Article Text

Abstract
Objective There is a paucity of studies in the literature body evaluating short term outcomes following endoscopic retrograde cholangiopancreatography (ERCP) in patients with inoperable malignant hilar biliary obstruction (MHBO). We aimed to primarily evaluate 30-day mortality in these patients and secondarily, conduct a systematic review of studies reporting 30-day mortality.
Design We conducted a retrospective analysis of all patients with inoperable MHBO who underwent ERCP at Leeds Teaching Hospitals NHS Trust between February 2015 and September 2020. Logistic regression models constructed from baseline patient data, the modified Glasgow Prognostic Score (mGPS) and Charlson Comorbidity Index (CCI) were evaluated as predictors of 30-day mortality.
Results Eighty-seven patients (49 males) with a mean age of 70.4 years (SD ±12.3) were included. Cholangiocarcinoma was the most common aetiology of MHBO affecting 35/87 (40.2%). Technical success was achieved in 72/87 (82.8%). The 30-day mortality rate was 25.3% (22/87), of which 16 were due to progression of underlying malignant disease. On multivariate analysis, only leucocytosis (OR 4.12, 95% CI 2.70 to 7.41, p=0.02) was an independent predictor of 30-day mortality. Neither mGPS (p=0.47) nor CCI with a cut-off value of ≥7 (p=0.06) were significant predictors of 30-day mortality.
Conclusion We demonstrated that 30-day mortality following ERCP for inoperable MHBO remains high despite technical success. Further studies are warranted to identify patients most appropriate for intervention.
- BILIARY ENDOSCOPY
- CHOLANGIOCARCINOMA
- BILIARY STRICTURES
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known about this subject?
Thirty-day mortality following endoscopic retrograde cholangiopancreatography (ERCP) in patients with inoperable and/or palliative malignant hilar biliary obstruction to be in excess of 20% according to a recent UK Hospital Episode Statistics analysis.
Although there is an abundance of studies in the literature evaluating the technical aspects of ERCP in these patients, there is a lack of studies evaluating 30-day mortality as a primary outcome.
What are the new findings?
In our retrospective analysis of 87 patients, the 30-day mortality following ERCP was 25.3% despite a technical success of 82.8%. The majority of deaths were due to progression of underlying malignant disease.
On multivariate analysis, only leucocytosis was an independent predictor of 30-day mortality.
How might it impact on clinical practice in the foreseeable future?
Further research is required to identify patients with malignant hilar biliary obstruction who are most likely to benefit from an ERCP.
Introduction
Malignant hilar biliary obstruction (MHBO) is most commonly caused by cholangiocarcinomas (CCA) but other typical aetiologies include gallbladder malignancy and metastatic disease from other primaries.1 The majority of patients present with jaundice and at a stage where the disease is not surgically resectable. In these circumstances, palliative biliary drainage aims to prolong patient survival, improve quality of life (QOL), relieve symptoms of biliary obstruction and facilitate oncological therapy.2
Biliary drainage can be established via endoscopic retrograde cholangiopancreatogaphy (ERCP), percutaneous transhepatic cholangiogram (PTC) and more recently, endoscopic ultrasound guided hepaticogastrostomy.3 Nationwide analyses from the UK demonstrated a 30-day mortality rate of 19.1% following ERCP for palliation of malignant biliary obstruction (MBO), with higher mortality in patients who had MHBO4 and a similar observation of 30-day mortality rate of 23.1% following PTC for MBO.5 There remains debate on the favoured approach between ERCP or PTC for palliative biliary drainage in MHBO with practice variable in the UK. Endoscopic drainage of selected or bilateral intrahepatic ducts is technically challenging and time consuming but is preferred by many where expertise is available. However, patient selection for intervention is paramount to avoid unnecessary complex procedures where outcomes may unavoidably be poor.
Given the poor prognosis in this cohort of patients, evaluations of 30-day mortality as a primary outcome are important to establish. However, there is a paucity of such studies in the literature and limited data available on factors predictive of a good (or poor) outcome in this cohort to advise on patient selection. Factors that have been implicated in other studies of prognosis in malignancy include the Charlson Comorbidity Index (CCI)6 and modified Glasgow Prognostic Score (mGPS)7 and would seem suitable for evaluation in MHBO. The aim of our study was, therefore, to describe a large cohort of consecutive patients from our tertiary referral hospital selected for endoscopic palliation of inoperable MHBO, describe 30-day mortality following ERCP and define factors predictive of early mortality. A secondary aim was to perform a systematic literature review of studies that have reported 30-day mortality rates and related prognostic factors for endoscopic drainage of MHBO.
