Article Text

Abstract
Objective Inflammatory bowel disease clinical nurse specialists (IBD-CNSs) face increasing pressures due to rising clinical and patient demands, advanced complexity of work role, and minimal specialist management training and support. Stress and burn-out could undermine the stability of this workforce, disrupting clinical provision. We reviewed the literature on stress and burn-out to demonstrate the lack of evidence pertinent to IBD-CNSs and make the case for further research.
Design Following Levac et al’s scoping review framework, relevant databases were searched for publications reporting work-related stress and burn-out among specialist nurses. Following screening and consensus on selection of the final articles for review, all authors contributed to data charting. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses Scoping Review extension guided reporting of the review.
Results Of 194 retrieved articles, eight were eligible for review. None focused on IBD-CNSs, were qualitative, or UK-based. Three core themes were identified: Rates of Burn-out, Mitigating and Alleviating Factors, and Preventing and Resolving Burn-out. Risk of burn-out is greatest in novice and mid-career CNSs. Age and duration in role appear protective. Personal achievement is also protective and can mitigate earlier episodes of burn-out; opportunities for career progression are limited. Promoting personal well-being is beneficial. Senior managers have poor understanding of the role and provide inadequate support. Commitment to patients remains high.
Conclusion Burn-out arises in CNSs across clinical specialisms in the international literature and has a significant negative effect on the workforce. Further research is needed to address the dearth of evidence on burn-out in IBD-CNSs in the UK.
- crohn's colitis
- crohn's disease
- inflammatory bowel disease
- ulcerative colitis
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
There is a worrying level of burn-out amongst clinical nurse specialists (CNSs).
Subjective data from one professional support group in the UK indicate the presence of burn-out in inflammatory bowel disease (IBD) CNSs.
The components of burn-out (emotional exhaustion, depersonalisation and lack of personal achievement) affect different cohorts (age, workplace environment, time in role) differently.
Current evidence comes from international studies where the structure and management of healthcare services and the remit of the CNS differ to those of the UK’s National Health Service.
There is no global or UK data specifically addressing burn-out in IBD CNS.
There is no qualitative evidence to explain relationships between different components of burn-out and personal characteristics such as age, and time in role.
Further research is needed to understand the experiences of burn-out within the IBD CNS workforce, and to determine the most effective strategies for addressing burn-out in this cohort.
Failure to address burn-out in IBD CNSs risks disruption to the clinical workforce, and thus the quality of service provided to patients due to attrition.
Junior IBD-CNSs need mentoring and support but risk losing this if senior colleagues leave the service.
Introduction
People living with inflammatory bowel disease (IBD) in the UK are supported by the knowledge, experience, and availability of IBD clinical nurse specialists (IBD-CNSs) who provide a range of advisory, therapeutic, advanced clinical services and emotional support to patients in many (often complex) situations. These IBD-CNSs have advanced or specialist expertise in caring for people with IBD and, as a core part of a multidisciplinary team (MDT), lead and manage a caseload of patients, providing diagnoses, care planning, treatment and follow-up and continuity of care. In the UK, IBD-CNSs may also deliver a broad range of additional clinical activities, including infusion clinics, endoscopy clinics, and email and telephone advice services. Yet as IBD interventions advance, and the patient population increases in size, the workload for IBD-CNSs increases. This workload can feel relentless and demanding, and the personal impact of responding to and working with patients with whom nurses have a long-term professional relationship, can be intense. Patients routinely report the IBD-CNS as their preferred point of contact when they need urgent clinical support or ongoing advice,1 2 bringing an expectation from patients of rapid response to queries, and resolution of problems. Many IBD-CNSs enter this specialist post soon after qualifying rather than after several years of gathering experience in clinical practice, and the increasing demands the specialist role places on them can quickly lead to work-related distress, burn-out and attrition.3 This complex and demanding caseload is unsustainable, both for service provision and for nurses themselves.4 As with other clinical specialisms,5 the Royal College of Nursing (RCN) IBD Nurse Network provides an important national network through which IBD-CNSs can seek clinical advice and pastoral support from each other; posts onto the Network’s Facebook page evidence the stress that many specialist nurses are and have been under since before the COVID-19 pandemic. Stress, and burn-out (characterised by high levels of emotional exhaustion (EE) and depersonalisation (DP) and low levels of personal accomplishment)6 are similarly reported in other advanced roles, including renal and oncology nurse specialists.7–9 The objectives of this scoping review were to identify the current evidence reporting experiences of stress and burn-out in specialist nurses, and to demonstrate the case for undertaking further qualitative investigation of this topic in IBD-CNSs.
