Article Text

Abstract
Objective A minimum of physical activity and low liquid intake are factors that have been associated with constipation. The health emergency brought on by the COVID-19 pandemic has resulted in adopting behaviour, such as sheltering-in-place (less mobility) and dietary changes, creating a scenario we believe to be an adequate model for examining the appearance of symptoms of constipation and its associated factors.
Design A cross-sectional and descriptive study was conducted on an open population, applying an electronic survey (4 weeks after lockdown due to COVID-19 in Mexico) to evaluate demographic characteristics, physical activity, water and fibre intake, appearance of constipation symptoms (including stool consistency), and quality of life.
Results Out of 678 subjects evaluated, 170 (25%, 95% CI: 21.7 to 28.4) developed symptoms of ‘new-onset’ constipation, with a significant decrease in the number of daily bowel movements (p<0.05) and stool consistency (p<0.05) during lockdown. Furthermore, in the ‘new-onset’ constipation population there was a higher proportion of subjects (79 (47%) of 170) who stopped exercising during the pandemic compared with the subjects who did not develop constipation symptoms (187 (37%) of 508, p=0.03, OR: 1.49, 95% CI: 1.0 to 2.1). The multivariate analysis (logistic regression) showed that female sex (p=0.001), water intake (p=0.039), and physical activity (p=0.012) were associated with ‘new-onset’ constipation.
Conclusions In our study on an open population in Mexico, we found that one-fourth of the population developed ‘new-onset’ constipation symptoms during the lockdown imposed due to the COVID-19 pandemic. A reduction of physical activity and less water consumption were associated factors.
- constipation
- dietary fibre
- COVID-19
Data availability statement
Data are available upon reasonable request. Data are available upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known about this subject?
A minimum of physical activity and low liquid intake are factors that have been associated with constipation.
The health emergency brought on by the COVID-19 pandemic has resulted in adopting behaviour and dietary changes, creating a scenario we believe to be an adequate model for examining the appearance of symptoms of constipation and its associated factors.
What are the new findings?
We found that one-fourth of the population developed ‘new-onset’ constipation symptoms during the lockdown imposed due to the COVID-19 pandemic. A reduction of physical activity and less water consumption were associated factors.
How might it impact on clinical practice in the foreseeable future?
Given those results, appropriate physical activity, and adequate liquid intake during prolonged periods of lockdown should be recommended to prevent the said symptoms.
Introduction
Constipation is one of the most frequent gastrointestinal disorders and is estimated to affect up to 14% of the general population.1–4 The pathophysiology of constipation is complex and multifactorial.1 5 6 Among the factors that contribute to the appearance or worsening of constipation symptoms are those that are considered unmodifiable, such as female sex, advanced age, and the association with different comorbidities, such as neurologic diseases.7 On the other hand, there are numerous factors, associated with lifestyle, that are considered modifiable, such as low fibre intake,8 9 inadequate water intake,10–12 sedentary lifestyle, medication use, and reduced physical activity.12 13 Nevertheless, evidence on the theme is limited and controversial, given the difficulty in conducting prospective studies on the topic. Some studies have demonstrated that physical activity has no effect on the motor activity of the colon, whereas others report the opposite, showing it can depend on the frequency, intensity and duration of exercise (for example, marathon running).11 13 14 Symptoms of constipation induced by immobility in geriatric patients have been shown to decrease with the regular performance of physical activity. In a unique study on the subject, Iovino et al15 demonstrated that prolonged physical inactivity (for 35 days, in 10 healthy volunteers) triggered constipation in 60% of the study individuals.
