Article Text

Abstract
Introduction Biliodigestive leaks are typically caused by an insufficiency at the surgical anastomosis. Biliodigestive anastomosis (BDA) insufficiencies can lead to bilomas, abscesses and vascular erosion in chronic conditions.
Material and methods We performed a retrospective analysis of the medical and radiological records of all patients with biliodigestive insufficiency who received interventional treatment between July 2015 and February 2021. Nine patients (three with unilateral drainage and six with bilateral drainage) were treated with a modified percutaneous transhepatic cholangiodrainage (PTCD). Clinical success was considered after complete resolution of the peribiliary collections, absence of bile within the surgical drains, radiological patency of the BDA (contrast medium flowing properly through the BDA and no signs of leakage) and haemodynamic stability of the patient without signs of sepsis.
Results Clinical success was achieved in all nine patients. No patients required revision surgery to repair their BDA. The mean indwelling drainage time was 34.8±16.5 days. The mean number of interventional procedures performed per patient was 6.6±2.0.
Conclusion Patients who present with BDA insufficiency may benefit from interventional radiological techniques. Our modified PTCD resolved the BDA leak in all nine cases and should be considered as a valuable option for the treatment of patients with this complication. Our technique demonstrated to be feasible and effective.
- bile
- bile duct surgery
- bile secretion
- cholangiocarcinoma
- pancreatic cancer
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known about this subject?
Biliodigestive anastomosis (BDA) insufficiencies can develop into bilomas, abscesses and can cause severe haemodynamic descompensation as well as peritonitis. Revision surgery must be weighed against radiologic and endoscopic interventions to diagnose and treat this complication. Interventional techniques like percutaneous transhepatic cholangiodrainage can provide an accurate diagnosis of the site of leakage and can help establish a biliary drainage with the goal of restoring continuity between the biliary system and the digestive system.
What are the new findings?
We describe our method to establish a proper insufficiency diagnosis and effective treatment using minimally invasive techniques and clinical follow-up. Key points to resolve this condition are the accurate position and size of the drains, performing frequent controls and continuous assessment of drainage output. Although the interventional treatment could be considered long, clinical success was achieved in all nine patients and no patients required surgical revision of their BDA.
How might it impact on clinical practice in the foreseeable future?
Percutaneous treatments already provide an alternative to endoscopy and surgery for treating early postoperative biliary complications. The presented approach for BDA insufficiency aims to share consistency for choosing the best approach. Interventional radiologists, surgeons and endoscopists could benefit from this work as a new concept to treat unstable patients with BDA leakage after hepatobiliary surgery.
Introduction
Biliodigestive anastomosis (BDA) is a common procedure in hepatobiliary surgery; it can be performed as hepaticojejunostomy, hepatojejunostomy (portoenterostomy) and hepaticoduodenostomy. Hepaticojejunostomy, established as the standard technique for BDA, is classically performed proximal to the cystic duct and 2–3 cm below the bifurcation of the hepatic duct. The most frequent complications arising after the creation of a BDA are insufficiency (0%–10%), stenosis (0%–15%) and bleeding (0%–36%).1
BDA insufficiency often occurs due to technical problems, such as lack of tightness of the surgical anastomosis and inadvertent surgical injuries. Other causes are often related to biliary ischaemia as seen with hepatic artery thrombosis and hepatic artery stenosis. BDA insufficiencies may develop into bilomas, abscesses and cause vascular erosion in chronic conditions. Typical signs of BDA insufficiency include bile discharge through surgical drains (Jackson Pratt drains), haemodynamic decompensation and biliary peritonitis. Alterations in liver function tests are not accurate indicators of biliary leaks. Therefore, understanding the imaging spectrum of BDA insufficiency and knowledge of proper interventional procedures is mandatory.2
In BDA insufficiency, revision surgery must be weighed against radiological or endoscopic intervention. According to the International Study Group of Liver Surgery (ISGLS), revision surgery is indicated when patients present with a severely compromised clinical condition, and leakage is due to complex duct transection or complete hepatojejunal dehiscence (Grade C). Radiological or endoscopic interventions are reserved for patients with a mild or moderate clinical condition (Grade A and B).3 The goal of radiologic or endoscopic techniques is to restore the normal biliary flow into the small bowel by placing a stent or drainage across the defect allowing ‘diversion’ of bile and ultimately progressive healing of the BDA.