Materials and methods
Scoping reviews are appropriate when the aim is to identify and analyse knowledge gaps.10 The approach facilitates a broad sweep of available evidence and is useful for informing focus and methodology of follow-up studies. As with a classic systematic review, the methodology is rigorous with transparent processes that enable the reader to assess the quality of what has been done.
We, therefore, conducted a scoping review of the relevant literature guided by the six-step framework recommended by Levac et al,11 (table 1), which extends the original work of Arksey and O’Malley.12
The six stage scoping review methodology of Levac et al11
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) extension for scoping reviews guided the reporting of the work.13 The scoping review approach enables the merging and presentation of data from studies of different design and from a range of sources via a narrative synthesis, to represent the meaning of the body of work reported in the selected papers.14
Stage 1: identifying the research (review) question
Levac et al recommend considering the target population (CNSs), the outcomes of interest (stress and burn-out) and the concept (experiences of burn-out) when developing the review question.11 We used the SPIDER (Sample size; Phenomenon of Interest; Study Design; Evaluation; Research type) tool to develop a broad search question incorporating these aspects.15 A preliminary sweep of the literature had indicated there may be very little evidence specific to IBD-CNSs, so our scoping review question was: What evidence exists on the personal experiences of work-related stress and burn-out among CNSs?
Stage 2: identifying relevant studies
Search strategy
The process of identifying studies is iterative, requiring repeated visits to the literature to gradually refine the search strategy.11 Early searches produced very few ‘hits’, which seemed unlikely, so the strategy was gradually refined until the most effective approach across all databases was confirmed. This flexibility is acceptable in a scoping review where the aim is to get a sense if what data exists on a topic, rather than produce a definitive answer to a specific question.10 To allow for the wide variation in job titles associated with these specialist roles, the final search terms were: (“Specialist nurse” OR “nurse specialist” OR “advanced nurse practitioner” OR “Advanced practice nurse” OR “ Consultant nurse” OR “clinical nurse specialist”) AND ((“work-related” OR “work related” OR job OR role) AND (wellbeing OR well-being OR “well being” OR stress OR burnout OR burn-out OR “burn out”)). The definitive searches were conducted in July 2020 in CINAHL Plus with full text, Google Scholar, Internurse, Medline, Pubmed, Science Direct, Scopus, and Web of Science. Reference lists of identified papers were also hand-searched. Throughout this paper, the term CNS is used to refer to nurses in any advanced, consultant or specialist clinical role. As recommended in the PRISMA-SCR checklist, the search strategy for one database is provided in online supplemental additional file .
Supplemental material
Search inclusion and exclusion criteria
We used the following broad inclusion and exclusion criteria to capture as many articles as possible:
Inclusion criteria
Original, full text, peer reviewed research.
Published in English, since first January 2000.
Qualitative, quantitative or mixed-methods design.
Key search terms in title and/or abstract.
Focuses on experiences/measurements of stress, burn-out and/or well-being.
Exclusion criteria for the search
All other forms of publication (abstracts only, conference proceedings, editorials, literature reviews, opinion pieces).
