Article Text

Abstract
Introduction Human papillomavirus (HPV) is strongly associated with Barrett’s dysplasia and oesophageal cancer suggesting a role in carcinogenesis. HPV persistence predicts treatment failure after endotherapy for Barrett’s dysplasia. This pilot study applies a novel HPV screening tool (previously only used in the oropharynx) to detect HPV DNA directly and determine the prevalence rates in Barrett’s oesophagus (BO).
Method DNA was extracted from 20 formalin-fixed BO samples. HPV DNA was detected using real-time PCR and gel electrophoresis.
Results 5 out of 20 patients were identified as positive for HPV. Prevalence was 25% in patients with BO.
Conclusion This method can be used in BO’s tissue to determine HPV infection. Adoption of this as a screening test could potentially revolutionise future research in this area. If a clear link between HPV and Barrett’s dysplasia can be confirmed, this qPCR method has the potential to aid in monitoring and/or dysplasia detection by stratifying those most at risk and aid in the development of new therapies.
- Barrett's oesophagus
- oesophageal cancer
- polymerase chain reaction
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known about this subject?
Transcriptionally active human papillomavirus (HPV) has been shown to be strongly associated with Barrett’s dysplasia. HPV persistence predicts treatment failure after endotherapy for Barrett’s dysplasia.
What are the new findings?
This novel HPV screening method successfully determined HPV prevalence rates.
How might it impact on clinical practice in the foreseeable future?
This novel screening tool could be adopted in routine clinical practice, aiding the monitoring and stratification of patients most at risk of treatment failure and in the development of new therapies.
Introduction
Barrett’s oesophagus (BO) occurs when a portion of the normal distal squamous lined epithelium is replaced with a metaplastic columnar epithelium. This is endoscopically visible (≥1 cm) above the gastro-oesophageal junction and confirmed by histological sampling. Risk factors associated with BO include reflux oesophagitis, male gender, older age, increased waist circumference and smoking. The population prevalence is around 1.6%.1 BO is the most important and recognisable known precursor lesion for oesophageal adenocarcinoma (OAC) which is more common in developed countries. The rate of cancer development is 0.33% per year in non-dysplastic BO.2 The progression of Barrett’s intestinal metaplasia to adenocarcinoma is through dysplastic stages. Our understanding of the known and unknown risk factors, in addition to the molecular bases that are involved in this sequence, is incomplete.3 Most cases of BO do not progress beyond non-dysplastic intestinal metaplasia or transient low-grade dysplasia, but for high-grade dysplasia the risk of OAC is 10% per patient-years.4 Survival rates for OAC at 5 years remain poor at around 13%.5
Human papillomavirus (HPV) infections are common and highly infectious, with an estimated 80% of the general population exposed to genital HPV infections in their mid-20s.6 Although the incidence of genital HPV is known, the incidence in the general population has not been determined.
HPV is known to be the main causative agent for cervical cancer. HPV is also strongly implicated in oropharyngeal cancers and is where we have adapted our screening tool from.
Systematic reviews have reported HPV prevalence in OAC to be between 13% and 35%.7 8 The limited studies that have investigated HPV in BO or OAC have yielded mixed results of unclear clinical significance. Transcriptionally active HPV has been shown to be strongly associated with Barrett’s dysplasia and OAC but not in those with BO alone, suggesting HPV may play a role in oesophageal carcinogenesis. Specimens from dysplastic Barrett’s and OAC that were positive for transcriptional markers of HPV activity lacked p53 overexpression. The majority had the wild-type TP53 which is important in HPV-driven malignancies.9–11 Both increases in HPV viral load and integration status are associated with more severe disease.12 13 HPV persistence (or p53 overexpression) predicts treatment failure after endotherapy for dysplasia or OAC.14 Iyer et al showed that using formalin-fixed samples did not detect a significant difference in p16(INK4a) expression between BO, OAC or normal oesophageal tissue.15 Previous studies have shown a negative association thought to be due to poor sample classification, inconsistent testing methodology and geographical variations.15 16
The principle aims of this pilot study were to apply a novel HPV screening tool to oesophageal tissue and to determine the prevalence rates in a small UK cohort with BO.17
Methods
Adult patients (18–85 years) attending Nottingham University Hospitals for gastroscopy for Barrett’s surveillance were prospectively recruited. The Barrett’s database was used to identify cases with non-dysplastic BO. Exclusion criteria included inability to give informed consent, emergency gastroscopy, prior upper gastrointestinal (GI) malignancy, previous upper GI surgery, current or previous HPV-associated lesions, immunocompromised patients or those post-HPV vaccination. Informed consent was obtained from all individuals prior to the use of tissue samples. Formalin-fixed paraffin-embedded oesophageal tissues of 20 patients with BO were analysed. DNA was extracted using the QIAamp DNA Tissue Kit (Qiagen, Crawley, UK). DNA yield and quality were determined by using NanoDrop 2000 (Thermo Fisher Scientific). All donated samples were screened for HPV detection by qPCR and samples that had HPV detected were reproduced three times before deemed to be HPV positive.
