk of CD was increased in the first 2 years, and decreased significantly after ≥15 years post appendectomy. Appendectomy appeared to protect against UC (HR=0.39; 95% CI: 0.22 to 0.71). The risk of UC was not associated with age at appendectomy, but decreased with time elapsed post appendectomy (HR=0.21; 95% CI: 0.06 to 0.72, comparing ≥5 with 0–4 years after appendectomy).
Conclusions The increased risk of CD related to appendectomy in young adults may result from detection bias, but physicians should have a low threshold for suspicion of CD in young symptomatic adults with a history of appendectomy. A strong protective effect of appendectomy against UC was observed after 5 years.
- CROHN'S DISEASE
- ULCERATIVE COLITIS
- INFLAMMATORY BOWEL DISEASE
- EPIDEMIOLOGY
Data availability statement
No data are available. Due to the nature of this research, participants of this study did not agree for their data to be shared publicly, so supporting data is not available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Changes in the intestinal microbiome induced by appendectomy may influence the occurrence of inflammatory bowel disease. Few studies have addressed the influence of age at surgery and time elapsed post appendectomy.
WHAT THIS STUDY ADDS
Crohn’s disease risk was increased among those who had an appendectomy, particularly in young adults and during the first years after surgery, suggesting a possible detection bias. Appendectomy appeared to protect against ulcerative colitis, strongly after 5 years post appendectomy.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Physicians should have a low threshold for suspicion of Crohn’s disease in young symptomatic adults with history of appendectomy. Likewise, the long-term impact of the new management strategy for moderate cases of acute appendicitis (antibiotics instead of surgery) should be investigated.
Introduction
Inflammatory bowel diseases (IBD) such as Crohn’s disease (CD) or ulcerative colitis (UC) are chronic diseases of the intestinal tract. The aetiology of IBD is not fully understood but the intestinal microbiota may play an important role.1 Several environmental factors that influence the risk for IBD have been identified, including appendectomy.2
Appendectomy causes intestinal dysbiosis that might be a precursor of intestinal inflammation. In addition, the parietal breach caused by surgery leads to an epithelial rupture and abundant secretion of cytokines by proinflammatory cells.3 These observations suggest the involvement of appendectomy in the occurrence of CD (online supplemental figure 1). On the other hand, appendectomy could allow recolonisation of the bowel, which in turn may prevent IBD.4 These studies highlight the relevance of studying the relationship of appendectomy with CD and UC.
Supplemental material
Previous studies suggest a protective effect of appendectomy on UC and conflicting results with respect to the association with CD.2 5 6 Few studies to date have documented the influence of age at surgery and time elapsed post appendectomy on the risk of CD7–10 and UC.11 12 Knowledge of the effect of age at surgery and time post appendectomy could allow a better understanding of the potential associations and provide a meaningful explanation for the previous inconsistent results for CD.
In this context, we investigated appendectomy and the occurrence of CD or UC, in a large population-based cohort, with a specific emphasis on the influence of age at surgery and time elapsed post appendectomy. This study thus aims to provide answers to the identified gaps in the literature, specifically relating to the timing of appendectomy on IBD incidence.
Materials and methods
Study population
The Quebec Birth Cohort on Immunity and Health (QBCIH) was established in 2010. The main objective of this cohort was to study the association between BCG vaccination and immune-related diseases. A detailed description of the cohort is available elsewhere.13 Briefly, eligible persons were live births, born after 32 weeks of gestation, and documented in the Quebec birth registry from 1970 to 1974. Participants covered by the public health system were identified by probabilistic linkage with the Healthcare Registration File from the Régie de l'assurance maladie du Québec (RAMQ). This linkage was performed using identifying variables such as surname, first name, date of birth, sex and father’s first name. The data used in this study were extracted from the Healthcare Registration File (1987–2014), birth (1970–1974) and death (1970–2014) registries, and administrative health databases including physician visits (1983–2014) and hospitalisations (1987–2014). A total of 400 611 subjects were included in the QBCIH cohort, representing 90% of eligible persons.