Stage 3: study selection
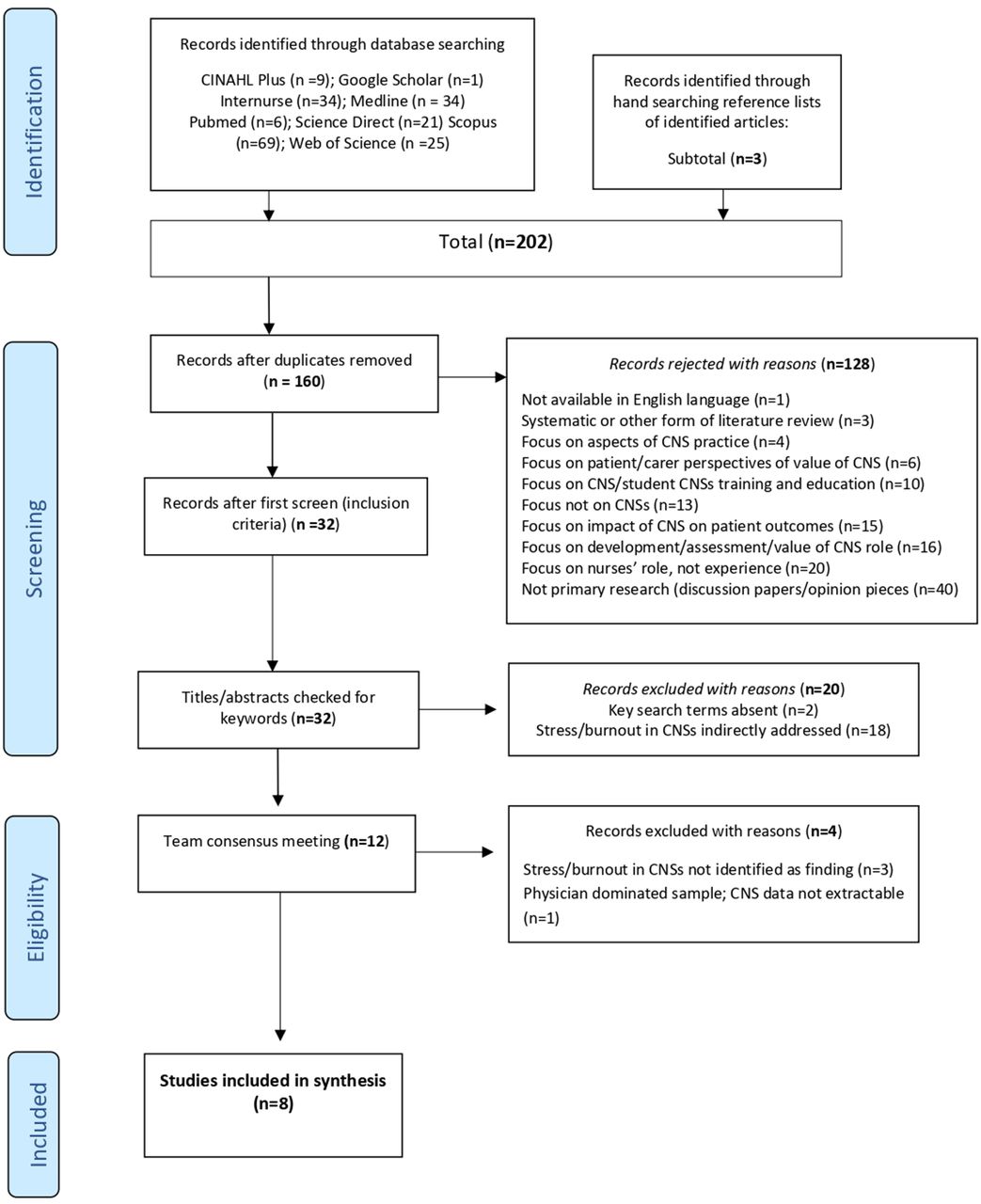
Duplicates were removed, and all studies were screened by the first and the senior author against the inclusion criteria. Studies were further excluded if: (1) the search term ‘Clinical nurse specialist’ or any of the equivalent role descriptors (detailed in stage 2: Identifying Relevant Studies, above) not appear in the title, and (2) if the term ‘burn-out’, ‘burn-out’ or ‘burn out’ was absent from title or abstract, or (3) was only included as a recommendation/conclusion of the study. The remaining articles were then reviewed by the team, before meeting to agree by consensus the final articles for the review. The process of study selection is demonstrated in the PRISMA diagram16 in figure 1.