Real-time PCR screening
Sample screening assays were established using real-time PCR on an AB StepOnePlus Real-Time PCR System (Thermo Fisher Scientific). BrightWhite qPCR 96-well plates for ABI FAST machines and StepOnePlus (Primerdesign) were used. For this assay, the composition of the real-time PCR Master Mix per well was as follows: 10 µL of PrecisionFAST qPCR Master Mix with SYBR Green (Primerdesign), 0.4 µL of each primer, forward and reverse (200 nM), and 4.2 µL UltraPure DNase/RNase-free ddH2O. The remaining 5 µL of well volume was used for the working stocks of participant DNA, all with a concentration of 1.6 ng/µL. The final thermocycling conditions established for this assay were as follows: a hot start for enzyme activation at 95°C for 3 min, followed by 40 cycles of denaturation at 95°C for 20 s, annealing at 53°C for 30 s, and extension at 72°C for 10 s. MY09/11 primers were used for this HPV consensus screening assay. Due to the use of SYBR Green as the fluorophore indicating dsDNA amplification, a dissociation (melt) curve followed the amplification to determine the number of PCR products present per sample.
All work was carried out using the standardised aseptic techniques to prevent any cross-contamination, which included the handling of patient and control tissues in separate localities and the processing of samples in a sterile environment.
All samples were screened alongside HPV-positive controls (HeLa DNA) and HPV-negative controls (non-template controls and Ltk-11 gDNA) for direct comparison of amplification and dissociation curve data. Online software uMeltSM V.2.0.2 (Dwight, Palais and Wittwer, 2011) (Wittwer Lab) was also used to compare dissociation curve data and predict HPV status based on HPV subtype melt curve profiles.
Gel electrophoresis
PCR products were electrophoresed on 2% agarose gel using 1× Tris-borate-EDTA running buffer (89 mM Tris; 89 mM boric acid; 2 mM EDTA) to separate DNA fragments. GelRed Nucleic Acid Gel Stain (10 000× in dimethyl sulfoxide) (Biotium) was added to the agarose to permit band visualisation via ultraviolet fluorescence.
To run the gels, 10–15 µL of the PCR products was to DNA loading buffer (0.05% (w/v) bromophenol blue; 40% (w/v) sucrose; 0.1 M EDTA, pH 8.0; 0.5% (w/v) sodium lauryl sulfate (Sigma-Aldrich)). A DirectLoad PCR 100 bp Low Ladder (Sigma-Aldrich) was loaded on the 1% gels according to manufacturer’s instructions. The 1% gels ran for ~40–60 min at a range of 75–100 V and visualised using a ChemiDoc XRS+ System (Bio-Rad).