Exposures
Appendectomy was defined as the presence of at least one procedure or intervention code referring to an appendectomy. This qualitative variable was analysed as binary (yes, no). Appendectomy codes for procedures or interventions (05201, 5909; INV89DA, INV89LA) were based on the Canadian Classification of Interventions in Health and the Canadian Classification of Diagnostic, Therapeutic and Surgical Procedures.
Appendicitis (with or without appendectomy) was defined as the presence of at least one diagnostic code referring to appendicitis (International Classification of Diseases, Ninth revision (ICD-9): 540 to 542; ICD-10: K35 to K37) in physician visit billing claims or hospitalisations during follow-up. Other diseases of the appendix (ICD-9: 543; ICD-10: K38) such as appendicular colic, appendicular mucocele and sphacele, appendicular cyst and other were grouped into a binary variable (presence or absence of other appendicular disease). We had no histology information relative to those diagnostic codes.
Age at appendectomy was defined as the age at first physician visit or hospitalisation with an intervention code for appendectomy. Time elapsed post appendectomy was updated during follow-up by counting the days between the date of appendectomy and the last follow-up date, then converted into years.
Outcomes
The events of interest (CD, UC) were identified by applying validated algorithms to administrative health databases. These algorithms have been used in several studies and were validated in Ontario, Canada.14–16 Diagnostic codes from ICD-9 and ICD-10 were used, respectively, 555/K50 for CD and 556/K51 for UC. Subjects aged less than 18 years old who satisfied the following criteria were considered as paediatric IBD cases: (1) at least one sigmoidoscopy/colonoscopy and (2) four IBD-related medical services or two hospitalisations within 3 years. Children who had seven IBD-related medical services or three hospitalisations within 3 years, without sigmoidoscopy or colonoscopy, were also classified as IBD cases.16 This algorithm had a sensitivity of 91.1% and a specificity of 99.5%.16 IBD cases in adults (≥18 years of age) were subjects who had ≥5 physician visits or hospitalisations for IBD within a 4-year interval. This definition had a sensitivity of 76.8% and a specificity of 96.2% in an adult population. The positive predictive value was 81.4% and the negative predictive value was 95.0%.14 CD and UC cases were determined from the five most frequent among the last nine diagnoses. IBD cases who did not have a consistent diagnosis (CD or UC) for at least five visits were classified as indeterminate colitis.
Covariates
Perinatal variables (sex, gestational age, birth weight) extracted from the birth register and sociodemographic variables derived from the postal code obtained from the Healthcare Registration File were used to describe the study population. Area of residence was a binary variable (urban, rural) defined using the Canadian postal code of residence in 1987.17 The median area-based income was derived from the 1991 Census and expressed in Canadian dollars. The material and social deprivation indices were based on six socioeconomic indicators from the national census.18
Statistical analyses
Cox proportional hazards regression models were used to assess the associations between appendectomy and CD or UC. This allowed for the estimation of HRs and 95% CIs. Distinct analyses were performed for CD and UC. Appendectomy and elapsed time post appendectomy were treated as time-dependent variables.
We considered age as the time axis and the participant’s age at the start of follow-up as the time origin was defined as 1 January 1983, since no administrative data were available before that date. Left truncation at the beginning of the follow-up and censoring at the end date (31 December 2014) were performed. The follow-up ended either: (1) at the date of diagnosis for subjects who met the case definition, (2) at death or (3) on 31 December 2014, whichever came first. The time-dependent variable (elapsed time post appendectomy) and age at appendectomy were studied in two separate models to avoid collinearity. These analyses were performed only in the subgroup of subjects who had an appendectomy.
Models were adjusted for the following potential confounding factors: gestational age and sex, as identified by a directed acyclic graph (online supplemental figure 2). Continuous variables were entered as such in the models after confirmation of the linearity of the logit, and in categories otherwise. Only 7 cases of the 400 520 subjects had missing data for gestational age. Therefore, the main analyses were based on subjects with complete data.
