Article Text

Abstract
Background Infliximab is an efficacious therapy for inflammatory bowel disease and may play a role in management of some extraintestinal manifestations. While higher trough levels of infliximab are associated with higher rates of disease remission, the association between trough levels of infliximab and arthralgia activity characterised as an extraintestinal manifestation has yet to be defined.
Objective We aimed to assess the association between serum trough levels of infliximab and peripheral arthralgia activity in patients with inflammatory bowel disease.
Design In this cross-sectional study, we identified patients with inflammatory bowel disease on infliximab therapy with known history of arthralgias attributed to an extraintestinal manifestation. Collected variables included disease phenotype, medications (such as thiopurines or methotrexate), Harvey Bradshaw Index, partial Mayo score, C reactive protein, trough levels of infliximab and anti-infliximab antibodies. The primary outcome was active patient-reported arthralgia.
Results Out of 267 patients included, 65 (24.4%) had active arthralgias at the time the trough level of infliximab was measured. No significant differences in trough levels were seen between those patients with and without arthralgias. Patients on combination therapy with methotrexate or thiopurines or those with detectable anti-infliximab antibodies were not more likely to have inactive arthralgias (OR 0.99, 95% CI 0.57 to 1.74, p=0.99 and OR 1.94, 95% CI 0.9 to 4.1, p=0.09, respectively).
Conclusions This study suggests that although therapeutic drug monitoring of infliximab can have a role in the management of Crohn’s disease and ulcerative colitis, it does not seem to be useful in managing arthralgias associated with inflammatory bowel disease.
- inflammatory bowel disease
- crohn's disease
- ulcerative colitis
- infliximab
- arthritis
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known about this subject?
Infliximab is an efficacious therapy for inflammatory bowel disease and some of its extraintestinal manifestations. Although higher infliximab trough levels are associated with higher rates of disease remission, the association between infliximab levels and arthralgia activity is not known.
What are the new findings?
In this retrospective, cross-sectional study of 267 patients, we found no significant difference in infliximab trough levels in patients with and without active arthralgias.
How might it impact on clinical practice in the foreseeable future?
The use of therapeutic drug monitoring of infliximab may not help manage peripheral arthralgias associated with inflammatory bowel disease.
Introduction
Inflammatory bowel disease (IBD), which includes ulcerative colitis (UC) and Crohn’s disease (CD), is characterised by chronic inflammation of the gastrointestinal tract. In addition to its effect on the digestive tract, IBD can affect nearly any organ. Patients may present with dermatological, hepatobiliary, rheumatological and ophthalmological extraintestinal manifestations (EIMs). Of these, joint symptoms involving both peripheral and axial joints are the most common EIM occurring in up to 40% of patients.1 2
Peripheral arthralgias in IBD cause little to no joint destruction yet can have a significant impact on quality of life.3 There are two types of peripheral arthralgia/arthropathy in IBD, both of which are seronegative.4 Type I arthropathy tends to be acute and self-limiting. It generally follows disease activity and affects six or fewer large joints including ankles, knees, hips, wrists and elbows.4 5 This type of peripheral arthralgia usually improves with treatment of intestinal inflammation. Type II arthropathy is less common and is usually polyarticular in nature, involving five or more small joints. Type II arthropathy does not typically parallel disease activity.4 5
The monoclonal chimeric anti-TNFα antibody drug infliximab is an effective treatment for induction and maintenance of remission of both CD and UC. It is also known to be an effective treatment of some EIMs, including arthropathies.6 7 Higher trough levels of infliximab (TLI) are associated with higher rates of clinical and endoscopic remission in IBD. Conversely, the presence of antibodies to infliximab (ATI) is associated with lower TLI, loss of response and worse outcomes. Mounting evidence regarding these associations has positioned the use of therapeutic drug monitoring (TDM) as an important tool in the management of IBD.8 9 However, the use of TDM to optimise therapy of EIM in IBD has yet to be defined. The aim of this study is to assess the association between TLI and peripheral arthralgia activity in patients with IBD.
Materials and methods
Study design and inclusion criteria
This retrospective, cross-sectional study included patients with IBD who were being treated with infliximab between 2009 and 2020 at Froedtert Memorial Lutheran Hospital and the Medical College of Wisconsin in Milwaukee, Wisconsin.