Endoscopic stenting is usually first line treatment but unfortunately this method frequently fails to reach the site of the biliary leak for example due to intestinal modifications performed during the Whipple procedure. Interventional radiological (IR) techniques like percutaneous transhepatic cholangiodrainage (PTCD) may be used to provide an accurate overview of the site of leakage and can help establish a biliary drainage with the goal of restoring continuity between the biliary system and the digestive system.4–6
Objective
To evaluate the clinical efficacy of a modified PTCD in the treatment of BDA insufficiencies and to analyse technical factors, treatment duration and mortality in patients after complicated hepatobiliary surgery.
Material and methods
We performed a retrospective analysis of the medical and radiological records of all patients with BDA insufficiency who received modified PTCD between July 2015 and February 2021. Clinical and demographic characteristics of the study population are shown in tables 1 and 2.
Clinical and demographic characteristics of nine patients with biliodigestive anastomosis (BDA) insufficiency who received modified PTCD
Detailed clinical characteristics of nine patients with biliodigestive anastomosis insufficiency who received modified PTCD
BDA insufficiency was suspected when patients presented with bile discharge through the surgical drains during the postoperative period and when patients showed clinical signs of mild or severe haemodynamic decompensation. According to the ISGLS definition, bile leaks were considered when total bilirubin levels in the abdominal drain fluid reached three times the serum concentration starting from the third postoperative day.3 Serum liver function tests and inflammatory parameters (ie, C-reactive protein and white blood cell count) were continuously assessed.
Non-invasive imaging
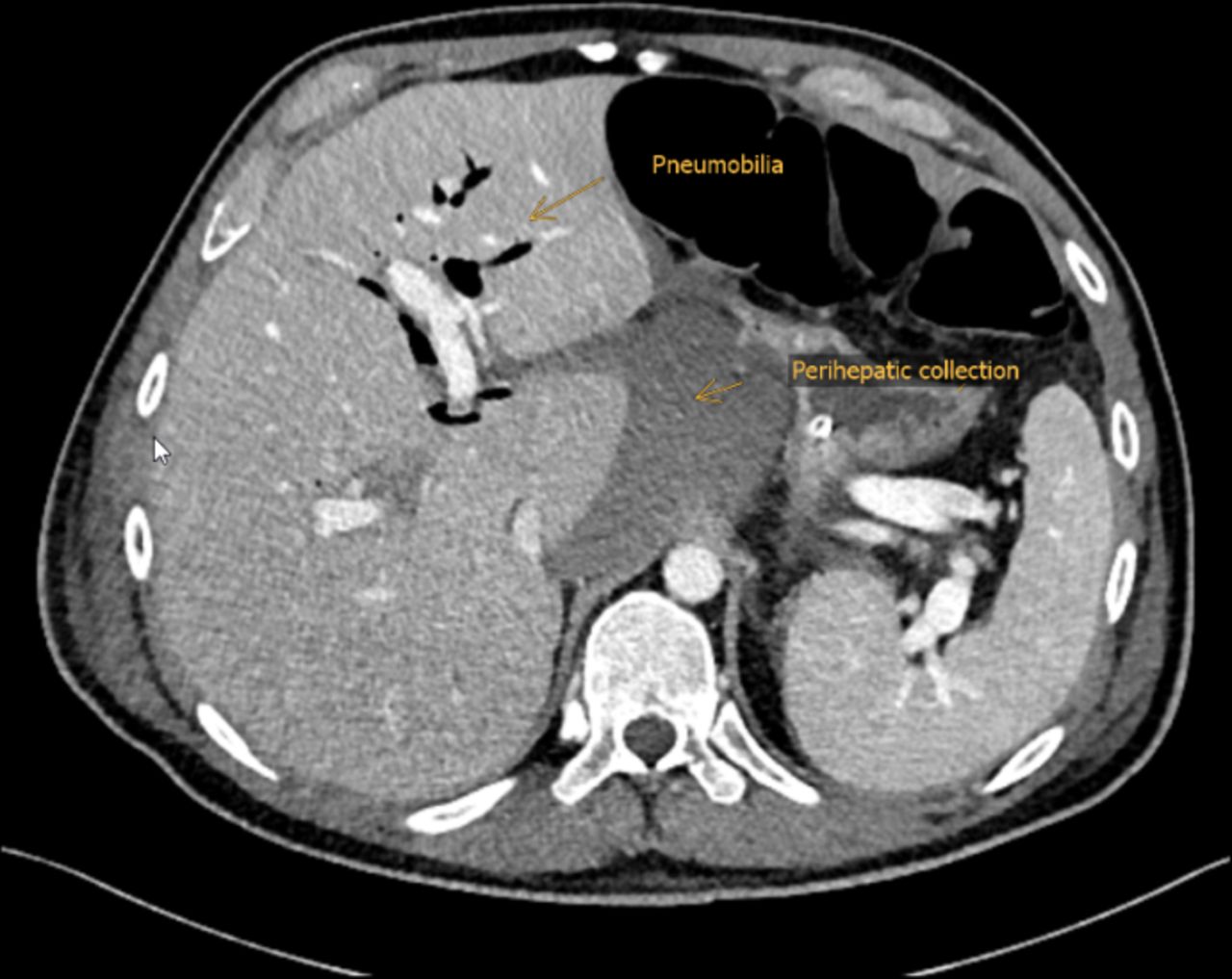
Ultrasound and CT are highly sensitive for detecting BDA insufficiency and rely on the following findings: free fluid in the right upper quadrant adjacent to the BDA, identification of variable amounts of free air adjacent to the BDA and pneumobilia in non-dilated intrahepatic biliary ducts (figure 1).
