Article Text

Abstract
Liver transplantation (LT) is the only curative therapy in patients with end-stage liver disease. Long-term survival is excellent, yet LT recipients are at risk of significant complications. Biliary complications are an important source of morbidity after LT, with an estimated incidence of 5%–32%. Post-LT biliary complications include strictures (anastomotic and non-anastomotic), bile leaks, stones, and sphincter of Oddi dysfunction. Prompt recognition and management is critical as these complications are associated with mortality rates up to 20% and retransplantation rates up to 13%. This review aims to summarise our current understanding of risk factors, natural history, diagnostic testing, and treatment options for post-transplant biliary complications.
- endoscopic retrograde pancreatography
- liver transplantation
- biliary strictures
- bile duct surgery
- hepatobiliary surgery
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- endoscopic retrograde pancreatography
- liver transplantation
- biliary strictures
- bile duct surgery
- hepatobiliary surgery
Introduction
Liver transplantation (LT) has revolutionised the care of end-stage liver disease. Since the first human LT in 1960s, advances in preoperative assessment, surgical technique, postoperative care, immunosuppression, and antiviral therapy have dramatically improved graft and patient survival.1 2 Currently, the 1-year, 3-year, and 5-year patient survival rates are 91.8%, 83.8%, and 76.1%, respectively.3 Yet biliary complications remain a major source of morbidity and mortality in LT patients, with an incidence ranging from 10% to 15% in deceased donor transplants. With living donor liver transplant (LDLT), the risk is even higher, ~15%–30%.4 Prompt recognition and management is critical as these complications are associated with retransplantation and mortality rates as high as 13% and 19%, respectively.5
Common post-LT biliary complications include anastomotic strictures (AS), non-anastomotic strictures (NAS), bile leaks, bile duct stones, bile casts, bilomas, and sphincter of Oddi dysfunction (SOD) (table 1).6 Prompt recognition and treatment of post-LT biliary complications reduces morbidity and mortality and improves graft survival.7 8 This review provides an up-to-date summary of epidemiology, pathogenesis, risk factors, diagnostic testing, and treatment options for post-LT biliary complications.
Biliary complications following orthotopic liver transplantation
Bile leak
Post-orthotopic liver transplantation (OLT) bile leaks can be divided into early (<4 weeks post-OLT) and late (>4 weeks post-OLT). Bile leaks are further subclassified into anastomotic versus non-anastomotic leaks.9 10
Early bile leaks most commonly occur at the anastomotic site, with ischaemia being an important mechanism. In theory, the risk of bile leak is lower with choledochocholedochostomy (duct-to-duct) compared with choledochojejunostomy (Roux-en-Y) because duct-to-duct anastomosis leaves the recipient bile duct better vascularised. In clinical practice, data have not clearly demonstrated a difference in the rate of bile leaks between these two types of anastomoses.1 11 Procedure-related risk factors that may predispose to ischaemia at the anastomosis include excess tension, extensive dissection of the donor bile duct on procurement, and the amount of electrocautery used to control bleeding from cut ends of donor and recipient bile ducts.9 12 13 An important postoperative risk factor is hepatic artery thrombosis (HAT), which can cause necrosis of the anastomosis, leading to strictures or leaks (figure 1). LDLT requires donor hilum dissection and dissection of the recipient bile duct. These manoeuvres can result in biliary devascularisation and increase ischaemic time. In a meta-analysis, the pooled risk of bile leak was 7.8% for deceased donor liver transplant (DDLT) and 9.5% for LDLT. In more recent studies, the bile leak rate was 7.1% with DDLT vs 11.8% with LDLT (p<0.03).14 15

Image showing a single, severe anastomotic biliary stricture with duct disruption and subsequent bile leak found at the post-transplant anastomosis.