Results
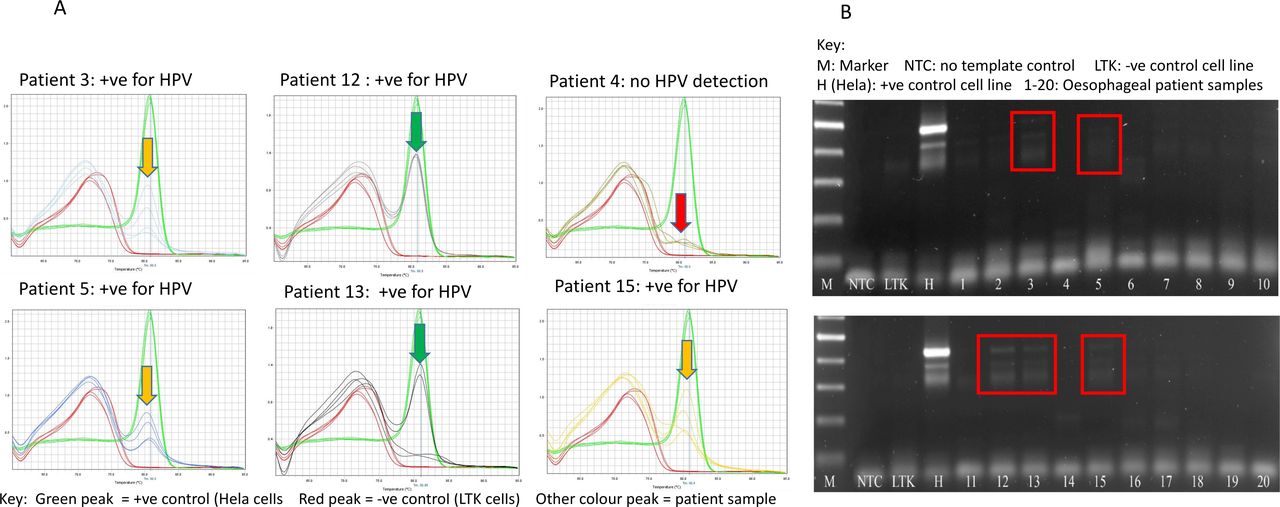
DNA extracted from archival oesophageal samples of patients with BO identified 5 out of 20 patients as positive for HPV using the qPCR screening methodology developed by Knight et al.17 The laboratory screening data are shown in figure 1, with the L1 HPV DNA clearly detected via qPCR screening and the resulting corresponding presence of a PCR product being visible via gel electrophoresis. These preliminary data indicate a possible HPV prevalence of 25% in patients with BO. The screening methodology also enables preliminary indication of the abundance of infection, with the height of the dissociation melt curve corresponding to a higher number of HPV PCR products. As indicated by the arrows, the height of the dissociation melt curves differs between patient samples, with patient 4 having no detectable dissociation curve, indicating no detectable HPV. Patients 12 and 13 have the highest dissociation melt curves when compared with the positive control. This difference in HPV abundance was confirmed by gel electrophoresis, with patients 12 and 13 producing a stronger/brighter signal than the other HPV-positive patients. Patients 15 and 5 had lower dissociation melt curves when compared with the positive control.
{kind=link}
Laboratory L1 HPV DNA screening of archival Barrett’s oesophagus (BO) samples using Knight et al’s novel HPV screening methodology. (A) Patients 12 and 13 have a high ‘relative fluorescence’ L1 HPV DNA peak (highlighted with green arrow), indicating an abundant HPV infection, while patient 4 is negative for HPV, as indicated by no relative fluorescence L1 HPV peak (highlighted with red arrow). Patients 3, 5 and 15 have a reproducible detectable relative fluorescence peak (yellow arrow), though at lower level than patients 12 and 13, indicating a less abundant HPV infection. (B) Corresponding DNA electrophoresis showing the visualisation of L1 PCR bands, with an intense PCR band for the positive control cell line (H) and varying intensity of PCR bands for the five HPV-positive patient samples. The PCR band intensity correlates with the peak height of the relative fluorescence. HPV, human papillomavirus.
Discussion
This pilot study is the first to demonstrate the adaptation of a validated oral HPV screening method for use in the oesophagus. This novel method has successfully determined the HPV prevalence rates in a small cohort of UK-based patients with BO.
The association between HPV and oesophageal squamous cell cancer has been described since the 1980s based on characteristic histological findings.18 HPV DNA is detected in approximately 66% of oesophageal squamous cell carcinoma specimens but with significant racial and geographic variations.19 20
The first evidence for a strong link in OAC was provided by Rajendra et al in 2013, demonstrating that transcriptional active high-risk HPV was associated with OAC and Barrett’s dysplasia.12 In situ hybridisation techniques have since demonstrated active HPV genome occurrence in dysplastic tissue but not in normal squamous epithelium.13
High viral load and early HPV integration have also been shown to be associated with severe disease development.13 21 HPV persistence or p53 overexpression has also been shown to predict endoscopic treatment failure.14 When next generation sequencing was carried out, the majority of biologically active patients with high-risk HPV had wild-type TP53.10 22
HPV-positive tumours have also been shown to have more favourable disease-free survival than HPV-negative tumours. Rajendra et al, in a case–control study of 142 patients with OAC and Barrett’s dysplasia, demonstrated that HPV positivity was associated with significant disease-free survival; 40.3 vs 24.1 months, p=0.003. This was also demonstrated for transcriptionally active virus, p16, E6 and E7 expression. These findings could potentially allow for future more personalised treatment based on virus status.23
A standardised testing of clinical samples to determine HPV status is highly important in HPV detection and subsequent research. Previous methodology has varied in the literature but this pilot study has demonstrated that this simple method can be accurately used in oesophageal tissue.