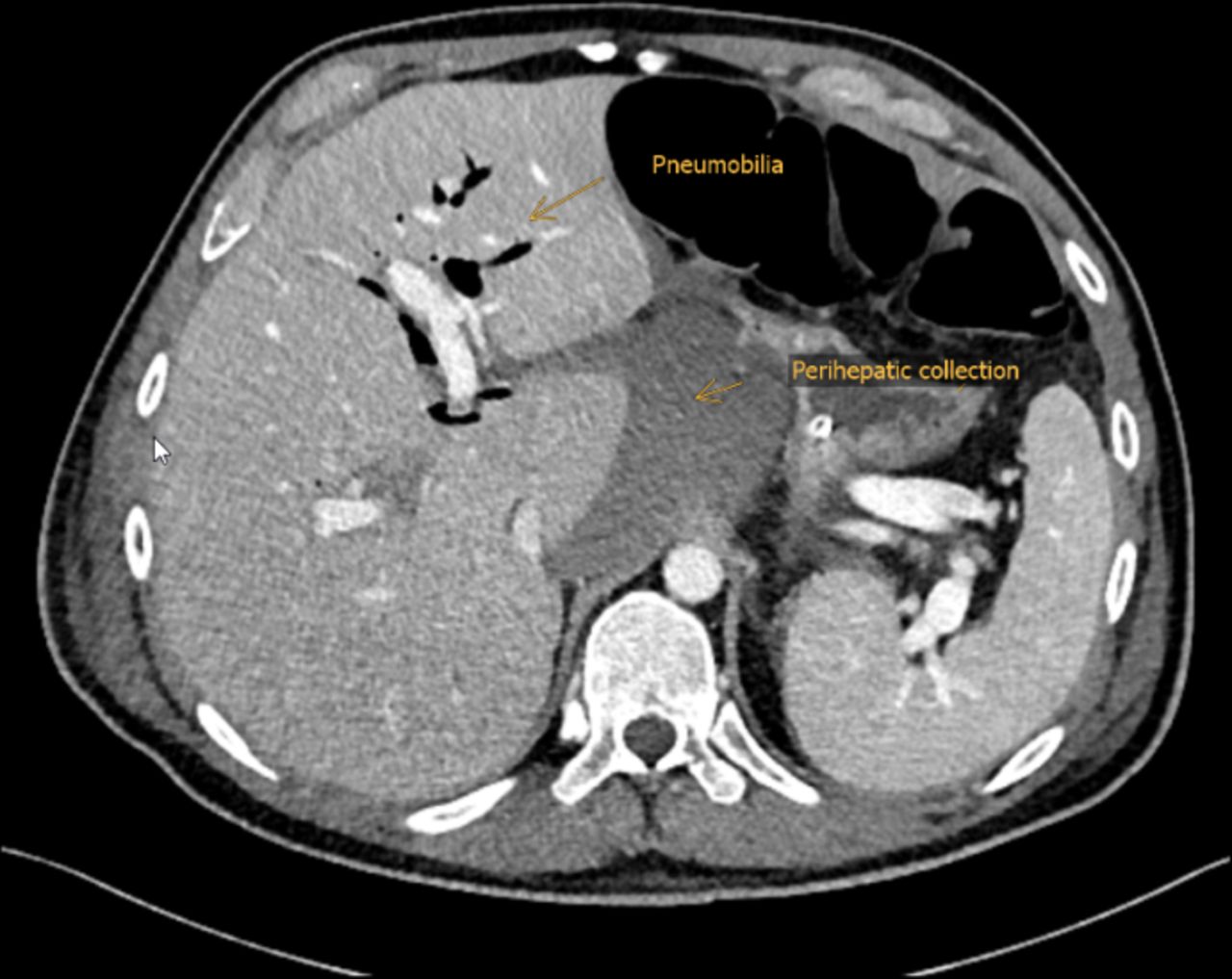
CT demonstrating signs of BDA insufficiency (perihepatic collection, the presence of pneumobilia in the left liver lobe and a small amount of free intraperitoneal air). BDA, biliodigestive anastomosis.
Invasive imaging
Percutaneous cholangiography is the gold standard for the diagnosis of BDA insufficiency. The pathognomonic finding is extravasation of contrast medium at the anastomotic area and filling of contrast of the surgical drains (Jackson-Pratt drains) (figure 2).
Fluoroscopy showing extravasation of contrast medium to the left side of the BDA and contrast uptake by the surgically placed drain (Jackson Pratt drain). BDA, biliodigestive anastomosis.
Interventional treatment steps
Sedation and analgesia were always provided by the anesthesiology team. Periinterventional antibiotics were usually not administered since the patients were usually already under broad-spectrum antibiotic therapy.
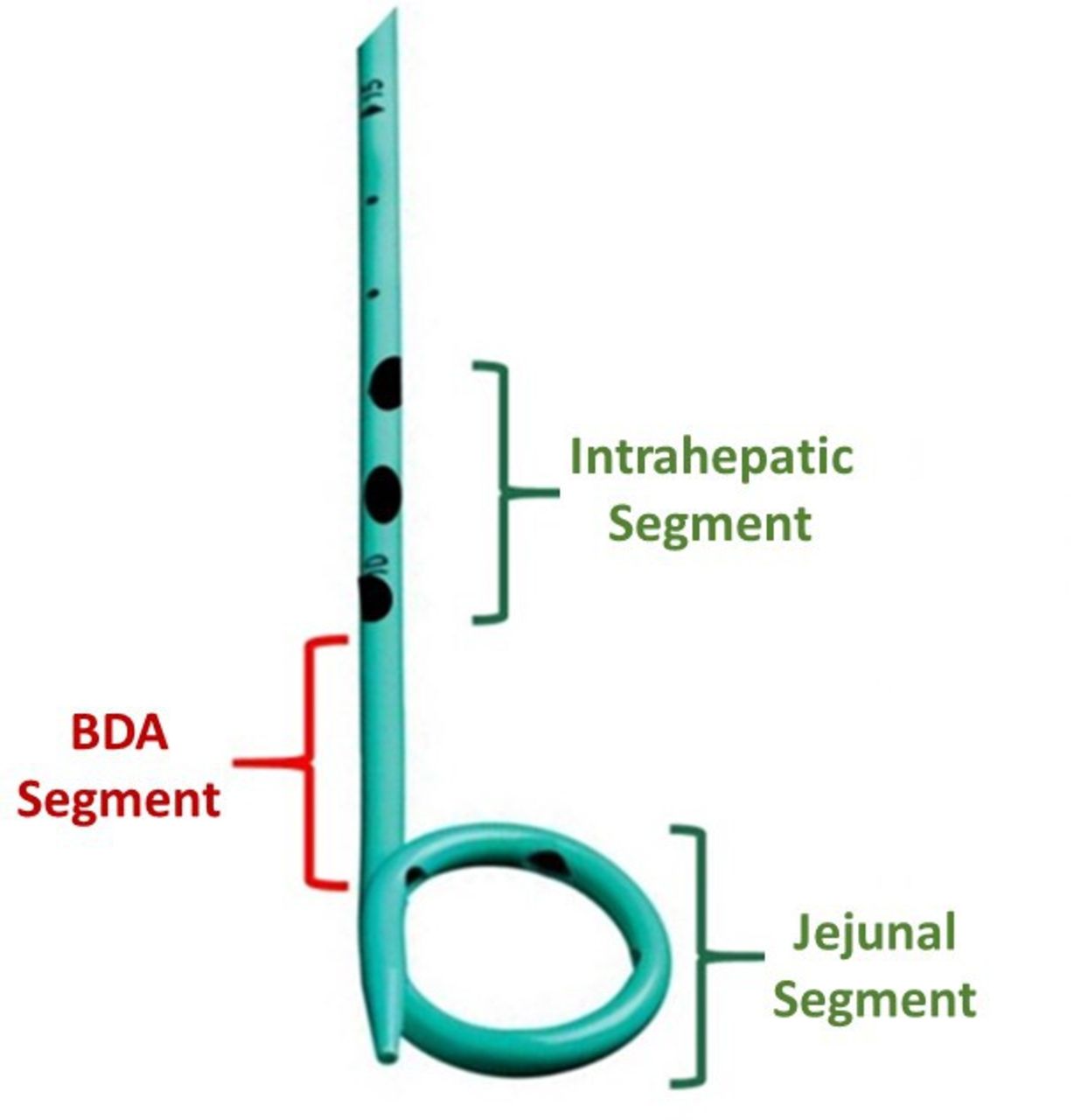
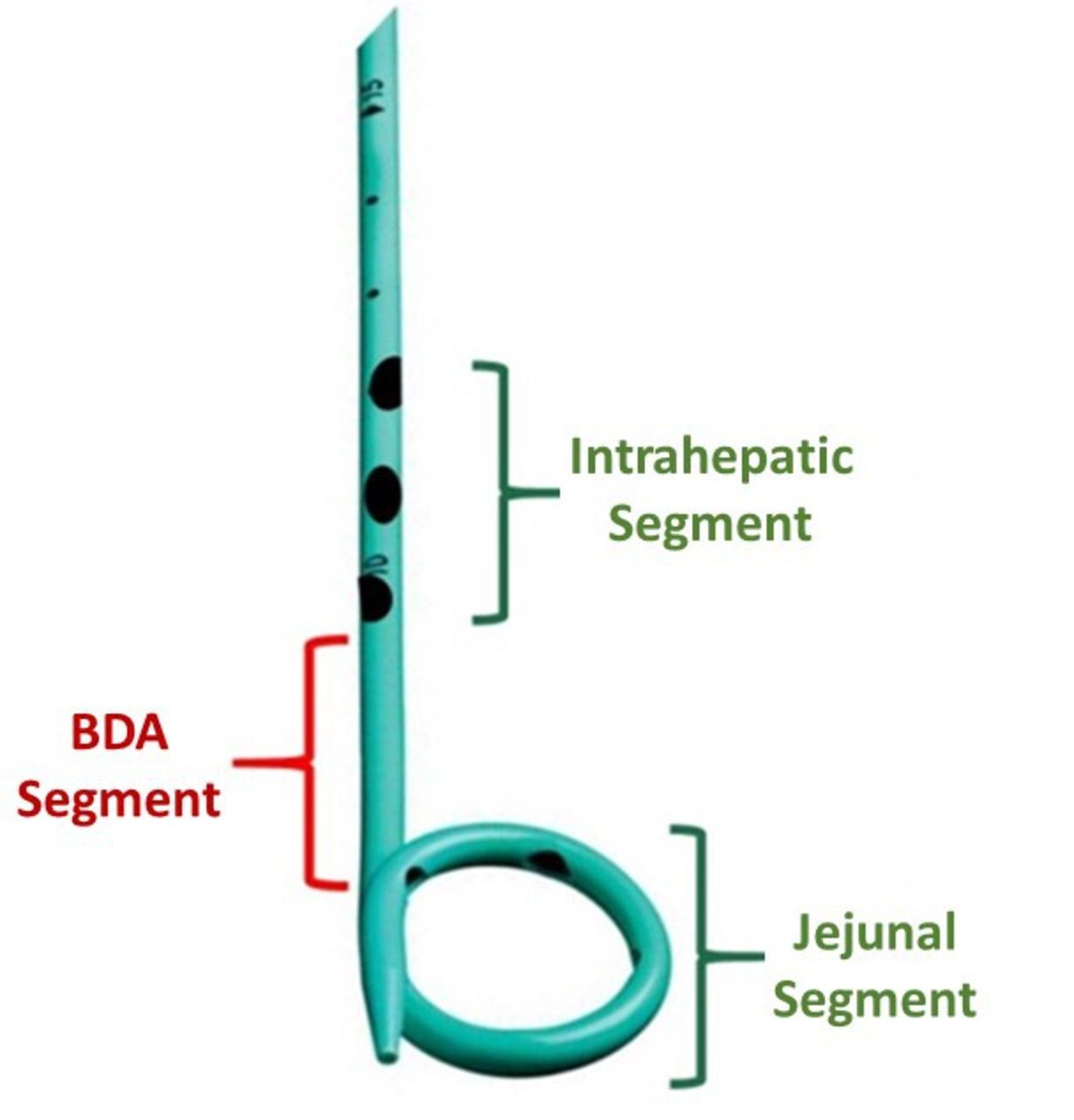