With regard to late bile leaks, important risk factors are T-tube placement at the anastomosis or recurrence of an early bile leak. Because of the increased incidence of T-tube-associated bile leaks, their use has decreased over the past two decades.16 Non-anastomotic bile leaks typically occur from the donor or recipient cystic duct remnants. The aetiologies may be iatrogenic (eg, improper ligation) or a distal obstruction that can occur from a mass, stricture, or stone. A less common aetiology is injury to the liver surface from the transplant itself. This aetiology is more common with LDLT.17
Clinicians should suspect bile leak in any post-LT patient with worsening liver enzymes of unclear aetiology, which should prompt abdominal imaging or bilious fluid noted from peritoneal drains.9 Bile leaks can result in abdominal pain, and fever if infected; but in many instances, leaks can occur without any of these typical symptoms. Initial abdominal imaging should include liver ultrasound with Doppler to evaluate for biliary dilatation and hepatic artery anastomosis. Over the past two decades, MRI has evolved as a highly sensitive and non-invasive alternative to percutaneous or endoscopic cholangiogram.18–20 Occasionally, MRI may not identify small leaks, in which case endoscopic or percutaneous cholangiogram may be necessary.
Once a bile leak is determined, the type of intervention depends on the anatomy allowing access to the biliary tree. In a duct-to-duct anastomosis, endoscopic retrograde cholangiopancreatography (ERCP) is the first-line intervention. For small leaks, a sphincterotomy alone is sufficient; stents are often used for larger leaks.21 22 Nasobiliary catheters and percutaneous transhepatic biliary drainage (PTBD) through interventional radiology are also options in the setting of a major bile leak.23 Overall, success with ERCP is reported to be from 80% to 90%.24 25 Surgery is largely reserved for large leaks that lead to uncontrollable infection and sepsis, or leaks presumed secondary to ischaemia that are unlikely to improve with stenting or percutaneous drainage.
In patients with choledochojejunostomy, the Roux limb contains the remnant bile duct, which makes endoscopic access challenging. These patients typically require percutaneous drainage.26 Recent publications have described successful cases of endoscopic ultrasound (EUS)-guided antegrade drainage approaches.16 23 Surface injury from LDLT is treated with either percutaneous drainage or surgery.22
Biliary stones, sludge, and casts
Bile duct filling defects (BDFDs) like biliary sludge, casts, and stones are another important biliary complication post-LT, occurring in about 3%–6% of patients.27 28 BDFDs can occur with any physiological process that slows the flow of bile leading to an increase in viscosity.29 30 The slow flow of bile can lead to formation of a cast or stone composed of bilirubin, collagen, bile acids, cellular debris, and cholesterol. Thus, any aetiology that slows bile flow (eg, biliary strictures, ischaemia, infection, cellular rejection, and medications) can predispose to sludge, casts, and stones. Biliary strictures are a particularly important risk factor for BDFDs; up to 45% of patients with BDFD have a concurrent stricture.10 Strictures often arise as a result of ischaemic injury to bile duct mucosa (eg, hepatic artery thrombus, ‘cold’ time during the transplant, or surgical technique). Similarly, infections and acute cellular rejection predispose to BDFDs because they disrupt bile duct epithelial cells.30 Any medication that causes cholestasis can predispose to BDFDs. For example, ciclosporin inhibits bile salt secretion, which induces cholestasis and thereby increases risk of BDFDs.31 In terms of BDFD risk based on type of anastomosis, one older study suggested that there was a slightly increased risk with choledochojejunostomy. Subsequent studies failed to show any difference in risk of BDFDs based on type of anastomosis.32
Bile casts are dark and hard in appearance and formed by lithogenic material confined to the bile duct dimensions. Casts occur most frequently in the common hepatic and right and left main intrahepatic ducts. They were first described after LT in the late 1970s when patients presented with multiple intrahepatic biliary strictures leading to large casts.33 As with bile duct stones, the major risk factor is ischaemia, in particular the amount of ‘warm’ time compared with ‘cold’ time.34 Additionally, if T-tubes and internal stents do not pass into the small bowel after the biliary anastomosis sutures dissolve, they can serve as a nidus for cast formation.35
The diagnosis of BDFD relies on clinical factors such as abdominal pain and more objective data such as rise in liver enzymes, usually in a cholestatic pattern.36 These findings should prompt liver imaging to rule out a hepatic artery thrombus and to evaluate the biliary ducts. MRI is highly sensitive at identifying BDFDs. The characteristic finding is a high signal intensity.