{kind=link}
PRISMA Flow diagram detailing study selection.16 CNSs, clinical nurse specialists; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Stage 4: charting the data
Study design and participant demographic data were extracted by the senior author (LD) onto a prepared data chart, before circulating this to the team who extracted data relevant to the variables of interest and the scoping review question (table 2).
Variables of interest extracted from each included study, with rationale
Three authors (JD, IM and LY) extracted data from two of the eight selected papers, while KK and LD extracted data from four, and all eight papers, respectively. Each selected article was thus charted at least twice. Extracted data were combined on a single data chart, and early themes were identified by LD. Initial or preliminary codes were allocated, guided by the stated aims of the scoping review. Following team discussion of these codes, main themes and subthemes were developed, and agreed. Data charting identified similarities and some outlying concepts across the eight included papers, leading to a detailed insight into the prevalence, development and impact of stress and burn-out in CNSs. Extracted data and summary of included papers is provided in table 3.
Summary of included studies
Stage 5: collating, summarising and reporting the results
The three distinct steps in stage 5 of Levac et al’s framework,11 reflect the standard reporting sequence of Results, Discussion, and Conclusions and Recommendations.
Results
Study characteristics
Of the eight included studies, there were five from the USA,17–21 one from Canada/USA,22 one from Spain,8 and one from Australasia.7 All were quantitative, with seven cross-sectional surveys,7 17–22 of which four7 19–21 were online; the remaining study was a meta-analysis of existing data.8 Of the seven studies that recruited participants, five described purposive sampling, but did not overtly state that as the method7 18–20 22; one used purposive and snowball sampling,21 and two used convenience sampling.8 17 These sampling methods are acceptable in quantitative studies when a particular population is being investigated. All studies used statistical methods for data analysis and reported findings using data charts or diagrams and explanatory text.
In total, there were 12 828 CNS participants (range 8–9959) of which 11 850 (92.3%) were female; where reported, ages ranged from 20 to 65+ years17–20 22 or were given as a mean of 38.2 years.8 Time as a nurse was reported by two studies, ranging from <5 to 20 years+,14 or as a mean of 8.78 years.8 Four studies reported time in the specialist role as either a range (<6 months to 20 years+)7 19 21 or a mean of 6.4 years10; two reported marital status.8 20 To measure or rate burn-out, five studies7 8 18–20 used the Maslach burn-out Inventory (MBI),6 one study22 used a single item from the Mini-Z survey,23 and one study21 used the Copenhagen burn-out Inventory.24 The remaining study17 used the Professional Quality of Life Scale to assess compassion fatigue (CF) and compassion satisfaction (CS) as predictors of burn-out.25
Three themes were established: Rates of burn-out, Mitigating and Alleviating Factors, and Preventing and Resolving burn-out.