Inclusion criteria included history of IBD confirmed clinically and endoscopically, age ≥18 years, treatment with infliximab maintenance therapy (with or without immunomodulator), a history of EIM of peripheral arthralgias. Additionally, patients had to have a TLI measured within 2 weeks of having an assessment of their arthralgias as part of their routine medical visits and had to have been on a stable dose of infliximab and immunomodulators (if applicable). Patients were excluded if they had incomplete medical records or if they were on systemic corticosteroids, narcotic pain medication and/or non-steroidal anti-inflammatory drugs. Patients were also excluded if they had another diagnosis known to induce arthralgias such as rheumatoid arthritis (RA) or a musculoskeletal injury.
Data abstraction
Demographic, clinical and laboratory data were abstracted from the electronic medical record. Diagnosis of IBD was established using ICD codes and confirmed using review of the medical chart based on clinical, endoscopic, histological and/or radiologic criteria. Current use of immunomodulator therapy (methotrexate or a thiopurine) in addition to infliximab was noted. Disease location and severity were based on clinician documentation of endoscopic reports and were also abstracted. Clinical disease scores including the Harvey Bradshaw Index (HBI) for CD and Partial Mayo Score (PMS) for UC and the Short IBD Questionnaire (SIBDQ) were extracted from the chart. The HBI, PMS and SIBDQ are routinely performed at every clinic visit and documented by the treating physician at our medical centre. TLI and ATI were measured using a drug tolerant, homogenous mobility shift assay (HMSA) or an ELISA. If multiple TLI or ATI levels were available for a single study participant, the most recent values were used. At our institution, TDM is performed proactively or reactively to optimise therapy. Serum albumin and C reactive protein (CRP) levels were noted if performed on the day that the TLI and ATI were drawn. All noted laboratory values were within 14 days of assessment of IBD and arthralgia activity.
Peripheral arthralgia definition and outcomes
The attribution of peripheral arthralgias to being an EIM was at the discretion of the treating physician. Peripheral arthralgia activity or inactivity was self-reported by patients and stratified as present or absent. The documentation of the presence or absence of active peripheral arthralgias is routinely documented as part of the clinic note template at our medical centre. The primary outcome of the study was active patient-reported arthralgia within 2 months of the TLI. The secondary outcome was IBD remission, defined as a normal CRP as per our laboratory assay (<0.5 mg/dL) in combination with either an HBI <5 in CD or PMS <2 in UC.
Statistical analysis
Descriptive statistics were used to examine the baseline characteristics of the study population. Continuous variables were compared using Student’s t-test or the Mann-Whitney U-test (for nonparametric variables). The χ2 test was used to evaluate distributions of categorical variables. Pairwise and Spearman’s rank correlation coefficient were used to measure statistical dependence between two parametric and non-parametric variables, respectively. Receiver operating characteristic (ROC) curves were generated to identify the association between TLI with arthralgia inactivity and with IBD remission. P values were calculated two tailed, and a p<0.05 was considered significant.
Results
Baseline characteristics
The study population comprised a total of 267 patients, 190 of whom had CD (71.2%) and 77 of whom had UC (28.8%). Mean age was 41 years; 58.4% of patients were women. The median time on infliximab at the time the TLI was drawn was 14 months (IQR 8–34). Of the 267 TLI tests done, 94 (35%) were performed using an ELISA test and the remainder using a HMSA. The number of patients on infliximab combined with an immunomodulator (either methotrexate or a thiopurine) was 144 (53.9%). Specifically, the number of patients on infliximab and methotrexate was 36 (13.5%) and the number of patients on infliximab in combination with a thiopurine was 108 (40.4%). The baseline characteristics of the study population are shown in table 1. The majority of patients enrolled in the study were receiving the standard infliximab dose of 5 mg/kg of body weight every 8 weeks. The distribution of the infliximab dosing regimens that patients were receiving is shown in online supplemental table 1.