ERCP is the first-line approach for BDFDs in patients with choledochocholedochal anastomoses. Standard techniques including sphincterotomy, balloon dilatation, and balloon and basket retrieval are highly effective. Mechanical, electrohydraulic, and laser lithotripsy have been used successfully in patients with large or complex BDFDs.24 25 In patients with choledochojejunostomy, successful removal of BDFD using balloon-assisted ERCP and EUS-guided approaches has been reported.37 More frequently, percutaneous drainage performed by interventional radiology is used in this setting.17 36 The evidence supporting ursodeoxycholic acid for BDFDs is limited and inconsistent.
Sphincter of Oddi stenosis
A less common complication of post-LT is SOD, also known as papillary dysfunction. SOD was initially classified into three subtypes using the Milwaukee classification: type I is believed to represent true sphincter stenosis and is most likely to respond to endoscopic therapy; type II likely represents an overlap between a structural dysfunction and a motility disorder; and type III represents functional biliary type pain.37 More recently, the Rome III criteria has advocated for the removal of SOD type III to be replaced by the more accurate terminology of functional biliary or pancreatic SOD.38 SOD type I is suspected in the setting of distal common bile duct (CBD) dilatation and elevated liver enzymes without an obvious stricture. One proposed mechanism involves injury to the innervation of the sphincter of Oddi leading to hypertonia.38 39 Data on SOD are quite limited and focused on studies involving manometry from the 1990s. Based on these studies, there were elevated resting basal pressures at the sphincter of Oddi demonstrated in patients who had an LT with choledochocholedochostomy anastomosis.40 41 In addition, T-tube manometry findings were also analysed showing elevated resting CBD pressures. Currently, the use of T-tube has been less prevalent due to the associated complications and manometry is also no longer routinely used as its utility has been questioned.
From a clinical standpoint, abnormal elevations in liver enzymes in a cholestatic pattern without a clear mechanical obstruction such as a stone or stricture should lead to consideration of SOD. Interventions include ERCP with sphincterotomy and consideration of stent placement.42 In extreme cases, surgery for conversion from a choledochocholedochostomy to a choledochojejunostomy has been reported.
Vanishing bile duct syndrome
Vanishing bile duct syndrome (VBDS) is a rare complication of LT. VBDS is defined as small bile duct loss caused by acute or chronic cellular rejection.42 43 The proposed pathogenesis of VBDS with acute cellular rejection is a T cell response against bile duct