Methods
Since 2015, all patients undergoing ERCP in Leeds Teaching Hospitals National Health Service Trust have been collated on a prospectively maintained database, with 30-day outcomes recorded subsequently. The favoured approach for biliary drainage in patients with MHBO in our organisation has been via ERCP for many years. Following a diagnosis of MHBO at cross-sectional imaging with CT and/or MRI, all cases are discussed at a dedicated multi-disciplinary team (MDT) meeting. Patients deemed surgically inoperable by the MDT on the basis of local invasion, distant metastases and/or medical comorbidities are selected for optimised endoscopic biliary drainage if jaundiced.
Consecutive patients undergoing endoscopic drainage for MHBO between February 2015 and September 2020 were retrospectively identified from our database and clinical data obtained from electronic general practitioner and local institutional databases to determine pre-procedure mGPS and CCI.
Endoscopic procedure
All procedures were performed by one of six experienced endoscopists using Olympus 260 duodenoscopes (Olympus Medical, Tokyo, Japan). The majority were performed under endoscopist-administered sedation (fentanyl and midazolam) though general anaesthesia with endotracheal intubation was used in some. All patients received a single dose of intravenous gentamicin 2 mg/kg or co-amoxiclav 1.2 g as antibiotic prophylaxis, as per British Society of Gastroenterology guidelines.8 Uncovered self-expanding metal mesh stents (Niti-S, TaeWoong) were deployed across the stricture and if necessary co-axial stents placed so as to overlap the ampulla. Bilateral stents were placed side by side.
The stenting strategy (unilateral vs bilateral; intended target ducts) was determined preprocedure following a HPB MDT consensus. Factors taken into consideration for unilateral vs bilateral and preferred side were the location of disease, presence of lobar atrophy, metastatic burden, portal vein thrombosis and separation of the intrahepatic ducts from tumour.
Definitions
Technical success was defined as successful stent insertion into the predefined intended duct(s). Unilateral stenting was defined as placement of stents into one main duct and bilateral stenting was defined as placement of stents into two main ducts (including combinations of left main, right main, or either right anterior and/or right posterior ducts). Clinical success was defined as reduction of serum bilirubin to ≤50% of preprocedural value within 30 days of ERCP. Cholangitis was defined in accordance with the Tokyo 2018 definitions for acute cholangitis.9 Adverse events were defined in accordance with the American Society of Gastrointestinal Endoscopy lexicon.10
Systematic review
We searched the PubMed database to identify studies which specifically reported 30-day mortality rates following endoscopic drainage in patients with inoperable and/or advanced MHBO. The search terms used were ‘endoscopic biliary drainage’, ‘ERCP’, ‘hilar obstruction’, ‘hilar strictures’ and ‘inoperable’. Titles were screened for relevance and subsequent full text was reviewed for specific reporting of 30-day mortality. References from accepted papers were screened for further relevant articles. The search flow diagram is illustrated in figure 1.