Sensitivity analyses were carried out to study the association of appendectomy for appendicitis and of appendicitis (with or without appendectomy) in relation to CD or UC.
Results
Main characteristics of the study population
From the 400 611 subjects in the QBCIH, subjects deceased before the start of follow-up on 1 January 1983 (49 subjects) and cases of indeterminate colitis (42 subjects) were excluded. The final cohort sample included 400 520 subjects (online supplemental figure 3).
Half of the subjects were male (51.4%). The majority (68%) of participants resided in urban areas. The mean gestational age was 39 weeks of amenorrhea (SD=1.7). A total of 27 303 participants (6.8%) had appendicitis (with or without appendectomy) and 17 205 (4.3%) had undergone surgery for appendectomy during follow-up. The main indication for performing an appendectomy was appendicitis, representing 98.2% of appendectomies. Among the 3679 cases of IBD, two-thirds were CD and one-third were UC (table 1).
Description of perinatal, sociodemographic and medical factors in the Quebec Birth Cohort on Immunity and Health, Canada, 1970–2014
The groups of subjects who had an appendectomy and those without appendectomy were similar in terms of birth weight, gestational age, median census-based family income, and social and material deprivation (table 1). The proportion of men among those who had an appendectomy was slightly higher (55.1%) compared with those who did not (51.2%). The proportion of subjects identified as having CD was similar in those with or without a history of appendectomy. In contrast, there were fewer subjects with UC among those who had an appendectomy (0.1%) than among those who did not (0.3%).
The cumulative incidence of CD and UC as a function of age is shown in figure 1. Incidence of CD was 600 per 100 000 persons in the first 40 years of life and 300 per 100 000 persons for UC.