Supplemental material
Baseline characteristics of study population
Among all study participants, the median TLI was 9 mg/dL (IQR 3.3–19.8). A total of 36 patients (13.5% of the study population) had detectable ATI. However, of the 94 patients that had TLI/ATI measured using an ELISA, 83 (88%) had detectable TLI and ATI were not measured. There was a negative correlation between infliximab drug levels and CRP (r=−0.3, p<0.0001) and a weakly positive correlation between infliximab drug levels and serum albumin levels (r=0.18, p=0.008). Median TLI was also higher in those patients receiving combination therapy in comparison with those on infliximab monotherapy (10.8 vs 6.3, p=0.009); however, these patients on combination therapy were not less likely to have detectable ATI (OR 0.56, 95% CI 00.28 to 1.15, p=0.11).
When evaluating presence of other concomitant EIMs in addition to arthralgias, ocular manifestations (including both active and inactive ocular EIMs) were present in 11% of patients with active arthralgias while only present in 3% of patients with inactive arthralgias (p=0.011, table 2). On the other hand, there was no statistically significant difference in presence of concomitant PSC in patients with active and inactive arthralgias (table 2). Patients with active arthralgias had significantly lower SIBDQ scores when compared with those that did not (table 2).
Differences between those patients with and without active arthralgias
Peripheral arthralgia activity and infliximab levels