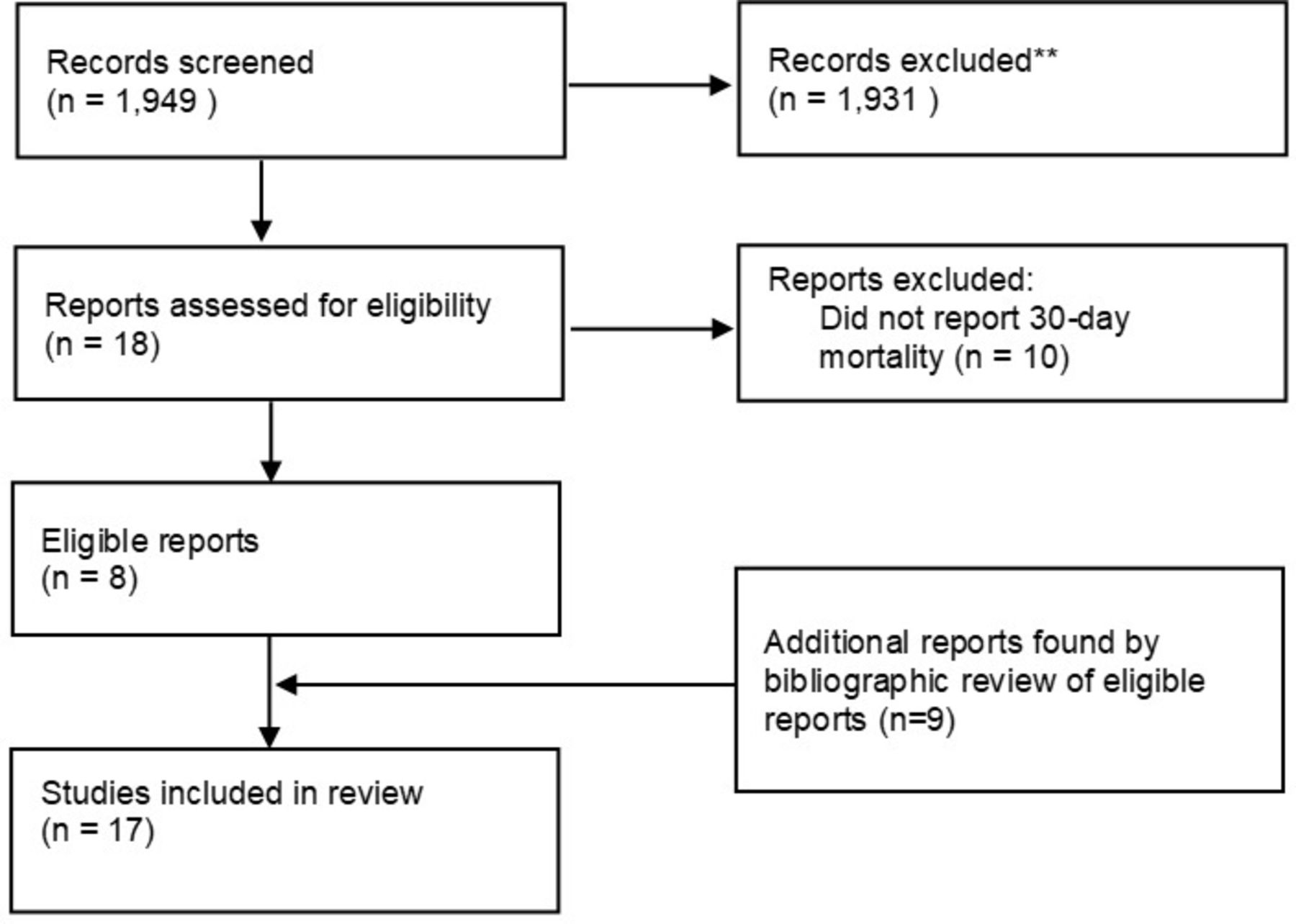
Flow chart depicting selection of articles for systematic review. ** Non-relevant articles.
Statistical analysis
Parametric continuous variables are presented as mean values (SD) and non-parametric as median values (IQR). Categorical variables are presented as values (percentages). Comparison between categorical variables was performed with χ2 or Fisher’s exact test. The cut-off value for CCI in predicting 30-day mortality was evaluated using receiver operating characteristic (ROC) analysis by determining values of sensitivity and specificity to derive the Youden index, by measuring CCI as a continuous variable against 30-day mortality as a dichotomous variable. Univariate analysis was performed to identify predictor variables of 30-day mortality and results demonstrated as OR with 95% CIs. Covariates that displayed a significance level of p<0.05 were used to build a multivariate regression model. CCI and mGPS were used to construct Kaplan-Meier survival plots and comparison of survival distribution between the subgroups was performed with the Mantel-Cox log rank test. Statistical significance was defined as p<0.05. Statistical analyses were performed with IBM SPSS Statistics V.26.0 (IBM).