cells, leading to destructive cholangitis, severe ductopaenia, and portal tracts without bile ducts.44 VBDS with chronic rejection is still not fully understood, but some studies suggest macrophage activation which leads to histological features of lobular hepatitis, marked hepatocyte apoptosis, and small bile duct injury.45–47 Acute and chronic rejection may occur as a result of cytomegalovirus (CMV) infection, medications (eg, sertraline), and ischaemic cholangitis as the instigating event.48 Case reports have described resolving ductopaenia, but such resolution appears to be highly unpredictable. Acute VBDS almost inevitably requires retransplantation.49
Anastomotic strictures
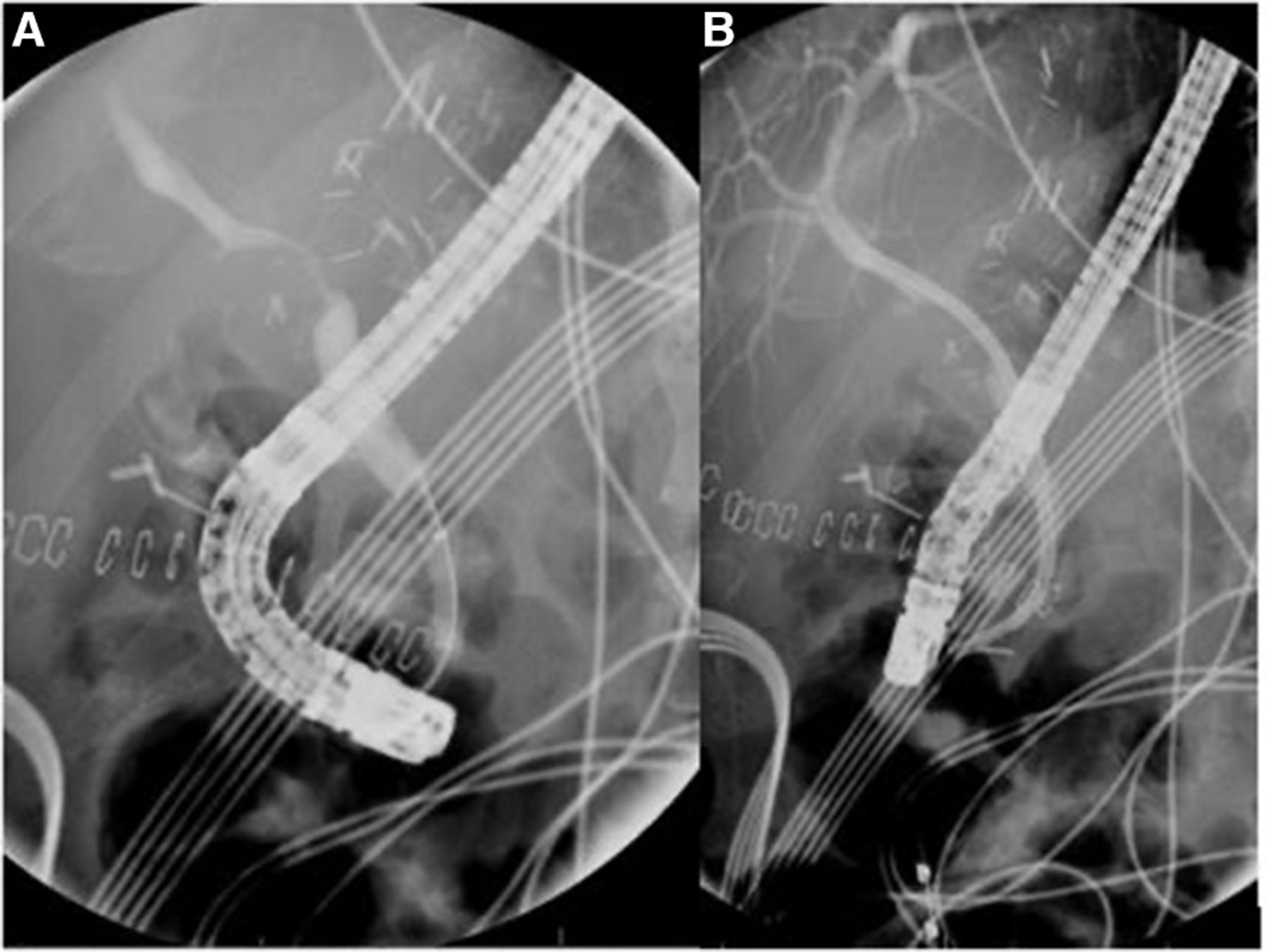
AS are a localised narrowing at the site of biliary anastomosis between the donor and recipient bile duct and are typically single and short (figure 2). They can present any time after transplantation, but the majority are diagnosed within 12 months following LT.50 The cumulative risk of AS increases with time (6.6% at 1 year and 12.3% at 10 years).51 AS are more common than non-anastomotic biliary strictures and constitute up to 86% of all biliary strictures post-LT.52
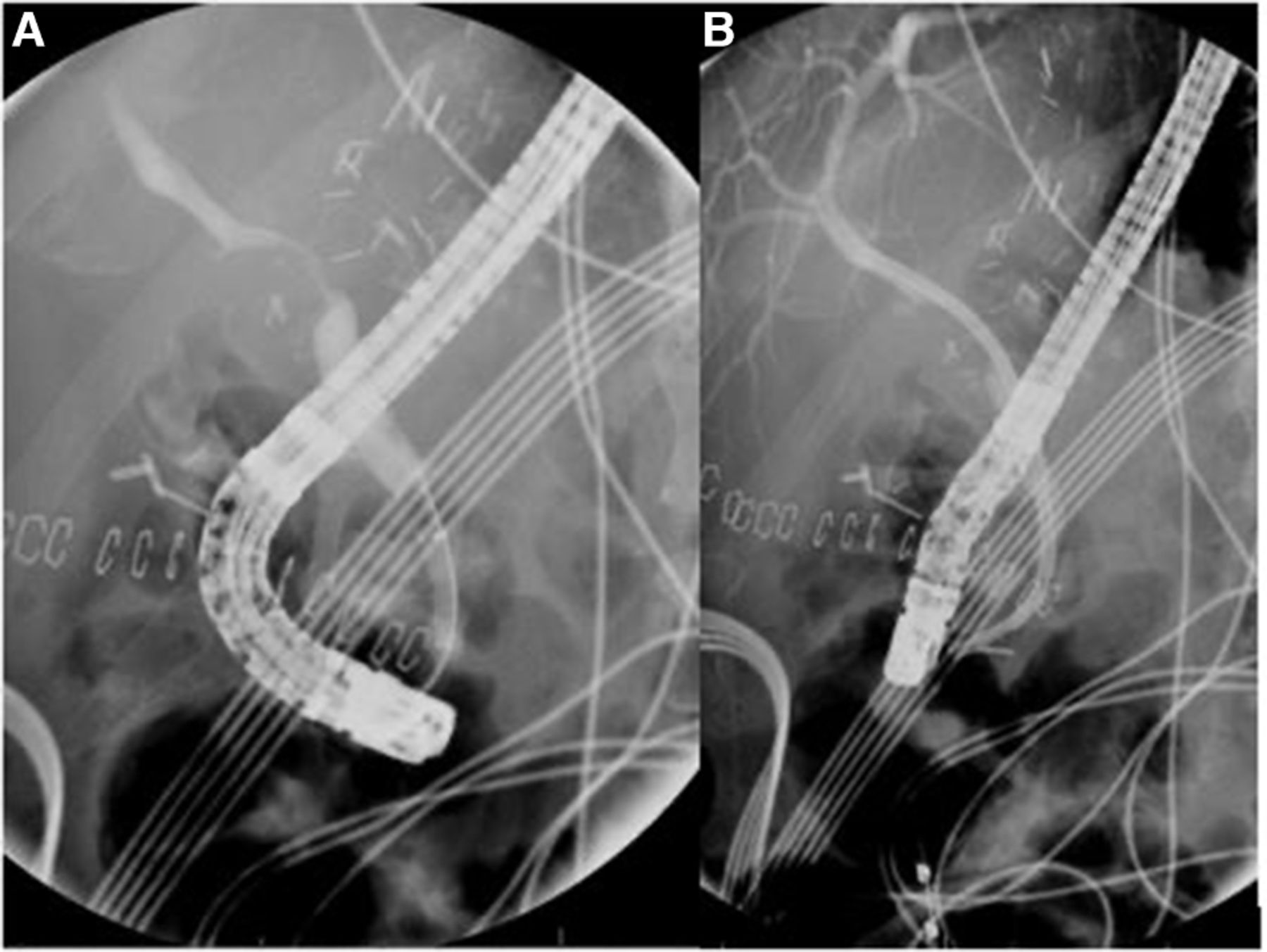
Fluoroscopic image demonstrating a severe anastomotic stricture (A) following endoscopic placement of plastic stent across the anastomotic site (B).