Adoption of a validated HPV detection tool similar to this could have a significant role to play in possible therapeutic vaccination to try to reverse HPV-associated lesions and on measuring the impact of vaccination in prevention of OAC.
However, little is known about the effectiveness of vaccination in this disease at present and the benefits of future vaccination are likely to take some time to be seen. The use of an accurate tool such as this is key.
The strengths of this study included the use of a qPCR method which is highly accurate, easily performed and cost-effective as HPV status directly impacts on clinical outcomes of individuals undergoing endotherapy. In the laboratory, the steps taken to prevent cross-contamination included discarding the first section of tissue blocks, and handling tissue sections with new equipment in addition to using acetone and alcohol to clean section areas. Positive and negative controls were also included in the PCR process.
However, there are several weaknesses of this pilot study. All patients were recruited from one centre, thus the cohort is unlikely to be generalisable to all areas in the UK. All patients had also been referred to secondary care, therefore, also possibly introducing selection bias. These factors potentially limit the generalisability of the studied samples. Furthermore, although PCR is sensitive false positives may still be produced and gel PCR assessment can be subjective at times. Although DNA electrophoresis has provided some quantifiable data on different levels of infection, accurate viral load could not be determined without type-specific screening. In future studies, measuring transcription activity using detailed molecular techniques would aid in determining the biological role of HPV in Barrett’s metaplasia rather than just assessing its presence.
In addition, the small sample size, lack of dysplastic and adenocarcinoma tissue, as well as established positive and negative controls make it difficult to fully interpret the accuracy of these results. However, such detailed assessment was always going to be beyond the scope of this simple pilot evaluation. Further studies should also assess whether there is any difference when this method is used on fresh frozen samples instead of paraffin-embedded samples as used in this study.
As this method has yielded positive results, the next stage going forward is the assessment of this method on a large cohort of patients including non-dysplastic Barrett’s, dysplastic Barrett’s and OAC. This future planned work would validate the method and provide a better understanding of prevalence in the UK. HPV strain testing could also be carried out to determine the common strains in the UK cohort. Viral load and oncogenic gene expression could also then be quantified and correlated with disease outcomes. Whole genomic sequencing of HPV-associated OAC could also be carried out to fully determine the viral integration to help form better insight into HPV-driven OAC. Once complete, a final intervention study could then be carried out in the form of a double-blind placebo-controlled vaccination study in HPV-infected dysplastic Barrett’s individuals using GTL001 (ProCervix) to further understand the role HPV plays in cancer development.
In conclusion, the adoption of this screening test for use in oesophageal tissue could potentially start to revolutionise future research in this area. If a clear link between HPV and Barrett’s dysplasia is proven with this method, it could aid in monitoring and/or in dysplasia detection in patients with BO by stratifying those most at risk and aiding in the development of new therapies.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Nottingham Health Sciences Biobank (REC reference: 15/NW/0685). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
DNA extraction was carried out by Professor Mohammad Ilyas research team at the University of Nottingham.
References
Footnotes
Contributors Guarantor of the article: GK. Conception and study design: GK, JRW, KR, PK. Real-time PCR and gel electrophoresis experiments: AW, EM. Article writing: JRW. All the authors approved the final version of the article. JRW and KR's research is supported by the National Institute for Health Research (NIHR) through the Nottingham Biomedical Research Centre, Nottingham University Hospitals NHS Trust and the University of Nottingham.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health.
Competing interests KR has received consultancy, research and educational grants from Olympus, Pentax, Cook, Boston Scientific, Medtronic and ERBE.
Provenance and peer review Not commissioned; externally peer reviewed.