Results
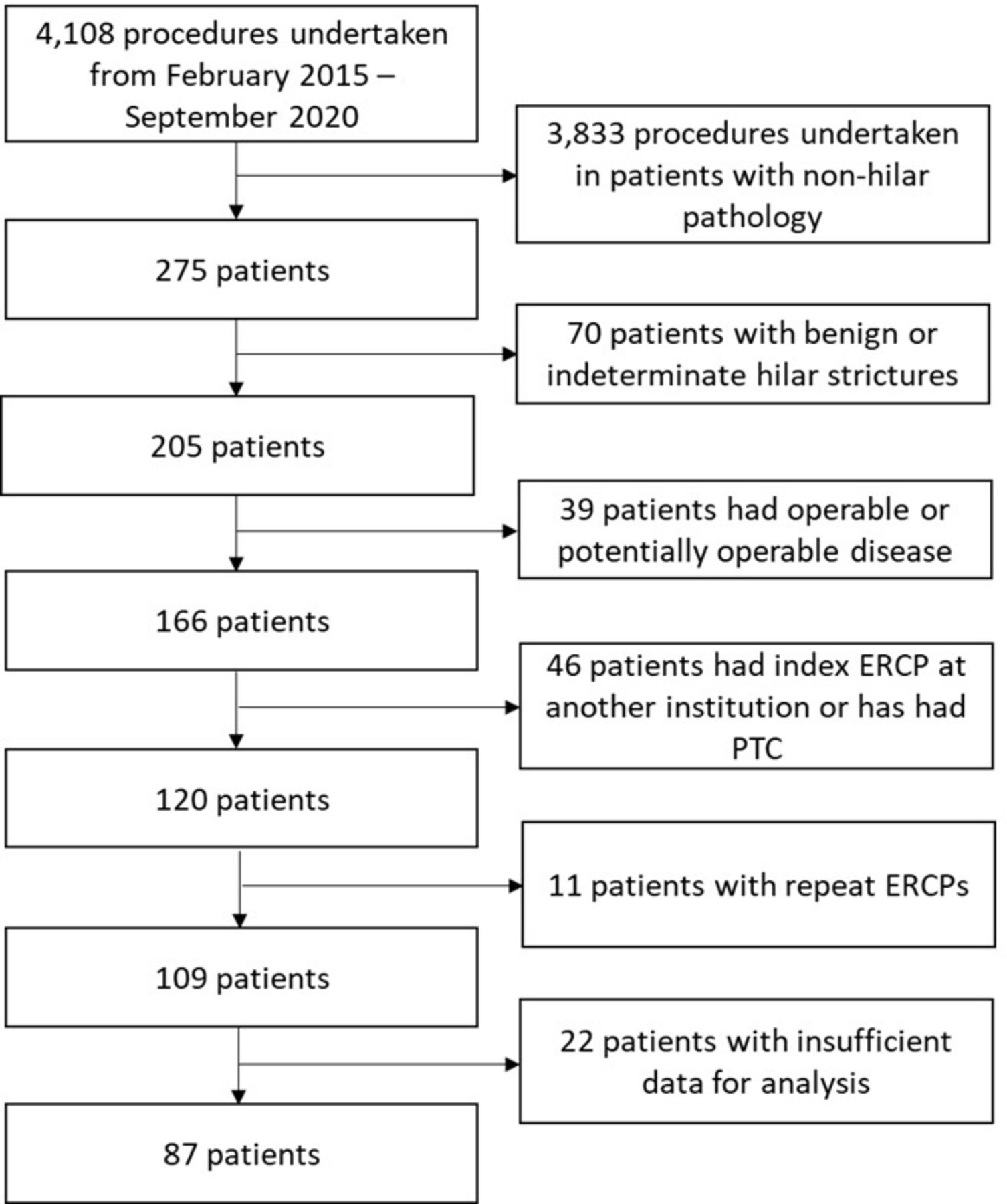
Two hundred and seventy-five procedures were performed for MHBO in the specified time period. Of these, 87 patients were included for analysis. Flow chart depicting patient selection is illustrated in figure 2. The mean age was 70.4 years old (SD ±12.3). Forty-nine (56.3%) of patients were male. CCA was the most common aetiology of MHBO in our cohort, affecting 35 (40.2%) patients.