Rates of burn-out
A total of 30%–35% of oncology CNSs report high levels of EE and DP and low levels of personal achievement (PA)8; similarly, haemodialysis CNSs report scores of ≥28 for EE (low ≤16, average 17–27, high ≥28); ≥10 for DP (low ≤5, average 6–9, high ≥10); and ≥40 for PA (low ≥40, average 39–34, high ≤33).7 Among haematopoietic cell transplantation CNSs, scores for EE and PA are similarly high, but lower (mean 4.8) for DP, although an average burn-out rate of 45% is reported.20 A burn-out rate of 20.9% is reported among CNSs using electronic health records (EHRs),22 and there was a mean composite score of 2.56 (range 0–6) for the MBI in a large group of mixed specialty CNSs, although composite score reporting is not recommended.26 In a cohort of 433 mixed specialty CNSs, burn-out was reported as occurring currently (26.3%), formerly (33.2%) or never (40.4%).18 In contrast to all this evidence, one very small study (n=7) reported a mean composite score of 43.05% of participants experiencing high levels of burn-out and deduced that there was no evidence of burn-out in CNSs,21 but the sample size is too small for results to be reliable. Finally, an exploration of CF and CS, both known precursors to burn-out, reported low levels of CF and high levels of CS in the sample (n=208), deducing low levels of burn-out across the cohort.17
Mitigating and alleviating factors
Demographic influences
Burn-out was less prevalent among older nurses7 17–20 and those with more experience/years in the role. Older participants had better CS scores (aged 50–60, 60.4%; aged >60, 58.3%); high levels of CS were also found in those with 5–10 years in practice (58.8%), with the highest CS scores reported by those with >20 years in practice (80%).17 In another study, older nurses and those with more time in the role (16–20 years) had higher job satisfaction scores, decreased stress and lower levels of burn-out, while all age groups below 60 years+had lower job satisfaction scores, and nurses in mid-life (31–40 years old) had higher DP scores than older nurses (51–60 years old).7 A third study found that while 41% of participants had never experienced burn-out, the highest rates of burn-out were reported in the 24–34 years (former burn-out 32.6%; current burn-out 30.7%), and 35–44 years (former 41.0%; current 29.8%) age groups. In contrast, those aged >55 years, reported low burn-out rates (former 4.9%; current 11.4%).18 This pattern continues across two other studies, where older professionals were found to experience higher levels of engagement with work (correlation coefficient (r)=0.11; probability (p)<0.05), while younger professionals experienced higher levels of job stress (r=−0.10; p<0.05),19 and nurses aged 40 years and older (40–49, 50–59, 60+) had lower DP scores than younger nurses (aged 20–29).20 Counter to this evidence, one very small study (n=7) reported that CNSs do not experience significant burn-out or endure risk factors predisposing them to burn-out, and states that burn-out appears more likely in more experienced nurses.21
Organisational influences
Working environment was found to influence burn-out. Oncology nurses based in hospital treatment centres had higher rates of burn-out than nurses working in palliative care or community settings.8 Among haemodialysis nurses, those working in tertiary (hospital-base) centres had lower satisfaction scores, higher stress levels and higher burn-out scores (mean (M)=30.71, SD=12.13) particularly when compared with nurses working in patients’ homes who had high satisfaction scores, low stress levels, and low burn-out scores (M=28.29, SD=10.46) although these differences did not reach statistical significance.7 In contrast, greater satisfaction with the working environment correlates with greater job satisfaction (r=0.70, p=<0.01), lower job stress (r=−0.41, p=0.01) and lower EE (r=−0.49, p<0.01).7 Working in an outpatients’ setting and completing longer hours including extra work at home predicts burn-out among haematopoietic cell transplantation specialist nurses.20 Similarly, the likelihood of burn-out increases among advanced practice/specialist nurses working with EHRs in an outpatients setting (adjusted OR: 1.30 (95% CI 0.53 to 3.24); p=0.567) who have to catch up with EHR-related administration at home (adjusted OR: 2.66 (95% CI 0.91 to 7.80); p=0.075) due to having insufficient time for documentation during the working day, which predicts a three times higher likelihood of burn-out (Adjusted OR: 3.72 (95% CI 1.78 to 7.80); p=0.001).22 Workload was identified as influential across three other studies7 18 20 where the EE component of burn-out was positively correlated with workload (r=0.44),7 the high demand for direct patient care and related administrative tasks left little time for personal and professional development activities and contributed to increased burn-out,20 and where specialist nurses felt they had no control over their workload.18 Low levels of personal accomplishment, either due to failure to ‘save’ the patient8 or having fewer opportunities for personal development/career advancement,18 and lack of career satisfaction20 lead to lower PA scores and increase burn-out risk. Nurses with