Of the total 267 patients included in the study, 75 patients (28.1%) had active arthralgias at the time the TLI was drawn. We found no statistically significant differences between the patients with active (n=75) and inactive peripheral arthralgias (n=192) regarding age, gender, body mass and subtype of IBD (table 2).
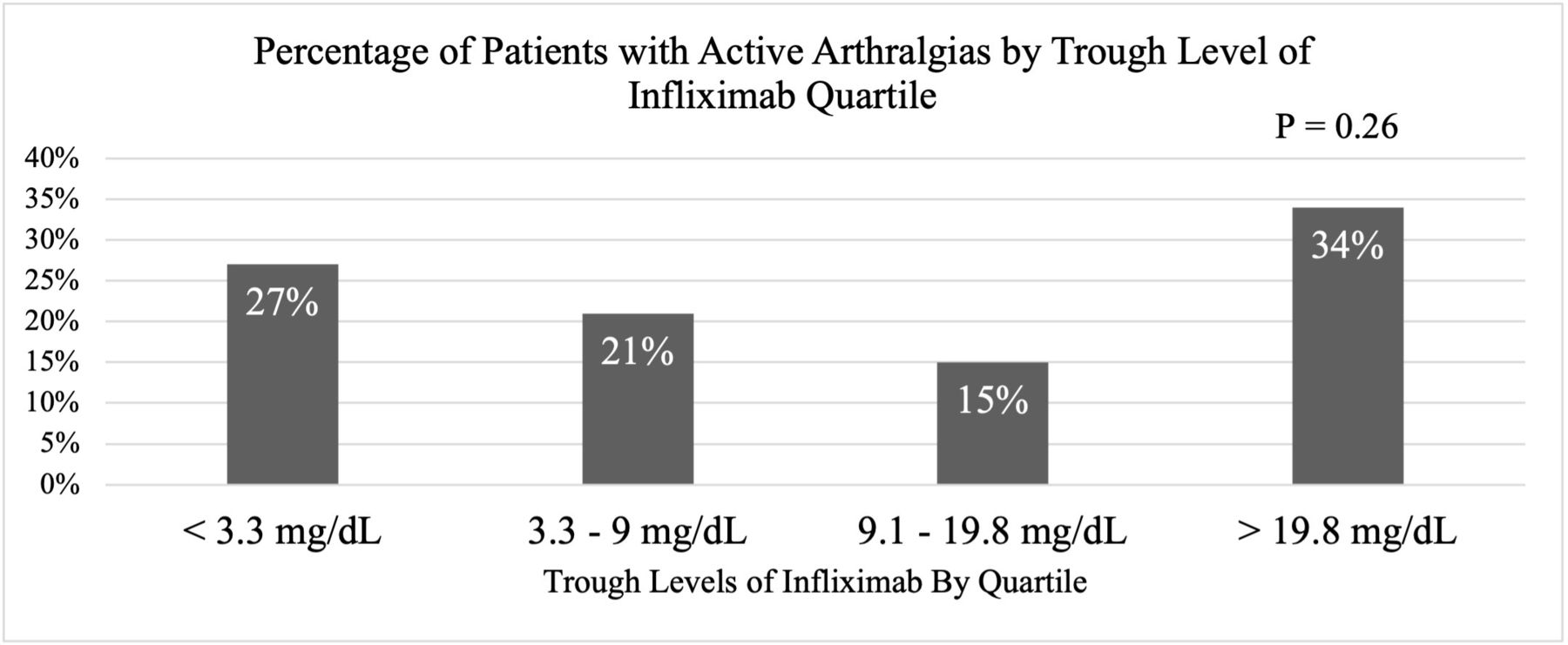
There was no difference in median TLI between patients with active arthralgias (8.7 (IQR 2.1–31.8)) compared with those with inactive arthralgias (8.7 (IQR 3.5–16.7)), p=0.48 (table 2). Similarly, the ROC curve in figure 1 shows that there was no significant association found between TLI and presence of active arthralgias (AUC=0.53, p=0.16). The rate of active arthralgias by TLI quartile is shown in figure 2. Patients with active arthralgias were not more likely to have detectable ATI when compared with those with inactive arthralgias (OR 1.95, 95% CI 0.92 to 4.11, p=0.08). Compared with patients with IBD in remission, those with active IBD were not more likely to have active arthralgias (OR 1.4, 95% CI 0.79 to 2.44, p=0.25). Patients with active arthralgias had a higher median HBI (3 IQR (1–6)) in comparison with those with inactive arthralgias (1 IQR (0–3)), p=0.0003).

ROC curve showing the association between TLI and active arthralgia. ROC, receiver operating characteristic; TLI, trough levels of inflixima; AUC, area under the curve.
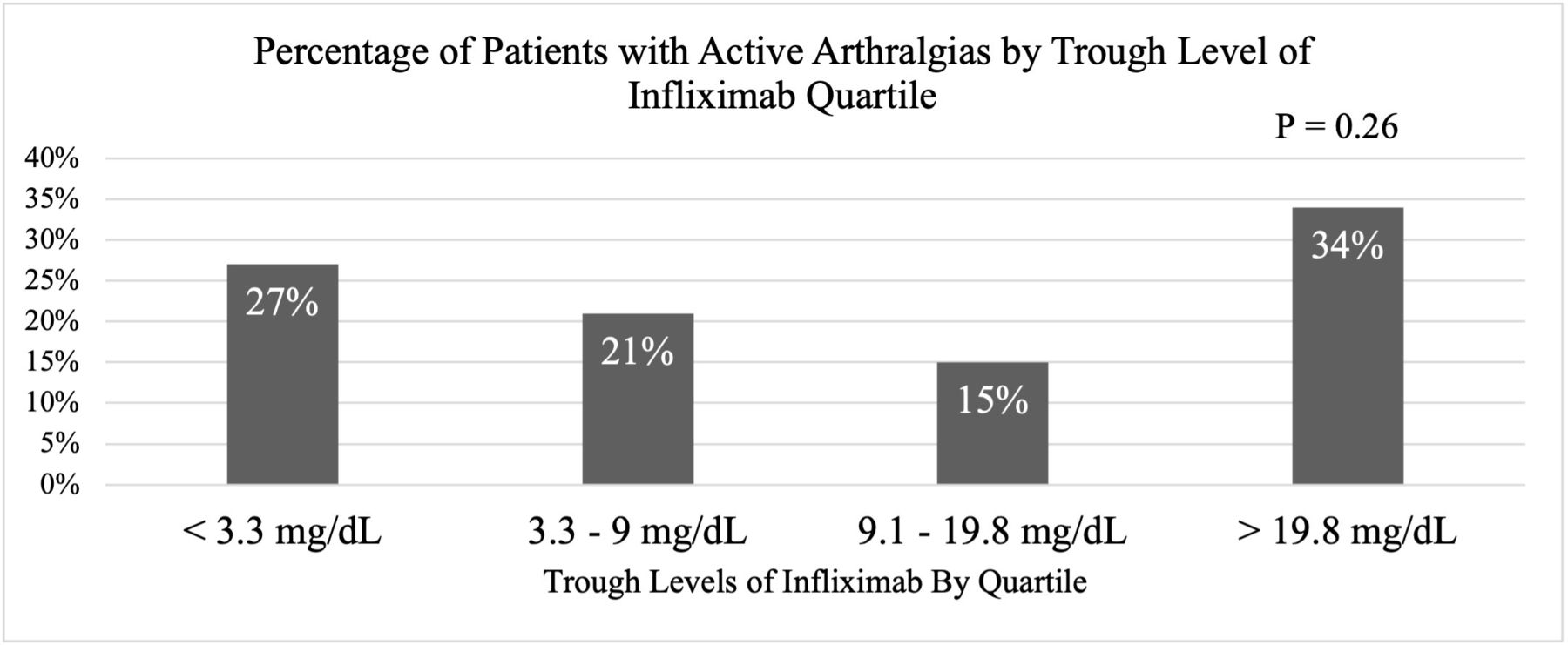
Rate of active arthralgias by quartile of trough level of infliximab.