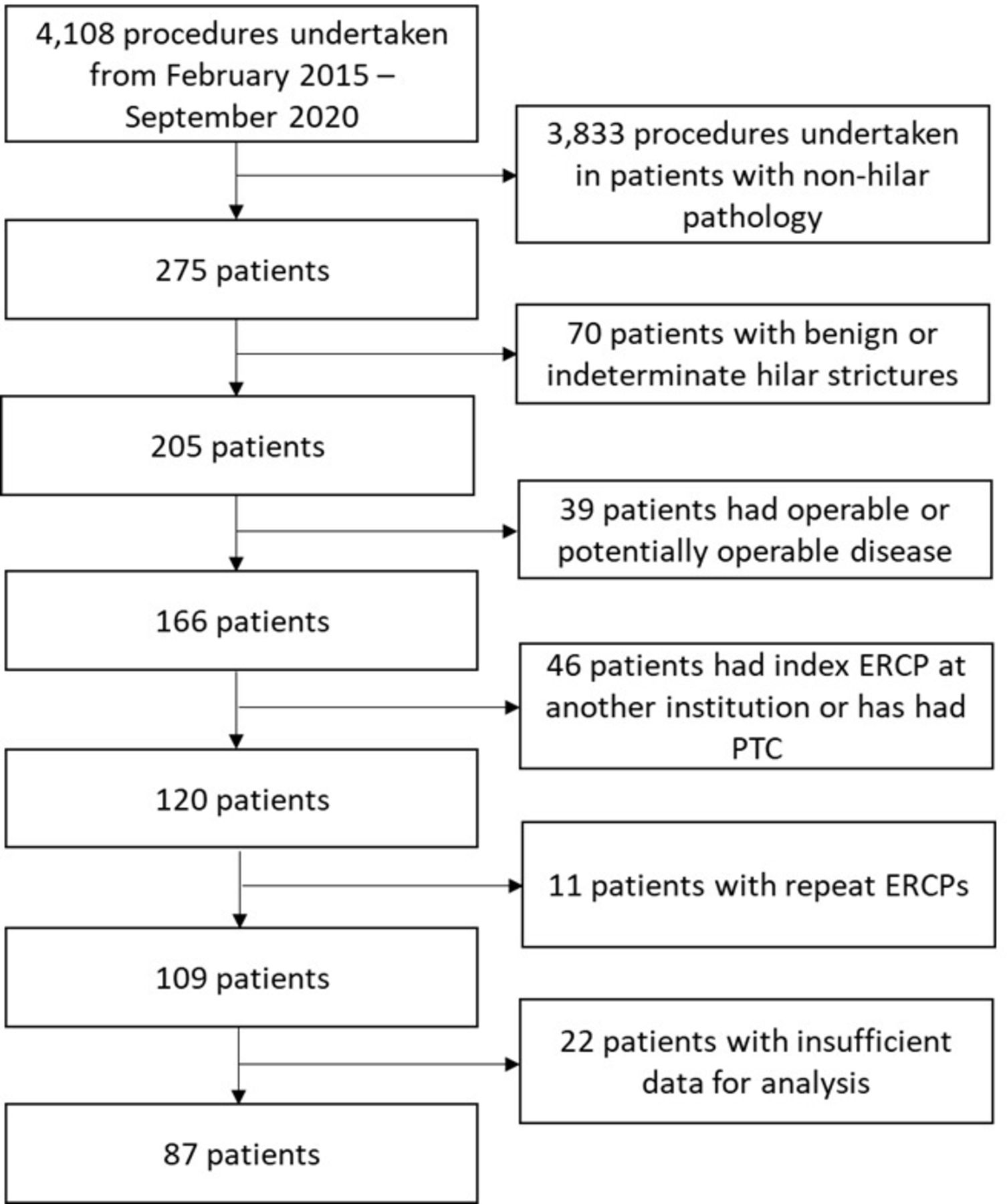
Flow chart depicting selection process for inclusion of patients. ERCP, endoscopic retrograde cholangiopancreatography; PTC, percutaneous transhepatic cholangiogram.
Technical success was achieved in 82.8% (72/87) patients. Of the 72 patients who had technically successful procedures, data on serum bilirubin to determine clinical success was available in 56 patients (11 patients died within 30 days and 5 patients were from external institutions). Clinical success was achieved in 87.5% (49/56) of patients. Baseline demographics and key procedural outcomes are summarised in table 1.