Incidence rate of Crohn’s disease and ulcerative colitis according to age, Quebec Birth Cohort on Immunity and Health (QBCIH), 1970–2014 (N=400 513). Compilation based on data from the Government of Québec, Institut de la statistique du Québec, 2017. Institut de la statistique du Québec is not responsible for compilations or interpretation of results. Compilation based on data from the Government of Québec, Institut de la statistique du Québec, 2017. Institut de la statistique du Québec is not responsible for compilations or interpretation of results.
Association between appendectomy and CD
Appendectomy (any cause) was associated with an increased risk of CD adjusted for gestational age and sex (HR=2.02; 95% CI: 1.66 to 2.44) (table 2). Similarly, appendectomy for appendicitis (HR=1.92; 95% CI: 1.58 to 2.34) and appendicitis (with or without appendectomy) were associated with CD (HR=2.89; 95% CI: 2.54 to 3.31) (online supplemental table 1).
Association between appendectomy and Crohn’s disease or ulcerative colitis, Quebec Birth Cohort on Immunity and Health, Canada, 1970–2014 (N=400 513)
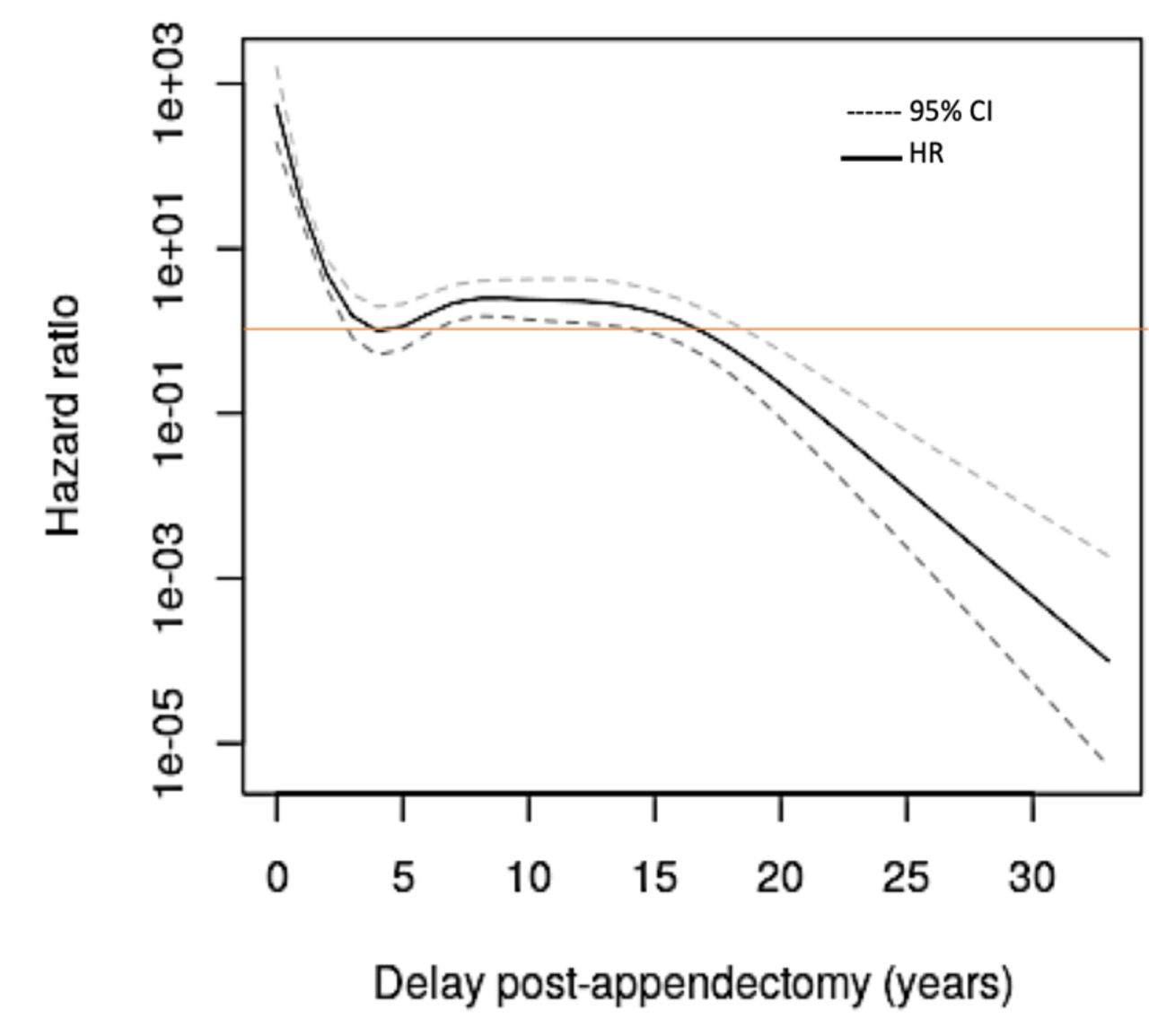
Among those who had an appendectomy, CD was associated with age at surgery and time elapsed after appendectomy. As displayed in Figures 2 and 3, there was an important variation of the association between appendectomy and CD according to both age at surgery and time elapsed post appendectomy. Subjects who had an appendectomy between 18 and 29 years of age had the highest risk of CD (figure 2). For instance, subjects who had appendectomy performed at 25 years of age had a twofold risk of CD compared with those who had appendectomy performed at 18 years of age. The spline function for the HRs suggests that appendectomy occurring before 18 years or after 29 years of age was not associated with CD. An increased risk of CD was found in the first 2 years post appendectomy, it was null 6–15 years after appendectomy, and significantly decreased 15 years post appendectomy (figure 3).