The pathophysiology for the development of AS is believed to be ischaemia or fibrosis of the bile duct following a suboptimal surgical technique or a bile leak in the early postoperative period.53 In patients presenting early after LT, AS likely result from technical issues during surgery. These include small calibre of the bile ducts, size mismatch between the donor and recipient ducts, postoperative bile leak, inappropriate suture material, tension at the anastomosis, and excessive use of cauterisation to control bleeding.54 Although many risk factors have been implicated in the development of AS, there is discordance among studies. Risk factors for the development of AS can be grouped into several broad categories, including ischaemic (surgical technique, longer intensive care unit (ICU) stay, and longer cold and warm ischaemia times), genetic factors, and inflammatory (CMV, Epstein-Barr Virus, and acute/chronic cellular rejection).55 56
The clinical presentation of AS can differ significantly, with some presenting with signs of biliary obstruction (abdominal pain, jaundice, fever, chills, cholangitis, and anorexia) and some discovered incidentally in asymptomatic LT recipients due to persistent elevations in cholestatic liver function tests. As many other post-LT complications (HAT, acute cellular rejection, choledocholithiasis) may present in a similar fashion, the diagnosis of AS requires a high clinical suspicion prompting radiographic or endoscopic confirmation. To date there have been no biomarkers or biochemical abnormalities that can diagnose AS with adequate accuracy.57
Because of the relatively low cost and convenience, transabdominal ultrasound is often the first radiographic test performed when biliary stricture is suspected. Unfortunately, its ability to assess the anastomotic site is dismal, with a sensitivity ranging from 30% to 70%.58 Similarly, the use of CT scan has led to suboptimal results, with a reported accuracy of diagnosing AS of around 40%.59 MRI/magnetic resonance cholangiopancreatography (MRCP) is the most accurate radiological test for AS, with a reported sensitivity and specificity of up to 95%.60 MRCP can accurately demonstrate a focal luminal narrowing across the biliary anastomosis, but not all narrowing are clinically relevant so close attention to the clinical context is essential.61 Endoscopic retrograde cholangiography (ERC) is the invasive gold standard diagnostic test, but interobserver variability is reported even with invasive cholangiography; ERC is generally reserved for therapeutic rather than diagnostic purposes.53
T-tubes were once thought to protect against the development of AS, but more recent data have not demonstrated reduction in AS with T-tube. In fact, routine use of T-tubes may even lead to an increase in overall biliary complications.62 63 Because AS are unifocal, short-segment, and located within the extrahepatic bile duct, they are easily amenable to endoscopic or percutaneous therapy. While the success rates between endoscopic therapy and PTBD are similar, PTBD is associated with higher recurrence rates, increased patient discomfort, and increased risk of complications such as drain dislodgement or infection.64–66 As a result, endoscopic therapy with ERCP is the first-line approach for the management of AS.