high personal accomplishment scores were less likely to currently be experiencing burn-out, than to never or previously have experienced it (14.5% vs 53.4%, 32.1% respectively, p=<0.001), suggesting that PAs can overcome previous episodes of burn-out.18 Additional work-related factors that contribute to burn-out included feeling undervalued or unrecognised for one’s work,7 18 poor work–life balance,18 20 22 conflict with physicians,7 lack of autonomy and role ambiguity,19 and managers having a poor understanding of the day-to-day role of the CNS.18 Increased autonomy increases job satisfaction, thus protecting against burn-out.7 In contrast, three studies found that good managerial and peer support mitigated against the factors that lead to burn-out.7 17 18 There was a significant positive relationship between increased levels of CS and increased perceptions of report received from managers (p=0.025, Cramér V=0.231), coworkers (p≤0.001, Cramér V=0.347) and family and friends (p≤0.001, Cramér V=0.385), which was then related to lower levels of burn-out.17
Nurses were most satisfied when managerial support was perceived as fair and equitable (including fairness in rostering) and supported their clinical practice.7 Being able to attend to their own self-care needs, being appreciated, receiving good leadership/management support, and experiencing organisational promotion of health and well-being were identified as strategies for mitigating against burn-out,18 alongside opportunities for career advancement.18 19
Job stress19 and moral distress20 are also influential. Job stress is positively related to burn-out (p<0.01), and both stress and burn-out are negatively related to work engagement (both p≤0.01); moral distress (arising from the inability due to external influences to deliver care to a preferred standard) was reported as medium (44–62) or high (>63) in 31% and 37% of specialist nurses respectively.20 burn-out (specifically the component of EE) negatively correlates with getting things done (r=−0.48, p=<0.01), task requirements (r=−0.46, p≤0.01) and feeling valued (r=−0.46, p≤0.01).7
The relationship between specialist nurses and patients appears influential. Lower levels of DP (manifesting as an affective-symptomatic lack of empathy)27 among CNSs are reported in one study with oncology nurses,8 with others observing that dedication to patients and absorption in the specialist role reduces burn-out19 and that despite personal and work-related challenges, commitment to patients remains high.18 21
Internal influences
While working practices, the work environment and the quality of managerial/leadership support were shown to affect burn-out, nurses’ internal influences often mitigated against it. Robust social support from family and friends appears important,19 more so than relationships with co-workers,17 and better work–life balance facilitates lower job stress levels.19 In one study, 75% of specialist nurses who reported that they had never experienced burn-out, had high PA scores, strong family support, close friendships, and engaged in group activities outside the workplace.18 In contrast, 57% (n=65.5) of 115 Advanced Practice Providers reporting burn-out either disagreed or strongly disagreed with the statement ‘my work schedule leaves me enough time for personal/family life’, indicating a poor work≤life balance.20 Self-care practices—including healthy eating, exercise, mindfulness practices, taking time off/holidays and seeking therapy were protective.17 18 20
Preventing and resolving burn-out
Four of the eight studies make recommendations for addressing burn-out based on their findings7 17–19 while one reinforces strategies recommended in previous literature.20 There was a statistically significant positive relationship between mindfulness practices and the level of CS with a moderate to large effect size (p=0.016, Cramér V=0.242), and between meditative practices and burn-out (p=0.42, Cramér V=0.219).17 As described above, the presence and quality of support from coworkers, managers and administrators affects the level of burn-out among CNSs,17 and support, workload management and reducing peer to peer conflict are recommended to reduce burn-out and increase retention among CNSs.7 In another study, ‘self-care’, ‘career development’, ‘leadership support’ and ‘creating community’ (work-based teambuilding) are recommended areas for attention,18 while the final study recommends resolving work–family conflict (restoring work–life balance and giving greater support (mentorship) to young professionals transitioning into the CNS role’.19 Drawing on recommendations from previous studies, the strategies of counselling, mindfulness, stress-reduction, confidence-building, exercise, team building and adjustments to rostering are advised.20
Discussion