The COVID-19 pandemic, caused by the SARS-CoV-2 coronavirus and declared in March 2019 by the WHO, has resulted in an unprecedented public health crisis worldwide.16 This health emergency has produced substantial changes in social, economic and cultural spheres. In Mexico, contingency measures (reduced essential activity, physical distancing, stay-at-home orders, etc) were established on 21 April 2020. Evidence suggests that the obligatory social self-isolation impacts the lifestyle of the population, forcing the adoption of unhealthy dietary habits (increased ultra-processed and refined foods and decreased fruit and vegetable intake), sedentary behaviour and sleep disturbances.17
Recent studies have shown that the COVID-19 pandemic negatively affected subjects suffering from functional digestive disorders such as irritable bowel syndrome (IBS).18–21 For example, Kamp et al18 reported that during the COVID-19 pandemic up to 50% of patients with IBS reported increases in abdominal pain (48%), diarrhoea (45%) or constipation (44%). Another study from France found that stress linked to the COVID-19 pandemic and confinement is high and equivalent in both IBS and non-IBS participants, with higher psychological and quality of life (QOL) consequences in patients with IBS who have altered coping capacities.20 However, the effect of confinement due to the COVID-19 pandemic specifically on the possibility of inducing symptoms of constipation in the general population is unknown. Thus, the primary aim of our study was to evaluate the incidence of symptoms of constipation during the lockdown implemented to contain the spread of COVID-19 in Mexico. The secondary aims of the study were to evaluate the clinical characteristics of the patients who developed ‘new-onset’ constipation and the factors associated with this condition (physical activity, water and fibre consumption).
Methods
Study design and population
A descriptive, cross-sectional study was conducted on an adult Mexican population (above 18 years of age), in which volunteers were asked to take a survey that was distributed on social media throughout Mexico. The survey was designed and applied utilising the ‘Google Forms’ tool (online supplemental material) . Because the lockdown (phase III of the pandemic) was put in place in Mexico on 21 April 2020, the survey became available on 18 May 2020 (4 weeks later) through social media platforms such as Facebook advertisements, Twitter, and WhatsApp. An invitation to fill anonymously an online questionnaire was sent by mail in accordance with general data protection regulations and with the Mexican Federal Law on Protection of Personal Data. Privacy of subject information was ensured by password-protected access to the data collection forms, the online response database did not contain any information that could reveal the identity of individual subjects, and was stored on a secured internet server. No compensation was given for participation in the study.
Supplemental material
Data collection
The following data were collected in the survey applied to each of the participants:
Sociodemographic characteristics: sex, age, weight, height, body mass index, educational level, comorbidities, and medication use.
Physical activity before and after the lockdown: physical activity was measured based on the questions used in the International Physical Activity Questionnaire-Short Form.22 Physical activity frequency (days per week), type, intensity (1=zero, 2=mild (walking, jogging), 3=moderate (riding a bicycle, using a treadmill, etc), and 4=intense (CrossFit, aerobics, working out at a gym, etc)), and duration (<30 min per day, 30–60 min per day, 61–90 min per day, 91–120 min per day, and more than 120 min per day) were recorded.
Water and fibre intake before and after the lockdown: water intake was evaluated according to the four following categories: (1) <500 mL per day, (2) 500 mL to 1 L per day, (3) 1–2.5 L per day, and (4) >2.5 L per day (n, %). Regarding fibre, the participant was asked if intake was on a regular basis and in what form it was consumed (cereals, fruits and vegetables, supplements in capsules, supplements in powder).
Constipation symptoms, stool consistency and bowel movement frequency before and after the lockdown: the participants were asked in binary form (yes or no) if they considered themselves to have constipation before the lockdown. The participants with prior symptoms of constipation were excluded. Those that answered that they had not previously presented with constipation were asked, ‘Do you think you have developed constipation symptoms since the lockdown was put in place?’ If the subjects answered ‘yes’ to this question then they were considered to have a ‘new-onset’ constipation. In addition, based on the questions for defining chronic constipation from the Rome IV Modular Questionnaire, the following symptoms were evaluated: straining, pushing force needed to defecate, stool consistency types 1 and 2, according to the Bristol Stool Form Scale, in more than 25% of the bowel movements, and use of digital manoeuvres. The participants were also asked the number of bowel movements they had per day and per week, and the average stool consistency, according to the Bristol Scale, in the past week.
Quality of life in relation to constipation: the Patient Assessment of Constipation-Quality of Life (PAC-QOL) Questionnaire was used because it is the most widely validated, specific tool for measuring QOL in patients with constipation.23 It has been validated and used in Spanish24 and consists of 28 items grouped into the following subscales: (1) physical discomfort, (2) psychosocial discomfort, (3) worries and concerns, and (4) treatment satisfaction, and includes an overall score. Scoring is on a Likert Scale of 5 points, from 0 (nothing/never) to 4 (extremely, always), and a lower score reflects a better QOL.
