Article Text

Abstract
Recurrent and persistent bouts of hiccups impact the quality of life by interfering with eating, social interaction and work. Popular home remedies, such as breath holding and drinking ice water, target activity in the vagal and phrenic nerves that are thought to trigger these repetitive, myoclonic contractions. However, the pathophysiology of hiccups and the mechanism by which any of these methods work are unclear. Indeed, so little is known that there is no agreement whether the ‘Hic’ sound is due to the abrupt closure of the epiglottis or the glottis, including the vocal cords.
Investigations were performed in a 50-year-old, otherwise healthy male with recurrent hiccups, in whom contractions persisted for up to 4 hours. Hiccups were initiated by drinking carbonated soda. The aerodigestive tract was visualised by video fluoroscopy. Hiccups were terminated by drinking a non-viscous contrast agent through a forced inspiratory suction and swallow tool. This device requires significant suction pressure (−100 mm Hg) to draw fluid into the mouth and is effective in approximately 90% of cases. The images were analysed together with concurrent audio recordings to gain insight into ‘what causes the ’hic’ in hiccups’ and how this commonplace but annoying problem can be treated.
- functional bowel disorder
- neurogastroenterology
- gastroesophageal reflux disease
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Recurrent and persistent bouts of hiccups impact the quality of life by interfering with eating, social interaction and work.1 These repetitive, myoclonic contractions are maintained by a reflex arc that consists of an afferent sensory limb (includes vagus nerve and sympathetic chain), an integration centre in the spinal cord and brainstem, and an efferent motor limb that involves the phrenic nerve to the diaphragm and accessory nerves to the intercostal muscles. This activity draws air into the lungs that is, within a few milliseconds, interrupted by closure of the upper airway producing the characteristic sound, the ‘hic’ in hiccups.1 Popular home remedies, such as breath holding and drinking ice water, seek to interrupt this neuromuscular relay.2 However, the pathophysiology of hiccups and the mechanism by which any of these methods work are unclear. Indeed, so little is known that there is no agreement whether the ‘Hic’ sound is due to the abrupt closure of the epiglottis or the glottis, including the vocal cords.
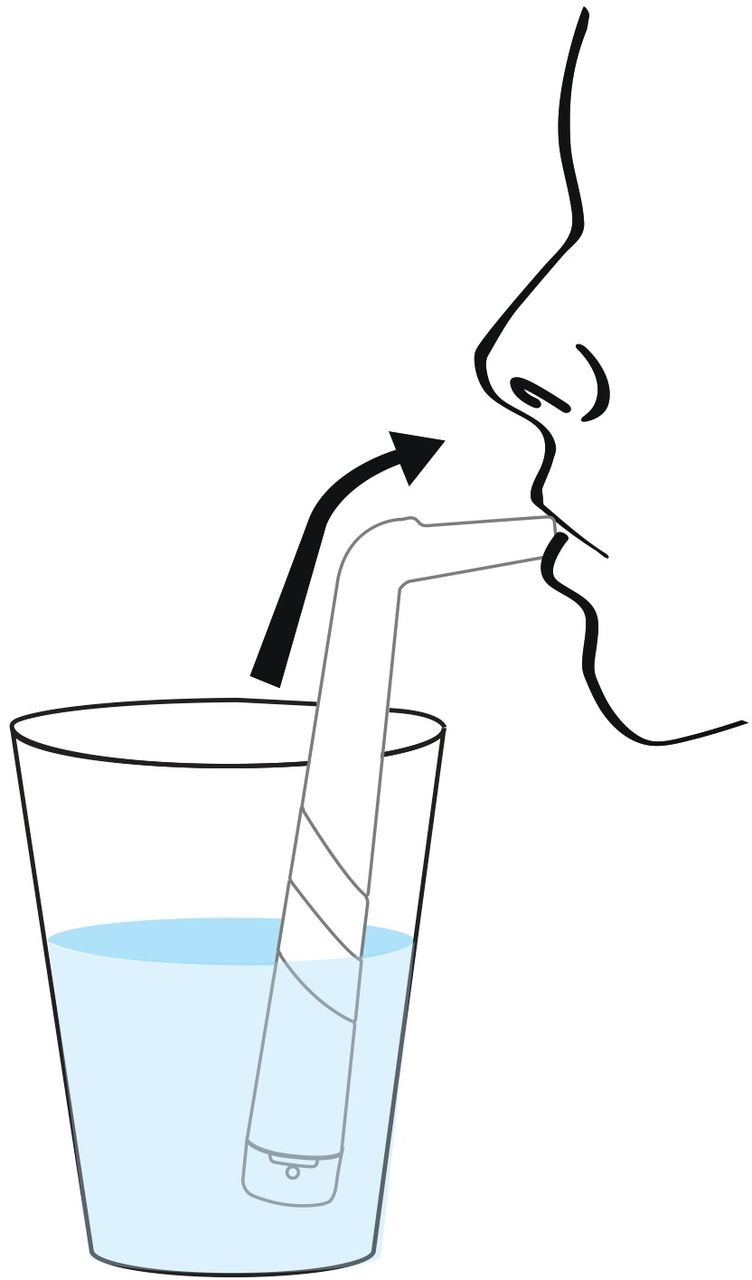
Investigations were performed in a 50-year-old, otherwise healthy male with recurrent hiccups, in whom contractions can persist for up to 4 hours. This unique experiment was possible because hiccups could be reproducibly initiated in this volunteer by drinking carbonated soda. The aerodigestive tract was visualised using video-fluoroscopy by drinking a non-viscous, barium sulfate suspension through a ‘forced inspiratory suction and swallow tool’ (FISST). This device has been described previously and patients report that its use terminates hiccups in more than 90% of cases (figure 1).3 FISST uses Bernoulli’s principle to generate a high-negative, intrathoracic, suction pressure (−100 cmH2O). This draws fluid through a small orifice in a rigid drinking tube into the mouth, an action that is immediately followed by swallowing.3 The images were analysed together with simultaneous audio recordings to gain insight into ‘what causes the ‘hic’ in hiccups’ (video 1).