A 21-gauge Chiba needle was used for percutaneous cholangiography. After performing the cholangiogram (usually by puncturing the right biliary branches), a 0.018-inch guidewire was inserted into the duct through the Chiba needle. The Neff introducer set (Cook Medical, Bloomington, Indiana, USA) ensured access into the biliary system and facilitated the introduction of a 0.038-inch guidewire and 4Fr/65 cm Berenstein catheter (Cordis, Santa Clara, California, USA). When a leak was detected through the 4Fr catheter cholangiography, a stiff guidewire was advanced past the BDA into the intestinal loop. Subsequently a modified biliary drainage catheter (figure 3) was placed over the stiff guidewire, and the drain segment without sideholes was placed exactly at the level where the leak was initially detected.

Modified drainage catheter used for treating BDA insufficiency. BDA, biliodigestive anastomosis.
Most cases required bilateral drains (right and left biliary access) in which the steps were repeated on the contralateral side. The use of bilateral drains is recommended to ensure that the whole internal diameter of the common hepatic duct and the anastomotic area are completely outlined.
Since anatomical differences between patients exist, not all patients are treatable with the same drainage diameter. We typically start with bilateral 10Fr modified drains and larger diameters can subsequently be exchanged to completely outline the common hepatic duct diameter. Final cholangiography is performed through both drains and both drains are sutured to the skin to avoid dislocation.
To promote the healing process of the BDA and to keep the anastomotic segment ‘dry’ or excluded from bile, the drainage catheters had proximal intrahepatic and distal intestinal orifices and were set to internal–external drainage mode.
Modified biliary drains
A modified PTCD consists of a 25 or 35 cm pigtail abscess/nephrostomy drainage catheter (Argon, Frisco, Texas, USA) in which proximal sideholes are manually created with scissors to allow the entrance of bile from the intrahepatic biliary ducts (entrance point), leaving a central segment (approximately 4–5 cm) free of holes (figure 3).