Statistical analysis
Incidence (new cases) of constipation after the lockdown (‘new-onset’ constipation) was calculated and the 95% CI was reported. A comparative analysis of the categorical variables and continuous variables was carried out between the participants with ‘new-onset’ constipation and those with no constipation during the lockdown, utilising the Student’s t test, the Mann-Whitney U test, the χ2 test, or the Wilcoxon test, as appropriate. Statistical significance was set at p<0.05. A multivariate analysis was then performed utilising logistic regression, employing the enter model. The analysis of the results was carried out through descriptive statistics with the IBM SPSS Statistics V.22 program. The protocol followed the Declaration of Helsinki stipulations for biomedical research and was approved by the institutional committee (IIMB-2020-008).
Results
General population characteristics
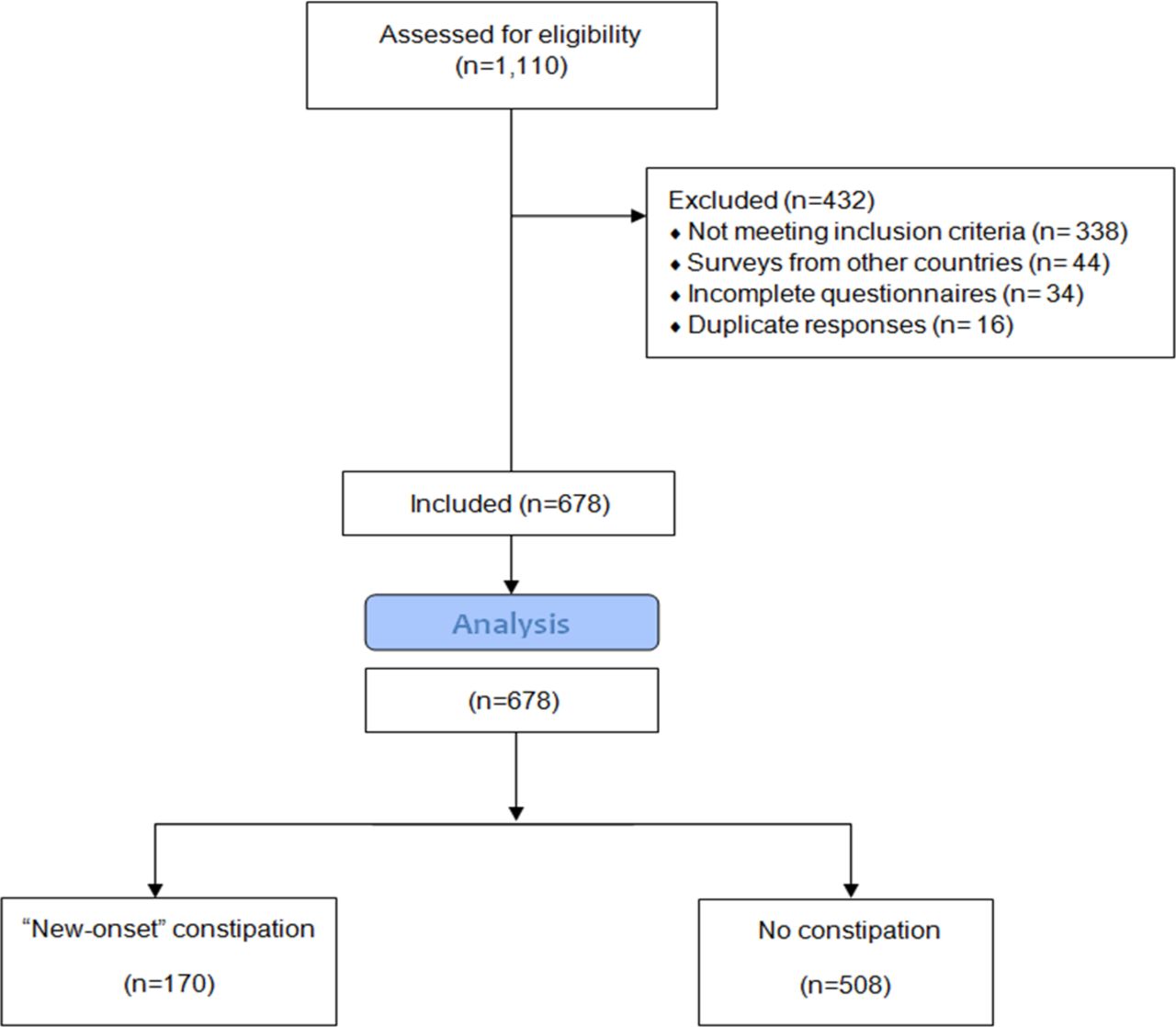
A total of 1110 questionnaires were received (figure 1), 338 were excluded because subject had a previous diagnosis of chronic constipation and 94 were excluded for other reasons (survey takers were from countries other than Mexico, surveys were incompletely filled out or duplicated), leaving 678 study participants. Of those subjects, 405 (59.7%) were women, and the mean participant age was 31.21±11. 9 years (range: 18–74).