{kind=link}
Forced inspiratory suction and swallow tool (‘HiccAway’, Aim Dynamics, Longmont, Colorado, USA). The tool has a mouthpiece on the top, a rigid body and a cap with a pressure valve on the bottom. The valve and the body’s dimensions were designed to generate high-negative suction pressure. The cap is removable and can be rotated to set the valve to the adult or child settings. The tip is submerged in a half-filled cup of water. The lips are pursed around the mouthpiece and forceful suction draws water into the mouth and is immediately swallowed. Hiccups usually stop after one to three attempts.
Answer
Analysis of the concurrent imaging and audio recordings showed that the ‘Hic’ sound occurs due to rapid closure of the glottis during hiccups. The epiglottis did not move during the repetitive contractions of the diaphragm and glottis (video 1).
As expected, forceful suction of water through the FISST device and swallowing was accompanied by epiglottic flexion to protect the tracheal entrance during drinking. At the same instant, this physiological event was associated with the termination of hiccups.
These novel observations indicate that (1) the ‘Hic’ sound of hiccups is produced by abrupt myoclonic contraction and closure of the glottis, not the epiglottis, and (2) the combination of breath-hold with suction pressure and swallowing appears to provide rapid and effective relief of transient hiccups. This work also shows how a device that combines key elements of popular ‘home remedies’ for hiccups, provides rapid relief of this commonplace but annoying problem (video 2). Specifically, FISST requires generation of high-negative, intrathoracic pressure, breath-holding and also the act of swallowing. At present the use of this device is supported by observational data from a large cohort of patients3; however, a randomised controlled trial using a dummy device as a comparator intervention is planned.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but IRB at the University of Texas (ref: HSC20210085N) exempted this study. Participants gave informed consent to participate in the study before taking part.
Footnotes
Contributors AS had the initial concept and performed the imaging investigation. AS and MRF contributed to data analysis and to the writing of the primary and final drafts of this article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests AS reported non-financial support from the University of Texas Health Science Center at San Antonio; he is the patent inventor for the hiccup-relieving apparatus (the forced inspiratory suction and swallow tool (FISST)/ HiccAway), University of Texas licensed the device to Aim Dynamics and receives a royalty.
Provenance and peer review Not commissioned; externally peer reviewed.