Baseline demographics and key outcomes of the patients
Thirty-day mortality
The overall 30-day mortality rate was 25.3% (n=22) in our cohort. Individual case note analysis revealed the cause of death to be due to progressive malignant disease (n=16), cholangitis (n=3), gastrointestinal bleeding (n=1), sudden cardiac arrest (n=1) and acute pulmonary oedema (n=1).
ROC analysis demonstrated a CCI cut-off value of ≥7, with a Youden index of 0.31, to be a predictor of 30-day mortality (area under curve (AUC): 0.66, 95% CI 0.53 to 0.79, p=0.02).
Baseline patient demographics, characteristics and key outcomes were analysed to evaluate for predictors of 30-day mortality. On univariate analysis, CCI ≥7, serum bilirubin and leucocytosis (white cell count ≥12 × 109 /L) were identified to build a multiple logistic regression model to predict 30-day mortality. On multivariate analysis, only leucocytosis was a predictor of 30-day mortality. Table 2 summarises the variables analysed.
Univariate and multivariate analysis of variables predicting 30-day mortality
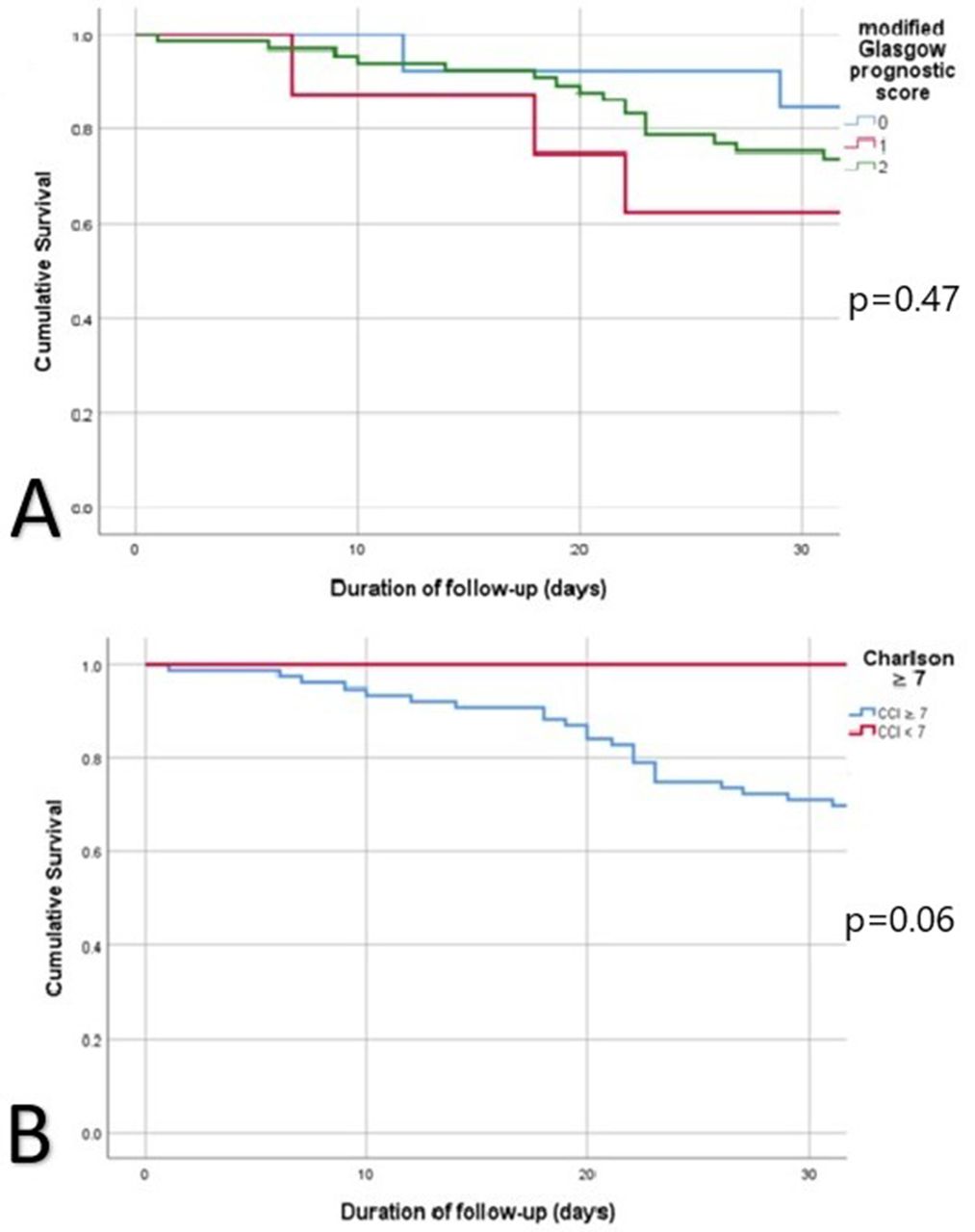
The 30-day mortality rate when categorised by mGPS was 15.4% (2/13) in mGPS 0, 37.5% (3/8) in mGPS 1% and 25.6% (17/66) in mGPS 2, which did not differ between the groups (χ2=1.52, p=0.47). The 30-day mortality rate was 0% in patients with CCI <7 and 28.6% (22/77) in patients with CCI ≥7 (χ2=3.38, p=0.06). Figure 3 illustrates the Kaplan-Meier plots for the above analyses.