Burn-out arises across numerous nurse specialist and advanced practice roles and affects clinicians differently throughout their career—findings that are highly relevant to the UK IBD-CNS workforce. Evidence indicates that CNSs who are new in post and those who are mid-career experience burn-out more than those who have many more years of experience and thus are also older. There are numerous possible explanations: younger nurses moving into the specialist role soon after qualification without an arsenal of advanced skills gained in a ward-based role; mid-career nurses moving into lead or consultant nurse roles without the necessary staff management and senior level operational skills; and nurses with many more years in the role having gained skills and competence through the natural novice-expert progression that is typical across nursing.28 The need for better preparedness for the role is indicated in this review and evidenced in the literature.29–31
Much of the evidence points to the importance of work–life balance, family time and support and self-care, and it is possible that the predominantly female nursing workforce experiences a great amount of stress from trying to balance home and family life, with the demands of their role. Where early and mid-career IBD-CNSs may also be raising children and managing their family, this may compound the stress factors that lead to burn-out. If the desire for personal advancement to progress their career (from study days, conferences and required training, through to clinically based Masters and doctoral studies) also arises during this time period the demands may be compounded, increasing the risk of low personal accomplishment as a precursor to burn-out. Older nurses not only benefit from the years of experience they have in the role, but may have fewer direct family responsibilities due, for example, to children growing up and achieving independence. This changing responsibility within the family home may bring more freedom to pursue personal development/achievement goals, thus reducing burn-out.
The importance of and desire for ongoing education and training to support the CNS role is well-recognised.9 32 33 As evidenced in this review, opportunities for personal development can mitigate against earlier episodes of burn-out, which suggests that providing personal development as an intervention for burn-out, may be beneficial. One report focusses specifically on the limited options for professional development among the older experienced specialist workforce but does not acknowledge this representation of low PA as a precursor to burn-out.9
The use of EHRs and working in outpatient settings are identified in this review as contributing to burn-out. Since the majority of IBD-CNS workload is clinic/outpatient based, with regular use of remote methods of access such as telephone clinic and advice lines,2 these factors may be highly significant to this and other CNS cohorts. Recent changes to the delivery of clinical services—particularly routine follow-up—due to the COVID-19 pandemic indicate that e-health is likely to have a bigger profile in the working practices of many clinicians,34 including IBD CNSs35; thus while addressing one problem, increased use of EHRs may compound another.
This review also highlights that poor acknowledgement by senior managers of the CNS role and unsustainable workload also fuel burn-out. Health service personnel outside the immediate MDT in which the specialist nurse sits, have a poor understanding of the complexity and range of the CNS role36 37 despite growing evidence on the clinical value of CNSs and the positive impact on patient care.38–42 Workload across IBD-CNSs has been shown to exceed recommended guidelines, with 63% of participants in one study reporting a caseload above the recommended level, and 84% doing unpaid overtime to manage this3; the consequence is that the opportunities for PA may diminish. As evidenced above, these factors contribute to burn-out, likely due to moral distress and EE. Addressing these issues is critical, as evidence indicates that job autonomy, role clarity, and job support are associated with a high level of job satisfaction29 which keeps nurses in post. One study from Germany reports that factors that ‘push’ nurses to leave their post and the country to take up clinical appointments elsewhere, include high workload, limited decision-making power, low recognition, lack of collaboration between nurses and physicians, poor working environment, low renumeration and poor advanced training opportunities.43 All of these ‘push’ factors, except low renumeration, are evidenced in this review, suggesting that this European data may be globally applicable.
Many of the difficulties and challenges identified in this scoping review are also relevant to IBD CNSs. There is thought-provoking commentary4 on the likely devastating impact to IBD services if the early indicators of burn-out, particularly among experienced IBD CNSs in senior positions, are not addressed. Burn-out has also been identified in colorectal surgeons, gastroenterologists and surgical and medical gastroenterology nurses, with similar factors (age, gender, years in role, workload and leadership responsibilities) being influential on the extent of burn-out experienced.44–46 While a useful contextual tool, some of the solutions suggested for medical staff and colorectal surgeons (mentoring, dedicated study time, support to follow specific areas of clinical interest)44 45 are unrealistic across a nursing workforce which already has, for example, difficulty simply securing study leave.