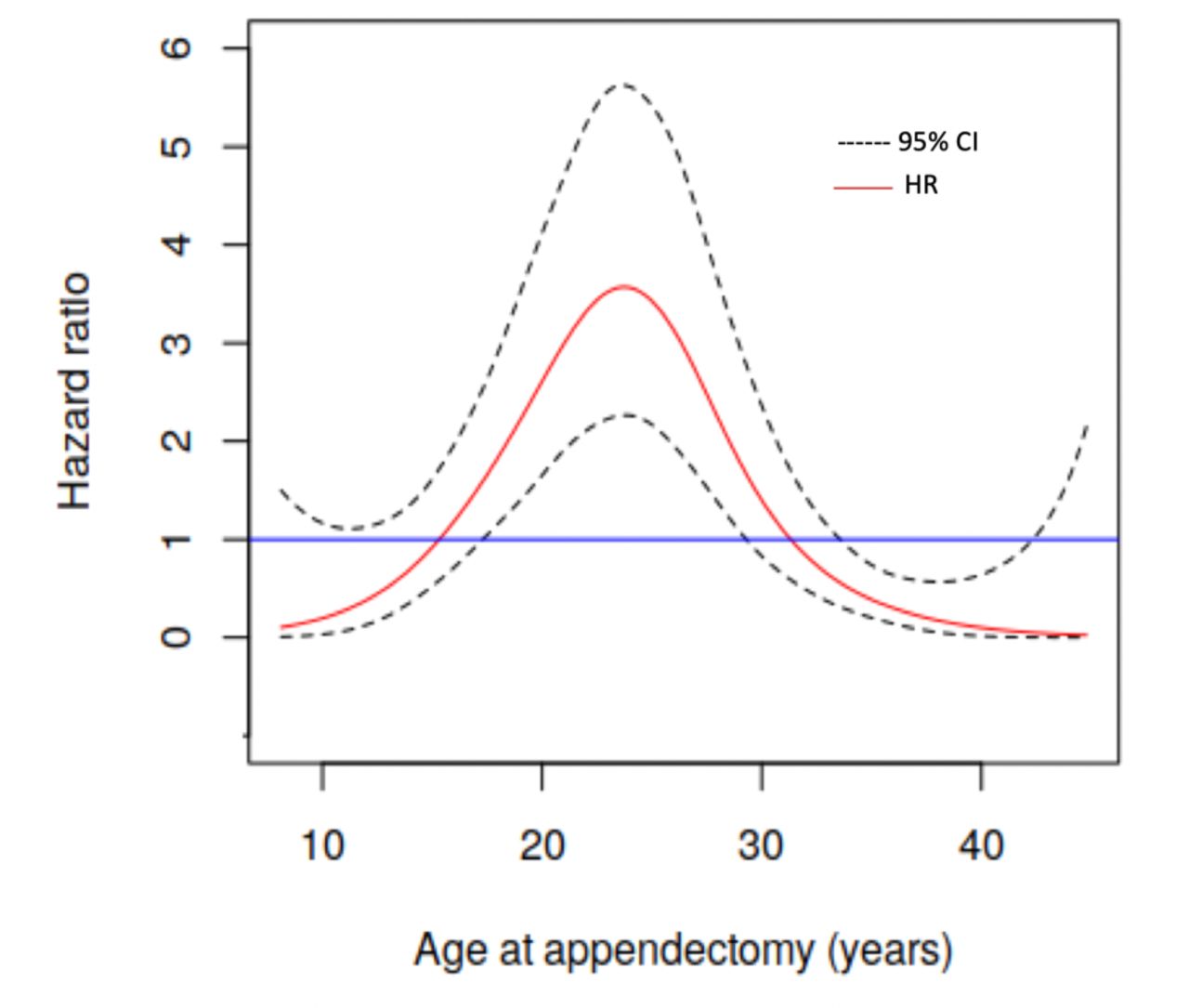
Estimate of effect of age at appendectomy on the risk of Crohn’s disease, QBCIH, 1970-2014 . HRs and 95% CI depicted based on a spline function, and using termplot function wich returns a centered set of predictions to estimate the exact HRs at each point of the age at appendectomy axis. Compilation based on data from the © Government of Québec, Institut de la statistique du Québec, 2017. Institut de la statistique du Québec is not responsible for compilations or interpretation of results.

{kind=link}
{kind=link}
{kind=link}
Estimate of effect of time elapsed after appendectomy on the risk of Crohn’s disease, QBCIH, 1970-2014. HRs and 95% CI depicted based on a spline function, and using termplot function wich returns a centered set of predictions to estimate the exact HRs at each point of the delay post-appendectomy axis. Compilation based on data from the © Government of Québec, Institut de la statistique du Québec, 2017. Institut de la statistique du Québec is not responsible for compilations or interpretation of results.