Flow diagram.
‘New-onset’ constipation symptoms presenting during the lockdown
One hundred seventy (25%, 95% CI: 21.7 to 28.4) subjects reported having symptoms of constipation that appeared during the lockdown. The symptoms associated with constipation in those subjects were hard stools in more than 25% of bowel movements in 131 (77%) participants, sensation of incomplete defecation in 122 (72%) participants, sensation of straining in 114 (67%) participants and use of digital manoeuvres in 6 (3.5%) participants. The average stool consistency reported in the past week, according to the Bristol Scale, was: type 1 in 20% (n=34), type 2 in 22% (n=38), type 3 in 22% (n=37), type 4 in 21% (n=36), type 5 in 9% (n=15), type 6 in 5% (n=8), and type 7 in 1.2% (n=2).
In those subjects, the median of bowel movements per day decreased from 2 (range: 1–6) to 1 (range: 1–6) after the lockdown (p=0.00001). Likewise, the median of bowel movements per week decreased from 9 (range: 3–35) to 7 (range: 1–28) after the lockdown (figure 2). The median of stool consistency, according to the Bristol Scale, decreased from 4 (range: 1–7) to 3 (range: 1–6) after the lockdown (p=0.0001). In contrast, in the subjects who did not develop constipation, there was no difference in the number of bowel movements per day (median: 2 (range: 1–7) vs 2 (range: 1–10), p=0.464), in the number of bowel movements per week (median: 12 (range: 1–42) vs 10 (range: 1–56), p=0.225), or in stool consistency (median: 4 (range: 1–7) vs 4 (range: 1–6), p=0.58).
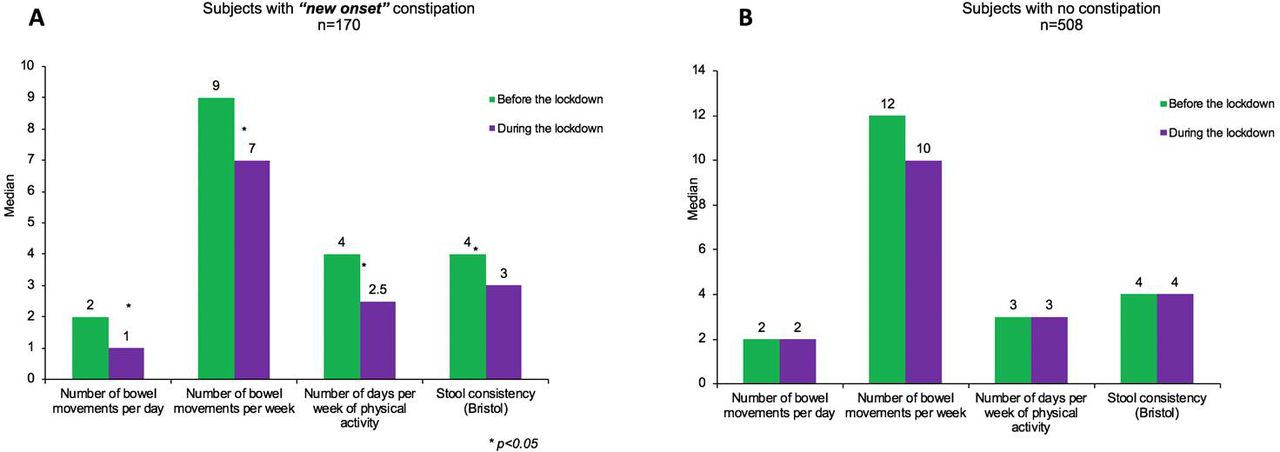
Number of bowel movements, days of physical activity and stool consistency before and after the lockdown.