We also evaluated the association between the use of immunomodulators and active arthralgias. Patients on combination therapy with methotrexate or thiopurines were not more likely to have inactive arthralgias vs those patients on infliximab monotherapy (table 2). Moreover, patients receiving methotrexate were not more likely to report lack of active arthralgias when compared with those on combination therapy with thiopurine or infliximab monotherapy (OR 0.87, 95% CI 0.37 to 2.02, p=0.75).
IBD activity and infliximab pharmacokinetics
Out of the study cohort, 148 patients (55.4%) were in IBD remission. We found no significant difference in age, gender, body mass, IBD phenotype or disease duration between patients with active IBD and those in remission (table 3). The median TLI was significantly lower in patients with active IBD in comparison with those patients in remission (5.7 vs 11.1, p=0.0004, table 3). Those patients with a TLI ≥9 mg/dL were more likely to be in IBD remission when compared with patients with TLI <9 mg/dL (OR 2.1, 95% CI 1.26 to 3.36, p=0.004). A receiving operator curve showing the association between active IBD and TLI is shown in figure 3 (AUC: 0.63, p=0.003). Median TLI was higher in those patients receiving combination therapy in comparison with those on infliximab monotherapy (10.8 vs 6.3, p=0.009); however, these patients on combination therapy were not less likely to have detectable ATI (OR 0.56, 95% CI 00.28 to 1.15, p=0.11). Patients with detectable ATI were significantly more likely to have active IBD (p<0.0001, table 3).
Differences between patients with active IBD and IBD in remission

{kind=link}
{kind=link}
{kind=link}
ROC curve showing the association between TLI and active IBD. IBD, inflammatory bowel disease; ROC, receiver operating characteristic; TLI, trough levels of infliximab.
Discussion
TDM of infliximab has been found to be an effective tool in treatment of IBD. Patients with active disease and low TLI can benefit from dose escalation, while those with active disease and high ATI and/or high TLI are more likely to benefit from switching drug therapies.9 10 Infliximab is known to be an efficacious treatment of EIMs; however, little is known on the use of TDM to guide and optimise treatment in this setting.6 In this study, we aimed to assess the relationship between TLI and peripheral arthralgia activity, one of the most common EIMs of IBD.1 2
While the majority of the patients in our study (72%) had no active peripheral arthralgias on infliximab, we found no association between TLI and presence or absence of peripheral arthralgias. This is an important finding, as treatment of extraintestinal targets may need a different approach when compared with intestinal inflammation. When infliximab is used in the treatment of RA, certain studies have shown that arthralgia response is independent of TLI.11 12 Although the pathophysiology of arthralgias may vary between patients with RA and IBD, it is possible that patients with IBD have a similar heterogeneous response to treatment that is independent of the drug pharmacokinetic. Another explanation is that serum TLI needed to achieve optimal concentrations in target organs may differ. Specifically, the inflammatory burden in the gastrointestinal tract in the setting of UC and CD is higher than in RA, requiring higher drug levels.13 Biological doses required to treat rheumatoid conditions are thus generally lower in RA compared with IBD. For example, standard dosing of infliximab for treatment of RA (3 mg/kg every 8 weeks) is lower than that used in IBD (starting dose of 5 mg/kg every 8 weeks). There is a possibility that the higher doses used for IBD treatment may not confer a dose-dependent response for treatment of peripheral arthralgias.