Association between appendectomy and UC
The risk of UC was 61% lower in subjects with an appendectomy compared with those without it (HR=0.39; 95% CI: 0.22 to 0.71) (table 2). Similarly, appendectomy for appendicitis and appendicitis (with or without appendectomy) decreased the risk of UC: the HRs were 0.40 (95% CI: 0.22 to 0.72) and 0.60 (95% CI: 0.42 to 0.88), respectively, (online supplemental table 1).
Overall, no association was observed between UC and age at appendectomy (HR=1.06; 95% CI: 0.97 to 1.15) (online supplemental figure 4, table 2). However, a stronger inverse relationship against UC was observed 5 or more years after appendectomy compared with the first 4 years post appendectomy (HR=0.21; 95% CI: 0.06 to 0.72). The small number of exposed cases precluded conducting spline analyses for the time elapsed post appendectomy.
Discussion
In this cohort study, appendectomy was associated with an increased risk of CD. This association was stronger during the first 2 years post appendectomy as well as among subjects who underwent an appendectomy in early adulthood (18–29 years). Appendectomy appeared to protect against CD after 15 years post appendectomy. An inverse association was found for UC, which was more pronounced with greater time elapsed after appendectomy. Similarly, appendectomy for appendicitis was associated with an increased risk of CD and a decreased risk of UC.
Previous studies investigating the link between appendectomy and CD have found similar results to ours. Piovani et al, in an umbrella review of meta-analyses in 2019 based on 17 studies, reported that subjects with an appendectomy had a 61% higher risk of CD compared with those without such surgery (HR=1.61; 95% CI: 1.28 to 2.02), although there was heterogeneity between studies.19 Results from Amarapurkar et al also suggested a positive association between CD and a history of appendectomy (OR: 3.16; 95% CI: 1.71 to 5.80).20
We observed that appendectomies occurring at 18–29 years of age increased the risk of CD. These findings are in line with Frisch et al who reported that appendectomies performed at 21–34 years of age were associated with an increased risk of CD.11
In the QBCIH cohort, the risk of CD was higher in the 2 years following appendectomy and decreased with increasing time elapsed post surgery. Few previous studies have investigated the effect of time post appendectomy with the time scale as a continuous variable using arbitrary cut-off points. Indeed, Kaplan et al estimated that the risk was elevated during the first year postappendectomy (RR=6.69, 95% CI: 5.42 to 8.25), and decreased after 5 years, suggesting that some appendectomies were likely performed on persons with undiagnosed CD whose symptoms may have been similar to those of appendicitis.8 Chen et al also found that the rates of appendectomy were higher in the first 5 years before the diagnosis of CD.9 Likewise, the risk of CD was highest in the first 6 months post appendectomy in a population-based cohort study in Sweden and Denmark.8 21 These results may reflect problems in the differential diagnosis between appendicitis and CD rather than a true association.4 Alternatively, the inflammation of the appendix and other clinical symptoms may be due to subclinical CD rather than appendicitis,8 and thus the positive association observed between appendectomy and CD may reflect reverse causation. To our knowledge, we are the first to estimate the effect of appendectomy on the risk of CD at different ages at surgery. Moreover, we report for the first time a decreased risk of CD 15 years after appendectomy.