Regarding physical activity, the subjects who developed ‘new-onset’ constipation, significantly reduced the number of days that they did exercise during the lockdown (median: 4 (range: 1–7) vs 2.5 (range: 0–7), p=0.004) (figure 2). In contrast, there was no difference in the number of days doing exercise during the lockdown in the subjects that did not present with constipation (median: 3 (range: 0–7) vs 3 (range: 0–7), p=0.669).
Factors associated with ‘new-onset’ constipation before the lockdown
Table 1 shows the baseline characteristics and associated factors (before the lockdown) in the 170 subjects with ‘new-onset’ constipation and the 508 subjects who had no constipation symptoms. A significantly higher percentage of women than men developed ‘new-onset’ constipation (p=0.0001). The presence of comorbidities, water and fibre intake, physical activity, number of bowel movements, and Bristol Scale-assessed stool consistency were similar between the two groups before the lockdown.
Demographic characteristics, bowel movements and risk factors before the lockdown in ‘new-onset constipation’ and subjects without constipation
Factors associated with ‘new-onset’ constipation during the lockdown
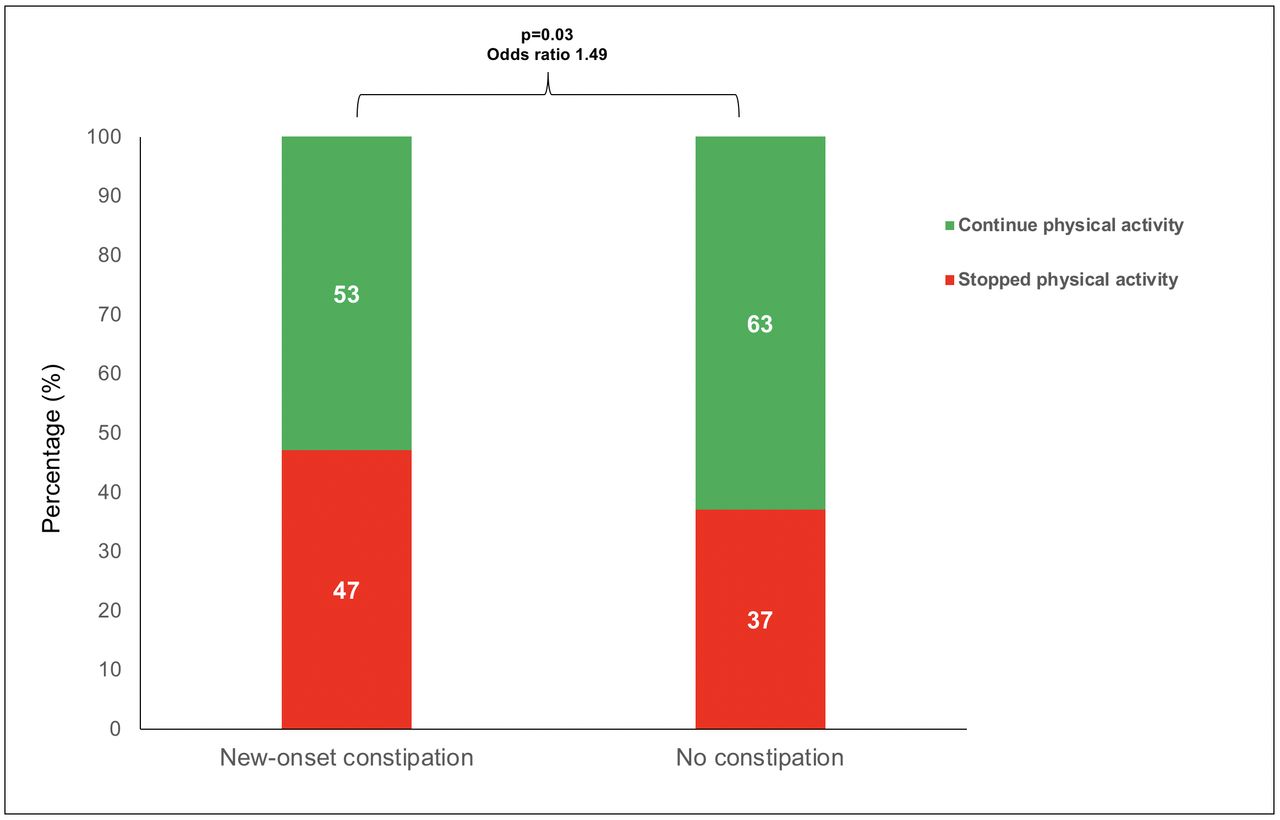
Table 2 shows the associated factors to ‘new-onset’ constipation during the lockdown. According to the univariate analysis, in the ‘new-onset’ constipation population there was a higher proportion of subjects (79 (47%) of 170) who stopped exercising during the pandemic compared with the subjects who did not develop constipation symptoms (187 (37%) of 508, p=0.03, OR: 1.49, 95% CI: 1.0 to 2.1) (figure 3). A higher proportion of subjects with ‘new-onset’ constipation drank <1 L of water per day (30% vs 18%, p=0.001, OR: 2.5, 95% CI: 0.4 to 12.8). No differences were found in the duration or number of days of physical activity or in fibre intake during the lockdown between the two groups (table 2). In the multivariate analysis (logistic regression), female sex, water intake, and physical activity were associated with the development of ‘new-onset’ constipation (table 3).