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier plots demonstrating survival. (A) 30-day survival in relation to mGPS. (B) 30-day survival in relation to CCI. CCI, Charlson Comorbidity Index; mGPS, modified Glasgow Prognostic Score.
Literature review
Seventeen studies, with a total of 1265 patients, were identified (online supplemental table 1).11–27 There was marked heterogeneity of the included studies with regards to the study design, methodology and tumour type of the enrolled patients, although CCA was the predominant aetiology of MHBO. None of the studies was primarily designed to evaluate predictive factors of 30-day mortality. The reported 30-day mortality rates ranged from 0% to 42%. Five studies reported causative factors of 30-day mortality. In the study by Deviere et al, 30-day mortality was higher in patients with Bismuth II/III MHBO who underwent unilateral stenting compared with bilateral stenting.11 Chang et al demonstrated that patients who had contrast opacification of an undrained liver lobe had increased rates of cholangitis and the 30-day mortality rate was also higher in these patients.12 Three other studies reported post-procedural cholangitis to be associated with increased 30-day mortality.13–15
Supplemental material
Discussion
In our study of a single cohort of patients with inoperable MHBO managed in one referral centre, we demonstrated the overall 30-day mortality rate to be 25.3% following ERCP. Both CCI (with a cut-off value of ≥7) and mGPS were not predictors of 30-day mortality. The derived values for AUC and Youden index for the CCI threshold in our cohort were suboptimal and reflect its limited utility in these circumstances. Multivariate analysis revealed leucocytosis (white cell count ≥12 × 109 /L) to be the only independent predictor of 30-day mortality. Conversely, a raised serum C reactive protein (CRP) (≥10 mg/L) was not predictive. It could be expected that the combination of preprocedural leucocytosis and elevated CRP are observed in a proinflammatory state, either due to the underlying malignancy or cholangitis. Accurate assessment of the presence of preprocedure cholangitis in our cohort is precluded by the retrospective nature of our study as well as the unavailability of local records for patients transferred to our institution for ERCP. The observed discrepancy between leucocytosis and CRP suggests that the systemic inflammation per se may not be associated with 30-day mortality in MHBO. This may also explain why the use of mGPS, a systemic inflammation based score, does not appear to correlate with 30-day mortality in our cohort although this result should be interpreted with caution due to the relatively small number of patients. Leucocytosis in solid tumours is a recognised paraneoplastic phenomenon associated with a poor prognosis and in the absence of systemic inflammation, reflects an intricate paradigm between tumourous secretion of granulocyte colony stimulating factors and altered haematopoiesis.28 29 It is plausible that leucocytosis is a harbinger of tumour progression, given that it accounted for 72.7% (16/22) of 30-day mortality in our cohort.