In the literature, appendectomy has been inversely associated with the risk of UC.2 4 22 For instance, according to Firouzi et al, the OR for this association was 0.38 (95% CI: 0.19 to 0.76).22 Surgical removal of the appendix appears to protect intestinal tissue from the occurrence of UC. This is supported by the current study in which subjects who underwent appendectomy had a 61% lower risk of developing UC. Therefore, our findings about the association between appendectomy and UC, in a Canadian population, are in line with previous evidence. Some authors have previously hypothesised a direct protective influence of appendicitis on UC, such that removing the trigger may protect against the development of UC in the future.12 It is not possible to dissociate, in our data, the association due to appendectomy from that due to appendicitis, the two events being strongly correlated. Andersen et al have suggested that extraneous factors, environmental or genetic, associated with an excess risk of appendicitis and a decreased risk of UC may explain this inverse association.23 We observed that the association was stronger 5 years after surgery compared with the first 4 years. In contrast, Frisch et al found an increased risk of UC 5–14 years post appendectomy (OR=2.0; 95% CI: 1.4 to 2.9).11 In the present study, no association was found between age at appendectomy and UC. Only two studies to date have documented the association between age at appendectomy and risk of UC.11 12 According to Andersson et al, only appendectomy performed before 20 years of age was associated with a lower risk of UC,12 whereas Frisch et al reported no association between appendectomy performed at 21–54 years and the risk of UC.11
The deleterious effect of appendectomy on CD could be explained by the inflammatory pathway caused by the epithelial defect of the intestinal mucosa.3 Appendectomy might change the epithelial barrier function, which disturbs the innate and adaptive immune systems, and the intestinal microbiome,24 which could lead to an increased production of inflammatory cytokines in response to antigenic stimuli. Intestinal dysbiosis induced by appendectomy could be another pathway for intestinal inflammation.3 However, our results, along with those of others, suggest that CD cases occurring immediately after appendectomy could be attributable to detection bias or reverse causality rather than a true causal association.4 Appendectomies that occurred at 18–29 years were associated with increased risk of CD. Therefore, physicians should have a low threshold for suspicion of CD in young symptomatic adults in the years following appendectomy.
The vermicular appendix constitutes a reservoir of commensal micro-organisms. This explains its involvement in the human immunological mechanisms. Removal of the appendix leads to an alteration of the intestinal microbiome.4 Moreover, an unusual microbial composition of this area of the digestive tract appears with appendicitis. Thus, a favourable microbial composition occurring after appendectomy could be protective against UC. The inverse association of appendectomy and UC recently inspired new therapeutic approaches such as appendectomy as an alternative to colectomy in the treatment of severe UC.25 Appendectomy early in life and before developing UC is associated with a lower risk of colectomy as well as UC-related hospital admissions.26 However, the new trend for the management of acute appendicitis in children is antibiotic treatment for mild to moderate cases, as several studies suggest the efficacy of antibiotics for managing uncomplicated acute appendicitis.27 Likewise, a recent randomised trial showed that antibiotics were as effective as appendectomy.28 This strategy may have an impact on the incidence of UC and CD in the future.
Limitations and strengths
This study has some limitations. First, the administrative health databases used in this study do not cover the period before 1983. This period of life (birth to 9–13 years) is a risk period for paediatric IBD but also for appendectomy. The incidence of IBD in the province of Ontario (Canada) was 6.6 per 100 000 person-years in children between 5 and 9 years of age.16 Missing early IBD cases might lead to a decrease in statistical power and an over or underestimation of the association between appendectomy and IBD. Second, the algorithm used to define cases of CD and UC occurring after 18 years of age had a sensitivity of 76.8% and a specificity of 96.2%.14 The low sensitivity may have led to case misclassification, and therefore moderately biased the HR estimation towards the null value. Third, appendectomies performed outside of Quebec and therefore not listed in the public health system (RAMQ) were not taken into account. Also, if study participants had medical visits outside Quebec, this information was not available unless they were billed to the provincial health system. The lack of information for identifying exposure may have led to biases towards the null value. Fourth, in our study population, 98.2% of the subjects who had an appendectomy had a health service with a diagnostic code of appendicitis. The appendicitis diagnoses were reported by physicians in administrative databases, either for reimbursement of their fees after a medical visit or in the context of a hospitalisation. Histopathology reports were not available to us, but previous studies have estimated the proportion of appendectomies with appendicitis as a discharge diagnosis at 70%–90%.29–32 The use of administrative data for identification of appendicitis was reported to have high sensitivity, but low specificity,31 as they may point to suspected disease that has yet to be confirmed histologically. This suggests that our definition of appendicitis is likely to have included some false positives.