{kind=link}
{kind=link}
{kind=link}
Percentage of subjects who stopped physical activity during the pandemic among groups.
Risk factors and bowel movement characteristics during the lockdown among ‘new-onset constipation’ and subjects without constipation
Logistic regression model
QOL according to the PAC-QOL Questionnaire
According to the PAC-QOL, the mean score for the physical discomfort subscale was 2.16±0.72, for the psychosocial subscale was 1.74±0.6, for the worries and concerns subscale was 2.98±0.8, for the satisfaction subscale was 3.46±0.9, and for the overall score was 2.3±0.6.
Discussion
The lockdown and mobility restriction measures put in place to contain the spread of COVID-19 created a ‘natural’ model to explore the role of some modifiable factors (such as water and fibre intake, physical activity) that have traditionally been associated with constipation. In our study, we found that up to 25% of the population that had to be in confinement due to the COVID-19 pandemic developed ‘new-onset’ constipation and reduced physical activity and lower water consumption were associated factors. Among subjects whom develop ‘new-onset’ constipation, there was a significant decrease in the number of bowel movements, as well as significantly harder stools during the lockdown. The fact that we found an increased occurrence of harder stools (using the Bristol Scale) suggests that colon transit time was slower in those subjects during the lockdown. Although a decrease in two bowel movements per week (9–7) or a decrease in one point in the Bristol Stool Form (4–3) may seem irrelevant, the perception of this by subjects with constipation is clinically relevant. For example, in previous studies it has been described that up to 50% of the patients defined constipation differently from accepted medical definitions (27% of the patients defined it as defecation every 2 days or less and 25% as hard stool alone).25
The role of mobility and physical activity in relation to chronic constipation is a subject of debate,12 13 but our study showed that reduced physical activity was an associated factor for the appearance of constipation symptoms. Some studies have reported that prolonged immobilisation is a trigger for the appearance of symptoms of constipation.26 27 Even though those findings have been described in chronically ill patients, little is known about reduced mobility and the appearance of constipation in a population that previously was apparently healthy, such as the one we evaluated. Our results are similar to those reported by Iovino et al,15 in a ‘new-onset’ constipation model. Those authors demonstrated that strict bed rest for a period of 35 days, adhered to even perform daily activities, including defecation, was associated with a high rate of constipation in healthy volunteers.
There is no doubt that exercise and physical activity have a beneficial impact on the physiology of the colon. Both have been shown to accelerate gastrointestinal transit,28 29 increase colon motility, and even produce favourable hormonal changes, thus preventing constipation.10 30 Nevertheless, it is important to recognise that there are other determining factors, such as the type and intensity of physical activity, as well as water and fibre intake. In that context, we found that 18% of the subjects with ‘new-onset’ constipation stopped doing exercise during the lockdown (65% before vs 47% after), whereas the rest of the subjects with constipation symptoms that did do exercise, reduced the frequency and intensity of their physical activity.