In our systematic review, four studies reported post-procedural cholangitis as a major factor in 30-day mortality.12–15 Strategies to reduce early mortality after ERCP for MHBO may therefore hinge on effective biliary drainage and reducing the incidence of post-procedural cholangitis. These strategies should be individualised in accordance with the patient’s disease burden. The effectiveness of drainage correlates with the volume of liver drained; Takahashi et al demonstrated that draining ≥33% of liver volume in patients with preserved liver function and ≥50% of liver volume in patients with impaired liver function to suffice.30 The presence of portal vein thrombosis, with resultant atrophy of the corroborative liver segment, is unlikely to lead to effective biliary drainage if stented and is associated with an increased risk of cholangitis.31
Although the literature body is abundant with studies evaluating technical aspects of ERCP in MHBO, there is a paucity of studies focusing on primary evaluation of short to medium term outcomes. Patient-reported outcome measures (PROMs) in this cohort of patients are essential to evaluate the benefit of ERCP in these settings. The studies identified in our systematic review did not address QOL or qualitative assessment of symptom relief. The retrospective nature of our study precluded accurate measurements of such metrics. In a palliative setting, an invasive intervention that is technically successful but which does not permit survival beyond 30 days may be considered futile unless it improves QOL in the short term. Prospective studies to evaluate the impact of ERCP as a palliative procedure on PROMs and QOL in patients with MHBO are warranted.
Recent nationwide analyses from the UK demonstrated the 30-day mortality in patients with MBO to be 19.1% following ERCP4 and 23.1% following PTC.5 Both studies found that 30-day mortality was higher in patients with intrahepatic biliary tract cancers and non-pancreatic cancers. In an English nationwide registry analysis following ERCPs in 40 938 patients, Bodger et al demonstrated a 30-day all cause mortality of 5.3% in all patients; 2.4% in non-malignant cases with underlying malignancy being a predictor of mortality (OR 8.6).32 In addition, the last-coded primary diagnosis was underlying malignancy (HPB and others) in 57.1% of deaths. The reasons for this observation are likely to be multifactorial. These patients often have impaired physiological reserve due to the underlying malignant disease burden, as well as the impact of biliary obstruction and cholestasis on malnourishment, cholangitis, coagulopathy, renal impairment and immune dysregulation. Furthermore, patients with MHBO are more likely to have complex, multi-focal stricturing compared with patients with malignant distal biliary obstruction. Therefore, biliary intervention in patients with MHBO tends to be more challenging and requires appropriate preprocedure planning. Therefore, appropriate patient selection for intervention should combine the evaluation of objective markers with an overall clinical judgement of the patient’s frailty and trajectory of decline. Utilisation of a standardised outcome measure, such as 30-day all cause mortality, in these patients should be encouraged.
Our study has some limitations. First, this was a retrospective study from a single institution and is subject to the pitfalls of a retrospective analysis. Second, the relatively small number of patients in our cohort may have been insufficient to be definitive of predictive variables on multivariate analysis. Third, patients with inoperable or palliative MHBO who did not undergo ERCP were not included. This precluded direct comparison of outcomes, including those pertinent to palliative care such as QOL and place of death. Fourth, as a tertiary institution, patients are often repatriated back to their local hospitals, therefore, not all postprocedural adverse events may have been captured, though our electronic database captures mortality in all patients. Patients with inadequate data were excluded from analysis in an attempt to mitigate information bias. The inclusion of all aetiologies of MHBO meant that our cohort was a heterogeneous group of patients with differing tumour characteristics which may have had an impact on mortality rates. However, this was a large consecutive cohort of patients managed in a systematic way by an experienced team of endoscopists and we believe contribute to the literature and understanding of the optimum management for these patients.
In conclusion, in our cohort of patients with inoperable and/or palliative MHBO, the 30-day mortality rate following ERCP was 25.3%. On multivariate analysis, only leucocytosis was a predictor of 30-day mortality. The majority of deaths were due to progression of underlying malignant disease. Our data are consistent with UK-wide and international published results and demonstrate that ERCP drainage of MHBO is appropriate for carefully selected patients, but is technically demanding with high morbidity and mortality so should be only performed by experienced practitioners with careful pre-procedure planning. Larger scale studies are required to further identify predictive alternative variables of 30-day mortality in addition to leucocytosis which may assist in selection of patients who are most likely to benefit from palliative intervention.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SME proposed conception of the manuscript. WO and MAS collected and analysed the data. WO performed the systematic review and analysis of the studies. WO wrote the initial draft of the manuscript. MAS, VSH, MTH, BP and SME critically revised the manuscript. All authors approved of the final version of the manuscript. SME is the overall guarantor for the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.