Endoscopic treatment options include balloon dilatation or stenting. Treatment failure and recurrence rates are much higher with balloon dilatation alone, or placement of a single stent when compared with placement of multiple plastic stents (MPS).64 In a meta-analysis assessing the effectiveness of MPS, resolution rates of 94%–100% were reported.67 Patients typically required between three and four endoscopic sessions over the course of 12 months, with recurrence after an initial resolution occurring in up to 37%. An alternative to MPS is the placement of a single fully covered self-expandable metal stent (FCSEMS) across the anastomosis. While they are relatively easy to deploy, care is required to ensure that the proximal end of the stent is distal to the bifurcation to avoid obstructing flow from one lobe of the liver to the CBD. One approach to mitigate this complication is to prophylactically deploy plastic stents into the secondary branch ducts to prevent their occlusion. While cost-effective studies are needed, a meta-analysis comparing the effectiveness of FCSEMS with MPS demonstrated similar rates of AS resolution, but found that FCSEMS reduced the number of ERCP procedures (mean difference: 1.69 ERCP; p<0.01) and duration of treatment (mean difference: 40.2 days; p=0.03).68
Refractory AS have been treated with a myriad of novel endoscopic techniques, including magnetic compression anastomosis (MCA) and cholangioscopy-guided steroid injection with balloon dilatation. MCA has been shown to be effective in treating up to 88% of refractory AS.69 A novel through-the-scope magnet has demonstrated similar rates of success while overcoming the technical difficulties of prior methods.70 In a small case series by Franzini et al,71 cholangioscopy-guided steroid injection in conjunction with balloon dilatation was a safe, effective, and durable therapy for refractory AS. Historically, endoscopic therapies were not considered for patients with altered foregut anatomy (eg, Roux-en-Y hepaticojejunostomy or choledochojejunostomy), but recent novel approaches, including laparoscopic-assisted ERCP, balloon-assisted ERCP, and EUS-directed transgastric ERCP, have made endoscopic therapy safe and feasible.72–74
Non-anastomotic strictures
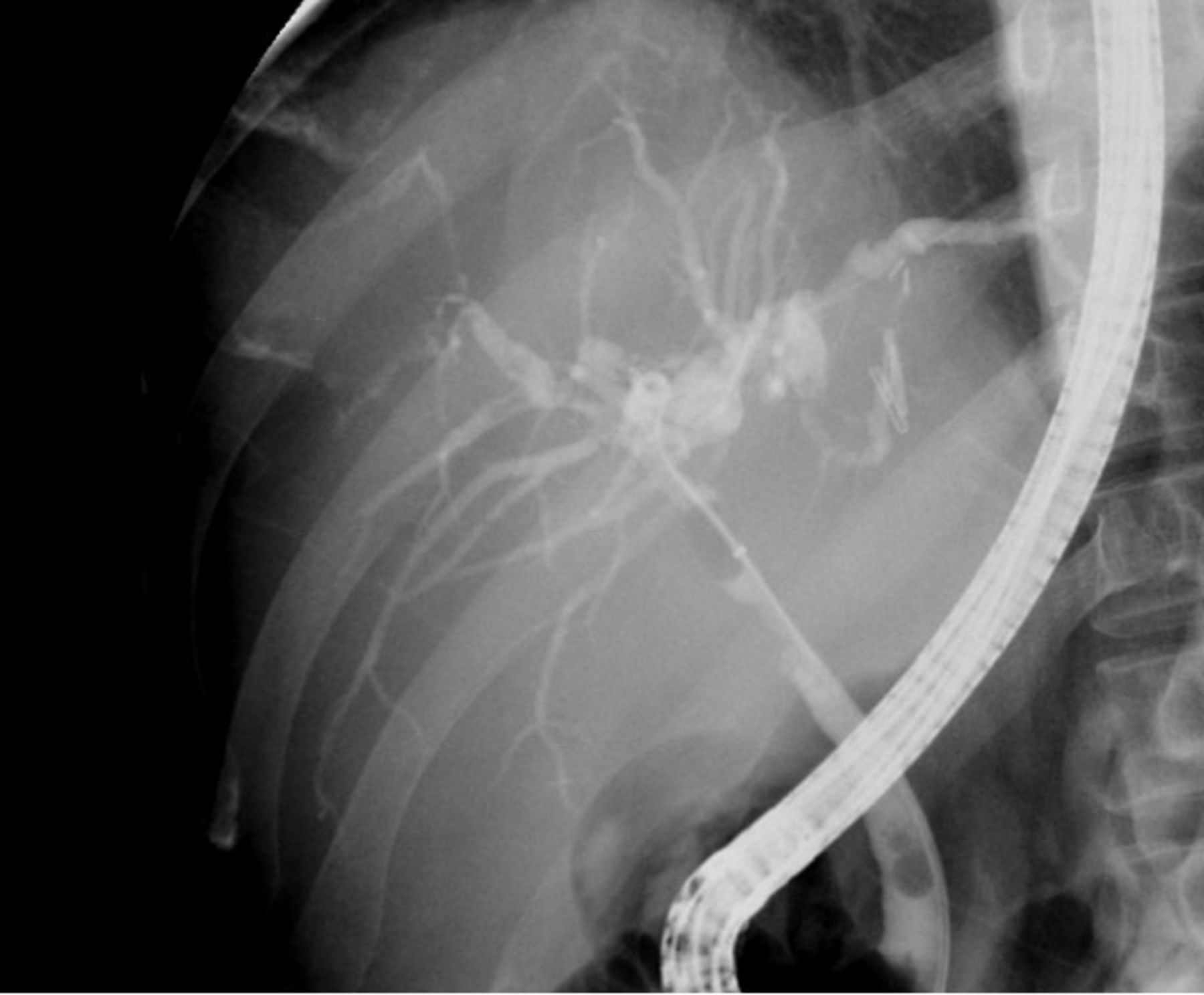
NAS, also referred to as ischaemic-type biliary strictures, are defined as a stricture, dilatation, or irregularity of the intrahepatic or extrahepatic bile ducts of the liver graft proximal to the anastomosis (figure 3).53 NAS are associated with significant morbidity and mortality, with graft loss of up to 46%.75 NAS typically present at a median of 6 months post-LT and recent long-term studies have documented that the incidence of NAS gradually increased from 10% at 1 year to ~16% at 10 years post-LT.53 76
{kind=link}
{kind=link}
{kind=link}
Fluoroscopic image demonstrating several areas of narrowing and dilatation representing non-anastomotic strictures. There is also bile duct filling defect seen in the distal common bile duct likely representing a gallstone in the recipient duct.