Drain output record
A daily record of the output of all drains (surgical and interventional) must be kept in order to have a registry of the balance between bile drained through the surgical drains and bile drained through the intrahepatic drains. Factors indicating satisfactory function of the intrahepatic drains include: reduction or disappearance of bile through the surgical drains (Jackson-Pratt) and an increasing amount of bile through the intrahepatic modified drains. The intrahepatic modified drains must be flushed gently once a day (only via injection; no aspiration) with 10 mL of sterile saline. The drains should be evaluated at least weekly under fluoroscopy, taking into account the correct position of the sideholes and the presence or absence of BDA insufficiency signs.
Postprocedure BDA assessment
For better assessment of the BDA, it is recommended to temporarily exchange the modified drainage catheters with 8Fr or 9Fr sheaths over a stiff 0.038-inch guidewire and to perform a cholangiography via the sheaths. After the cholangiography has been performed, the sheaths are once again replaced with new modified biliary drainage catheters. Postprocedure BDA assessment should be repeated weekly or every 2 weeks until the BDA insufficiency resolves completely.
If a single drain does not seem to adequately outline the diameter of the BDA, a larger calibre drain or alternatively a second drain must be inserted from the contralateral side. In certain cases, it was even necessary to place bilateral modified 14Fr drains. Patience is a crucial factor for treatment success. The time it takes for a BDA insufficiency to heal and become hermetic and functional depends on several factors such as the size of the defect, nutritional and immune status of the patient and correct position and diameter of the drains. When there is no radiological evidence of bile leakage (figure 4), the drainage catheters can be removed and tract embolisation with Gelfoam slurry should be performed.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Digital subtraction fluoroscopy showing healed biliodigestive anastomosis after 48 days of treatment.
Results
Nine patients with BDA insufficiency who received modified PTCD between July 2015 and February 2021 were included into our study (three received unilateral drainage and six received bilateral drainage). The patients underwent BDA due to malignancy of the pancreas (3), malignancy of the duodenum/papilla vateri (3) and iatrogenic bile duct injury during laparoscopic cholecystectomy (3) (tables 1 and 2). Of the nine patients, six were males and three were females.
All BDA insufficiencies occurred at the hepaticojejunostomy anastomosis. Four cases demonstrated bile leaking from the left side of the BDA, two cases centrally and three cases on the right side. One patient had a concomitant BDA stenosis that was successfully treated with balloon cholangioplasty.
A total of three patients received unilateral drainage with a single drain that adequately covered the diameter of the BDA. A total of six patients received bilateral drains as the BDA was not adequately covered by a single drain. Three cases of BDA insufficiency were resolved using 10Fr drains (two bilateral and one unilateral), four cases required 12Fr drains (three bilateral and one unilateral), one case resolved with bilateral 14Fr drains and one case only required a unilateral 8Fr drain.
The mean number of interventional procedures was 6.6±2.0 which mainly consisted of control cholangiographies to verify the correct position of the drains and to assess the status of the biliary leak. Clinical success was considered after complete resolution of the peribiliary collections, absence of bile within the surgical drains, radiological patency of the BDA (contrast medium flowing properly through the BDA and no signs of leakage) and haemodynamic stability of the patient without signs of sepsis. Clinical success was achieved in all cases (100%) with mean indwelling drainage time being 34.8±16.5 days. No patients required revision surgery to repair the BDA and no patients showed complications related to the modified PTCD procedure.
Survival and mortality
The 90 days survival after the endovascular treatment was 100%. There were no deaths related with the interventional therapy or due to other complications during the time when the patients were treated.
Long-term survival after treatment
Late deaths or complications related to our treatment were not reported even in those cases who survived 5 years after the end of the treatment.
Discussion
BDA insufficiency is associated with increased mortality if not treated prompt and properly. According to current literature, the reported overall 90-day mortality of bile leaks is 1.9% for grade A, 2.5% for grade B, and 25% for grade C, mainly due to severe infections and development of sepsis.7
Comparing results between centres remains challenging, even with similar patient populations.6 Percutaneous treatments currently provide a valuable alternative to endoscopy and surgery for treating early postoperative biliary complications. Information about percutaneous treatments in BDA insufficiency is not always consistent and there is no standardised consensus for the best approach (bilateral vs unilateral drains), material selection (biliary drains vs nephrostomy type drains vs modified drains) and length of therapy until healing is achieved. Treatment strategies for severe bile leaks vary significantly between centres and are dependent on hospital resources such as the availability of a dedicated interventional radiology team.