In a study by Levartovsky et al, researchers found similar results in that peripheral arthralgia activity in their study population did not correlate with TLI.14 One important difference between our studies is that we found no association between arthralgia activity and antibody presence, although there may have been a trend towards significance (OR=1.95, p=0.08). Physiologically, antibody presence has a neutralising effect on infliximab, and thus we expected presence of ATI to impact arthralgia activity. This discrepancy between results could be explained by the relatively low prevalence of detectable ATI in our study population (13.5%), a difference in ratio of type 1 to type 2 arthralgias, or differences in the assays used. We do have to note that one-third of the patients in this study had ELISA testing done and had detectable TLI, hence ATIs could not be measured in these patients.
Our study does differ from the literature in that in our cohort, peripheral arthralgia activity did not correlate with overall IBD activity. Certain studies show that the majority of peripheral arthralgia activity follows overall disease activity. It is possible that our study population had a larger prevalence of type II arthropathy (polyarticular), which unlike type I arthropathy (pauciarticular), does not follow disease activity. Another potential explanation for this lies within our classification of active IBD, defined as an elevated CRP in conjunction with abnormal indices of clinical disease activity (HBI and PMS), as these indices contain subjective and patient-reported data. True correlation of peripheral arthralgia activity and luminal activity would need to be performed by endoscopic evaluation as symptoms and even biomarkers (such as CRP) do not always correlate with endoscopic disease activity, especially in CD.15 16
An interesting finding in our study was the association of active arthralgias and SIBDQ scores. Our results showed significantly higher quality of life in patients with inactive peripheral arthralgias in comparison with patients with active arthralgias. Although patients may not have gastrointestinal symptoms from their IBD, IBD-related arthralgias can limit daily activity and affect quality of life. Given the high prevalence of peripheral arthralgias, in 5%–10% of patients with UC and 10%–20% in patients with CD, the relationship between arthralgia activity and quality of life further highlights the importance of EIM treatment optimisation.17 18
The strengths of this study include a large sample size and a greater percentage of patients with CD than UC, thus proving representative of the overall IBD population with peripheral arthralgias. Furthermore, we excluded patients on medications that could have masked arthritic symptoms. Our study does have inherent limitations of a retrospective single-centre study. Selection bias, however, was somewhat minimised in that documentation of presence or absence of EIMs, as well as activity of these EIMs is a standard, templated part of our documentation. Furthermore, TLI/ATI were measured using two different assays and the ELISA is not able to measure ATI in the presence of drug. Other limitations related to the nature of this retrospective study include lack of further objective data regarding arthralgia activity, limiting our ability to delineate arthralgia severity, characterise the inflammatory nature of the arthritis, and distinguish between type I and type II arthropathy. Additionally, although arthralgia documentation was obtained in an IBD-specific clinic, the gastroenterologists documenting arthralgia activity may lack advanced training in joint assessment possibly further limiting our study. Future studies delineating between the two types of arthralgias may show differing results, as type I arthropathy follow disease activity and may be impacted by TLI as opposed to type II arthropathy.
In conclusion, although TDM has a role in the management of CD and UC, its use in the management of the peripheral arthralgias associated with IBD may be limited.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study protocol was approved by the Medical College of Wisconsin Institutional Review Board (IRB #PRO00036230).
Acknowledgments
Abstract has been presented at Digestive Diseases Week 2021 as a virtual poster presentation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors had final approval of submitted version. SS: acquisition of data, analysis and interpretation of data, drafting of manuscript, critical revision. BR: acquisition of data, critical revision. AM: acquisition of data, critical revision. PB-P: interpretation of data, critical revision. AB: acquisition of data, critical revision. DJS: interpretation of data, critical revision. AJY: study conception and design, analysis and interpretation of data, drafting of manuscript and critical revision
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests DJS: Has speaker honorariums from Abbvie, Takeda, Pfizer and Jansen. AJY: Member of advisory boards for Takeda, Bristol Myers Squibb, Prometheus Laboratories and Arena Pharmaceuticals
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.