Nevertheless, this study had several strengths. The QBCIH is a large cohort in which more than 400 000 subjects were followed over 32 years. This cohort includes more than 90% of eligible Quebecers. This high representativeness prevents selection bias. Also, statistical power to detect a possible association between appendectomy and the events studied was high, especially for CD. The use of administrative health data limited the potential for missing data. Regarding the variables included in the regression models, only seven subjects (0.01%) had missing data for only one variable (gestational age). This limits information bias. The use of validated and standardised algorithms to define the events minimised differential information bias. A comparison between included (CD or UC) and excluded IBD cases (indeterminate colitis) revealed no differences in relevant characteristics (sex, appendectomy, appendicitis, gestational age and birth weight). This exclusion therefore had no impact on the results, thus limiting selection bias. In addition, the proportion of excluded subjects was very low (1% of IBD cases).
Conclusion
The results from this large cohort study suggest that subjects who had an appendectomy between 18 and 29 years of age experienced an excess risk of CD. The highest risk of CD occurred in the 2 years after appendectomy, which is likely attributable to detection bias rather than a harmful effect of the intervention. Nonetheless, a low threshold for suspicion of CD should be used by physicians when encountering young adults with onset of digestive symptoms after having undergone appendectomy.
A protective association of appendectomy against UC was identified, in line with the previous literature. For the first time, a low risk of CD was observed 15 years after appendectomy suggesting a long-term protective effect. To our knowledge, this study is the first to find a strong protective association between UC and elapsed time after appendectomy. The new antibiotic treatment approach for appendicitis should be carefully monitored for possible impact on IBD occurrence.
Data availability statement
No data are available. Due to the nature of this research, participants of this study did not agree for their data to be shared publicly, so supporting data is not available.
Ethics statements
Patient consent for publication
Ethics approval
This study has obtained the necessary authorisations from the Quebec governmental authorities (Commission d’accès à l’information) and the Research Ethics Committees of the Institut national de la recherche scientifique, Institut de la statistique du Québec and Régie de l'assurance maladie du Québec.
Acknowledgments
We gratefully acknowledge Isabelle Leroux and Jimmy Baulne from Institut de la statistique du Québec, as well as François Blouin and Claude Verville from the Régie de l’assurance maladie du Québec for their contribution to various aspects of the establishment of the Quebec Birth Cohort on Immunity and Health. Institut de la statistique du Québec was instrumental in realizing the linkages between administrative databases. We are grateful to the personnel from the Centre d’accès aux données de recherche de l’Institut de la statistique du Québec where all analyses were conducted. We also wish to acknowledge Hugues Richard, biostatistician from Centre Armand-Frappier Santé Biotechnologie at INRS for discussions about regression models and Florence Conus from Institut de la Statistique du Québec. Finally, we would like to thank Dr Karen Leffondré from Institut de Santé Publique, d'Épidémiologie et de Développement at Université de Bordeaux for her precious statistical advice.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors PJ and M-CR conceived the study. CF, PJ, M-EP and M-CR developed the protocol. PJ and M-CR obtained the funding and data. CF analysed the data. CF, PJ, M-EP and M-CR interpreted the results. CF drafted all versions of the manuscript and PJ, M-EP and M-CR revised it critically for important intellectual content and approved the final version. CF, PJ and M-CR are the guarantors.
Funding Establishment of the Quebec Birth Cohort on Immunity and Health was supported by an infrastructure grant from the Canada Foundation for Innovation & the Québec Ministry of Education, Leisure and Sports (#12532), research grants from the Canadian Institutes of Health Research (#MOP-97777, #MCH-97593, #MOP-142705), Fonds de recherche du Québec-Santé (FRQS, #16227) and Multiple Sclerosis Society of Canada (#2435). This research was supported by a grant from the Canadian Institutes of Health Research (#PJT-159791). CF received scholarships from Aquimob (#55612) and Réseau intersectoriel de recherche en santé de l’Université du Québec. PJ (#283723) and M-EP (#15868) are recipients of career awards from the FRQS.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.