One of the most important challenges of the interventional treatment is convincing medical teams that this therapy requires time and patience to ensure a complete healing of the BDA defect.
The main reason for percutaneous treatment failure is the premature removal of the transhepatic drains before the healing process is completed. An early removal of the transhepatic biliary drains invariably leads to an early recurrence in the BDA leak. In a retrospective study by Fonio et al, IR percutaneous treatment achieved clinical success in 92.5% of BDA fistulas using transhepatic conventional biliary drains, with a mean indwelling catheter time of 34.9 days and an average of 4.1 interventional procedures, resulting in a perioperative mortality rate of 1.2% and an overall recurrence rate of 6.7%.8
Although the time to resolve a BDA insufficiency and the number of required interventions in our study were similar to the results of Fonio et al, we observed an overall higher clinical success (100%) with no recurrences, complications or mortalities.
Promising results using self-expanding, retrievable metallic stent-grafts for biliary leaks have been reported. These stents can be placed and retrieved via endoscopic or percutaneous approaches. Nevertheless, stenting is significantly associated with the presence of drug-resistant bacteria in bile samples and longer postoperative length of stay.9 The modified PTCD technique has the advantage that new drains are exchanged weekly thus minimising the risk of bacterial colonisation of the material and reducing the risk of superinfection.10 11
Anastomotic lesions secondary to scar formation, local ischaemia or technical issues may coexist with BDA insufficiencies. They are usually located exactly at the anastomosis and are frequently associated with the development of biliary concrements with a reported incidence of 4%–9%. These can be treated with an IR standard approach that involves establishing percutaneous transhepatic biliary access, dilating the stricture with balloon cholangioplasty and placing an internal–external biliary drainage catheter. Multiple prolonged dilatations are often necessary to obtain reasonable results.12 In our study, only 11.2% of the patients presented with a concomitant biliary stenosis that resolved completely after balloon cholangioplasty.
Haemobilia or fresh blood within the drains may occur when the transhepatic drainage catheter intersects a vascular structure (venous, portal or arterial branch), this may cause haemorrhagic shock or catheter obstruction after clot formation within the lumen. In these cases, repositioning the drain with correct positioning of the orifices in order to occlude the vascular communication may provide relief. Pseudoaneurysm formation has also been reported when biliary drains are placed. In these cases, the diagnosis can be made with CT angiography to locate the vascular injury. Afterwards, treatment may require removal of the catheter over a wire followed by selective angiography for precise location and embolisation of the bleeding artery.13–15
In the past, some authors have argued that any demonstration of bile leakage should be managed with prompt surgical repair.16 However, new studies have demonstrated that 96% of biliary leakages treated solely with IR techniques resolved completely without residual stenosis and with a low complication rate and a procedure-related mortality of 0%.17 In our study, all patients who underwent modified PTCD were alive at the time of finishing this manuscript and no patients experienced any complication related to the procedure.
Our study had several limitations, including the retrospective, single-centre nature of the investigation and the small number of patients.
Nevertheless we could probe that patients with bilio digestive insufficiency after hepaticojejunostomy may benefit from IR techniques as an initial option for the accurate diagnosis and treatment of this condition. Our modified percutaneous drainage technique seems to be a promising alternative to the conventional PTCD drainage with higher success rates. Meanwhile, more evidence is needed before IR therapy meets its maximum potential and multidisciplinary research should continue to further standardise this concept in our community.
Supplemental material
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but all procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. This study was approved by our institutional review board.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @tomrdc
Contributors RLB was the main author of the manuscript. PSB, JER, IZ, AS and J-MG participated in the data collection, analysed the data and drafted the paper. TRdC provided technical and administrative support and provided a critical review of the intellectual content of the article. All authors read and approved the final manu-script.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.