Avoiding attrition of these highly-skilled IBD-CNSs may be a considerable challenge in the current climate, when morale within the workforce is very low and the Registered Nurse vacancy rate in the UK’s National Health Service (NHS) is currently at 10.5% (39,813 vacancies) amidst an overall vacancy figure of 100 000.47 This staffing crisis, which existed prior to 2019, is currently escalating due to the significant personal impact of the pandemic on all clinical staff and on NHS services. An RCN press release in July 2020 reported that of their surveyed members, 36% were now thinking of leaving the profession.48 ‘Push factors’ cited include dissatisfaction with the way staff were treated during the pandemic, low staffing levels and lack of management support. These factors reflect the aspects identified in this literature review of feeling undervalued, overworked, and experiencing poor support from senior management, suggesting that a system-wide approach is needed to resolve burn-out throughout the clinical workforce, regardless of specialism.
There are some suggestions from this review of the strategies that nurses can employ personally to help mitigate against the risk of burn-out (physical exercise, social support networks, mindfulness activities, eg) but we do not know how transferable these potential mitigating factors are to the IBD CNS workforce; further, individual efforts are unlikely to overcome the negative systemic influences detailed above.
An IBD-CNS collaborative workshop to acknowledge emotional impact and risk of burn-out identified that these specialist nurses need support addressing the many ways in which they are emotionally affected by their work, with an express request for further training and support, including access to clinical supervision.49 The potential for clinical supervision to counter burn-out in nurses is recognised50 51 and has been demonstrated, in principle, in one small pilot study with IBD-CNSs,52 but more work is needed to strengthen this evidence and to understand the experiences and implications of burn-out among these specialist nurses.
Limitations
Although the CNS role in the UK is among the most established globally, with a wide remit and high level of role autonomy, we could find no published UK data addressing burn-out in this professional group, and none specifically relevant to IBD-CNSs in the UK, or globally. Participant cohorts in the included studies were not described, so it is not known if IBD CNSs/gastrointestinal nurses were included.
Conclusion
There is no evidence of either the prevalence and experience of burn-out in IBD-CNSs in the UK, and no UK or global qualitative data to explain correlations such as age and years in role, or why the mid-career group (aged 31–50 years, 10–20 years in practice) seem the most vulnerable.
Further qualitative work may give insights into the impact of burn-out on nurses’ decisions to remain in or leave the service, the factors which mitigate or exacerbate well-being, and the future security of the IBD CNS workforce in the UK. Such work could also lead to the development of a nationwide survey to measure prevalence of burn-out using the MBI. This evidence would provide a robust rationale for developing interventions to protect and support the well-being of IBD-CNSs.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants. As per the PRSIMA-ScR guidelines, (ref. 13) ethical considerations must be acknowledged. This scoping exercise did not require ethical approval as it reviewed previously collected data. All included studies that did collect data from human participants reported securing ethical approval prior to study commencement.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors devised the search strategy. LD conducted the searches; LD and KK did preliminary screening; all authors agreed by consensus the documents to retain for the review. All authors carried out data extraction, and contributed to devleopment of themes and subthemes. LD drafted the manuscript and all authors reviewed, revised and agreed content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests KK: Janssen, Takeda, Tillotts, Falk, MSD, Abbvie, Shield JD: employed full-time by Takeda UK as clinical nurse educator providing non-promotional education to IBD CNS SM: Takeda, consultancy on education resource development for IBD CNS LY: speaker fees from Ferring, Falk, Galapagos, Janssen, Sandoz, Tillotts and Takeda LD: funding to support research from Takeda, Janssen; speaker fees from Abbvie, Janssen and WedMD.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.