Another interesting finding of our study was that a significant number of subjects who developed constipation drank <1 L of water per day. That result was similarly described in a population study conducted in the USA by Markland et al.12 They reported that low liquid intake (<1882 mL per day) was a predictor for constipation in women (prevalence odds ratio (POR): 1.3, 95% CI: 1.0 to 1.6) and men (POR: 2.4, 95% CI: 1.5 to 3.9). The mechanisms by which appropriate liquid intake positively influences colon transit are variable and include a better general hydration status and it can potentiate the effect of fibre and reduce its secondary effects.31–33 With respect to fibre, as in other studies,12 we found no relation between fibre intake and the appearance of ‘new-onset’ constipation symptoms.
Currently, the PAC-QOL Questionnaire is the most validated and the most specific tool for measuring the QOL of patients with constipation. In our study, subjects who developed ‘new-onset’ constipation, had higher scores on the satisfaction and worries and concerns subscales (3.46±0.9 and 2.98±0.8, respectively), which suggest that even in the short span of symptom progression, constipation is a condition that impairs QOL. PAC-QOL was developed to measure the health-related QOL of patients with constipation as a secondary objective in Prucalopride evaluation randomized control trials (RCTs), so there are no normal values in healthy controls. However, the mean value of the PAC-QOL overall score in our population is comparable to that reported by Tack et al34 in patients with functional chronic constipation (2.3 and 2.1, respectively).
Even though ours is a novel study with relevant findings, it also has limitations. The appearance of ‘new-onset’ constipation symptoms does not necessarily imply that they will persist chronically and classified as chronic constipation according to Rome IV criteria, and in some subjects, the symptoms will probably disappear once their pre-lockdown physical activity and habits are re-established. Our study also was focused primarily on evaluating constipation symptoms, without taking abdominal pain into account, making it likely that some of our subjects had IBS-C (irritable bowel syndrome with constipation). It is important to acknowledge that both Rome IV criteria for chronic constipation and 'new-onset' constipation, suffer from recall bias. A prospective stool diary would have helped reduce the possibility of this bias. We also do not ask specifically about previous underlying bowel disorder, functional gastrointestinal disorders, stress level or psychological factors. With respect to the tools utilised, the quantity of water was evaluated through an arbitrarily created Likert Scale, considering that normal water intake should be at least 1 L per day. Another limitation is that we assessed water intake only as opposed to fluid intake. Likewise, the null association between fibre intake and constipation was related to the fact that we did not employ a specific questionnaire for its appropriate evaluation. Both water and fibre consumption evaluation also suffer from recall bias. A limitation related to the data collection was that 12% of responses were excluded due to incomplete answers for a particular question or duplicate information. Although multiple social media platforms were used it is very difficult to estimate how many individuals viewed the advert to recruit to this study but chose not to. A further limitation of this study is access to smartphones and the literacy of the study population (required by the pandemic) may have influenced the results. Also, our evaluated population is young and the results may not be applicable to everyone. Finally, psychological comorbidities were not accounted for as these have been shown to have increased during COVID-19 and may have acted as confounders.
In conclusion, in our study on an open population in Mexico, we found that one-fourth of the population developed ‘new-onset’ constipation symptoms during the lockdown imposed due to the COVID-19 pandemic. A reduction of physical activity and less water consumption were associated factors. Given those results, appropriate physical activity and adequate liquid intake during prolonged periods of lockdown should be recommended to prevent said symptoms.
Data availability statement
Data are available upon reasonable request. Data are available upon request.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @chemaremes, @BryanPriegoP
Contributors JMR-T is the guarantor of the article. JMR-T and CD-R wrote the paper. JMR-T, EC-A and MA-B designed the research study and analysed the data. CD-R, BAP-P, SMMP-G and ATR performed the research tools and electronic platform. EC-A, MA-B, PCG-C, JAV-RV, RF-R, OG-E and MCR-L collected the data.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests JMR-T is a member of the advisory board of Takeda, Asofarma and Biocodex. He has been a speaker for Takeda, Asofarma, Medtronic, Carnot and Alfasigma. EC-A has been a speaker for Takeda, Asofarma, Medtronic, Carnot and Grünenthal. MA-B has been a speaker for Takeda and Asofarma. JAV-RV, PCG-C, RF-R, OG-E, MCR-L, CD-R, SMMP-G, BAP-P and ATR have no conflicts of interest.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.