Similar to AS, the risk factors for the development of NAS can be grouped into several broad categories, including ischaemic (HAT, surgical technique, longer ICU stay, and longer cold and warm ischaemia times), grafts from donation after cardiac death, genetic factors, and inflammatory (CMV, Primary sclerosing cholangitis, autoimmune hepatitis, and acute/chronic cellular rejection).77–79
Like AS, the diagnosis of NAS is often challenging as the initial clinical presentation may be variable and often subtle. Some patients present with signs and symptoms of biliary obstruction, while others are asymptomatic and identified incidentally based on abnormal liver enzymes or imaging. Other subtle clues may include new-onset jaundice, Gram-negative sepsis, or signs of graft failure. Transabdominal ultrasound is often the first non-invasive test but is limited in its ability to identify NAS, with sensitivities for detecting NAS ranging between 38% and 66%.80 The sensitivity of hepatobiliary scintigraphy with 99-technetium labelled iminodiacetic acid is similarly only 65%–75%.81 CT scan has a sensitivity >80% for NAS, but its specificity is only ~70%.59 MRI/MRCP is the most accurate non-invasive test for NAS, with sensitivities and specificities as high as 95%.82
NAS are a challenging biliary complication following LT because they may occur at multiple locations and are frequently resistant to minimally invasive endoscopic and percutaneous therapies. Medical management is generally used initially and involves optimisation of immunosuppression along with treatment of complications such as sepsis. Given the challenges in management, prevention of NAS has become an important focus of research over the last decade. Machine perfusion has become a promising technique to prevent bile duct injury at the time of transplant.83 These initial findings were supported by several studies which again demonstrated decreased incidence of NAS in those who underwent dual hypothermic oxygenated machine perfusion.84 85
Endoscopic therapy generally involves maximal endoscopic stenting with MPS with or without balloon dilatation, yet results have been suboptimal, with a success rate around 50%.86 87 The success rate in those with LDLT has been reported to range from 25% to 33%.88 As a last resort in non-responders, endoscopic therapy may also serve as a bridge to retransplantation.89 PTBD insertion has similar efficacy as endoscopic management for NAS, but complications such as drain malfunctions and patient discomfort preclude its use unless endoscopic management fails, in altered surgical anatomy or peripheral lesions not amenable to endoscopic therapy.90 Surgery or retransplantation is typically reserved for patients who fail endoscopic or percutaneous therapy or progress to graft failure.64
Conclusion
Biliary complications remain a major source of morbidity after LT and are commonly encountered. Considerable inroads have been made in understanding the aetiology and natural history of these complications. Minimally invasive endoscopic therapies have obviated the need for repeat surgery or retransplant in a large proportion of patients, yet gaps remain in our understanding of the pathogenesis of many of these complications, which has curtailed the development of prophylactic therapeutics or interventions to prevent their occurrence.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
References
Footnotes
Contributors MF: conception and design, analysis and interpretation of data, drafting of the article, critical revision of the article for important intellectual content, figure design, final approval of the article. MP, LK: critical revision of the article for important intellectual content, final approval of the article. TS: conception and design, critical revision of the article for important intellectual content, final approval of the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests TS: CSA Medical research advisory board, Allergen research support, Research support Lucid.
Provenance and peer review Commissioned; externally peer reviewed.