Article Text

Abstract
Objective Colonoscopy withdrawal time (CWT) is a key performance indicator affecting polyp detection rate (PDR) and adenoma detection rate (ADR). However, studies have shown wide variation in CWT and ADR between different endoscopists. The National Endoscopy Database (NED) was implemented to enable quality assurance in all endoscopy units across the UK and also to reduce variation in practice. We aimed to assess whether CWT changed since the introduction of NED and whether CWT affected PDR.
Methods We used NED to retrospectively collect data regarding CWT and PDR of 25 endoscopists who performed (n=4459 colonoscopies) in the four quarters of 2019. We then compared this data to their performance in 2016, before using NED (n=4324 colonoscopies).
Results Mean CWT increased from 7.66 min in 2016 to 9.25 min in 2019 (p=0.0001). Mean PDR in the two periods was 29.9% and 28.3% (p=0.64). 72% of endoscopists (18/25) had CWT>6 min in 2016 versus 100% (25/25) in 2019, the longer CWT in 2019 positively correlated with the PDR (r=0.50, p=0.01). Gastroenterology consultants and trainee endoscopists had longer CWT compared with colorectal surgeons both before and after using NED.
Conclusion NED usage increased withdrawal times in colonoscopy. Longer withdrawal times were associated with higher PDR. A national colonoscopy audit using data from NED is required to evaluate whether wide variations in practice across endoscopy units in the UK still exist and to ensure minimum colonoscopy quality standards are achieved.
- colonoscopy
- colorectal adenomas
- colorectal cancer
- colorectal cancer screening
Data availability statement
Data are available upon reasonable request. Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known about this subject?
High-quality colonoscopy prevents colorectal cancer and reduces mortality, but wide variations in key quality indicators (KPIs), such as colonoscopy withdrawal time and adenoma detection rate, exist between different endoscopists.
The National Endoscopy Database (NED) collects data from all participating endoscopy units to ensure high-quality service and minimise variations in practice.
What are the new findings?
NED usage increased withdrawal times in colonoscopy and longer withdrawal times were associated with higher polyp detection rate.
Variations in practice exist between endoscopists according to their specialty and level of training.
How might it impact on clinical practice in the foreseeable future?
NED offers endoscopists the opportunity to monitor and audit their own KPIs, which seems to be the most effective way of improving colonoscopy practice.
The next national colonoscopy audit should use data from NED including colonoscopy withdrawal times to ensure quality across UK endoscopy units.
Introduction
Incidence and mortality rates of colorectal cancer (CRC) in western countries have been falling over the last decade since the introduction of national screening programmes.1–4 However, CRC remains the second cause of cancer-related deaths in the UK.1 Colonoscopy is an effective and safe screening tool5 that has been shown to prevent CRC and reduce mortality.2 5–7
The demand for colonoscopy has significantly increased in England, with over 360 000 procedures performed each year.8 Recent studies have shown wide variations in colonoscopy quality between different endoscopists and across institutions.9–13 Suboptimal colonoscopy practice has been associated with an increased risk of postcolonoscopy CRC.14 Therefore, current UK guidelines have set clear standards for a minimum acceptable colonoscopy withdrawal time (CWT) of 6 min to achieve adenoma detection rate (ADR) of at least 15% with an aspiration to reach a CWT of 10 min and ADR of 20%. These quality standards aim to guarantee delivering high-quality colonoscopy as well as minimising variations between different units across the country.6
CWT, which is the time spent cautiously inspecting the colonic folds while withdrawing the scope, is a key performance indicator (KPI) in colonoscopy. Longer CWT has been shown to increase polyp detection rate (PDR)/ADR in both screening15–21 and non-screening colonoscopies.9
Various studies have investigated the minimum CWT to achieve acceptable PDR/ADR.9 11 17 22 23 In their landmark study, Barclay et al11 found a significant difference in PDR/ADR between endoscopists with a withdrawal time longer than 6 min and those with less than 6 min. Patel et al21 suggested that a minimum withdrawal time of 11 min resulted not only in higher ADR but also in increased detection of proximal serrated polyps, which were found to be the most missed lesions in the polyp prevention trial.24 This correlation between CWT and ADR is significant, given the inverse relationship between ADR and interval CRC.25 In one study, each 1% increase in ADR led to a 3% reduction in the risk of cancer.26
In 2013, the National Endoscopy Database (NED) was launched to create a central online database collecting data from all endoscopy units across the UK to ensure high-quality service as well as facilitating nationwide large-scale audits and research.27 Moreover, auditing national endoscopy services through NED should reduce variations in practice to a bare minimum.
We aimed to assess whether using NED has led to longer CWT. Also, we wanted to know if there were differences in CWT and PDR according to endoscopists specialty and whether CWT correlated to PDR.
Methods
We retrospectively reviewed and included data of all diagnostic non-screening colonoscopies performed at Sheffield Teaching Hospitals from January to December 2016. Electronic Document and Records Management System (EDMS) and Infoflex V.5 software were used to retrieve the following data: the endoscopist’s details, the indication of the procedure, the time of caecal intubation and rectal retroflexion and the presence of polyps.
In our centre, we started uploading all endoscopy data to NED from April 2018. In order to evaluate the impact of NED on endoscopists performance, we collected data regarding CWT and ADR on all diagnostic colonoscopies performed at Sheffield Teaching Hospitals from January to December 2019. All data were retrieved directly from NED system.
We included all diagnostic colonoscopies performed by the same endoscopists (n=25) in 2016 and 2019. The included endoscopists were divided according to their specialty and level of training into three groups: group A—colorectal surgeons; group B—consultant gastroenterologists; group C—trainee endoscopists including medical/surgical trainees and a nurse endoscopist. These trainees were perfoming independently (signed off for colonoscopies).
For colonoscopies performed in 2016, we calculated CWT using the documented times of caecal intubation and rectal retroflexion images on EDMS. CWT for colonoscopies performed in 2019 was retrieved directly from NED.
In 2016, we excluded withdrawal time measurements in procedures with poor preparation, diathermy usage, with multiple cold polypectomies as these may spuriously increase the withdrawal time. However, the data for PDR was derived from all the procedures done by endoscopists. As the KPIs for 2019 were derived from NED, there was not any exclusion criteria as this information is not currently captured by NED.
All colonoscopies were performed using the Olympus Colonoscope (CF-H290L/I) either under conscious sedation or without sedation.
All endoscopists were made aware, by the endoscopy operational team, that NED upload was commencing and that individual data were monitored. The endoscopy clinical lead monitored regular data input to NED.
Ethical approval was not required as this study was a service evaluation. The study was approved at the local endoscopy user meeting.
Statistical analysis
Student t test and Mann-Whitney U test were used to compare the differences in CWT and ADR between 2016 and 2019. One-way analysis of variance with Bonferroni post hoc test was used to compare different groups of endoscopists. Pearson correlation test was used to assess the relationship between the CWT and PDR. A two-tailed p value of <0.05 was considered significant. GraphPad Prism V.8.2.1 for Windows (GraphPad Software, La Jolla, California, USA) was used to conduct statistical analysis.
Results
Twenty-five endoscopists performed a total of 8783 colonoscopies in the two study periods (table 1). Group A endoscopists (n=9) performed 1865 colonoscopies in 2016 and 1887 colonoscopies in 2019, group B endoscopists (n=9) performed 1478 colonoscopies in 2016 and 1293 colonoscopies in 2019, group C endoscopists (n=7) performed 981 colonoscopies in 2016 and 1279 colonoscopies in 2019.
Comparison of the number of colonoscopies, mean CWT and PDR in 2016 and 2019 for each endoscopist
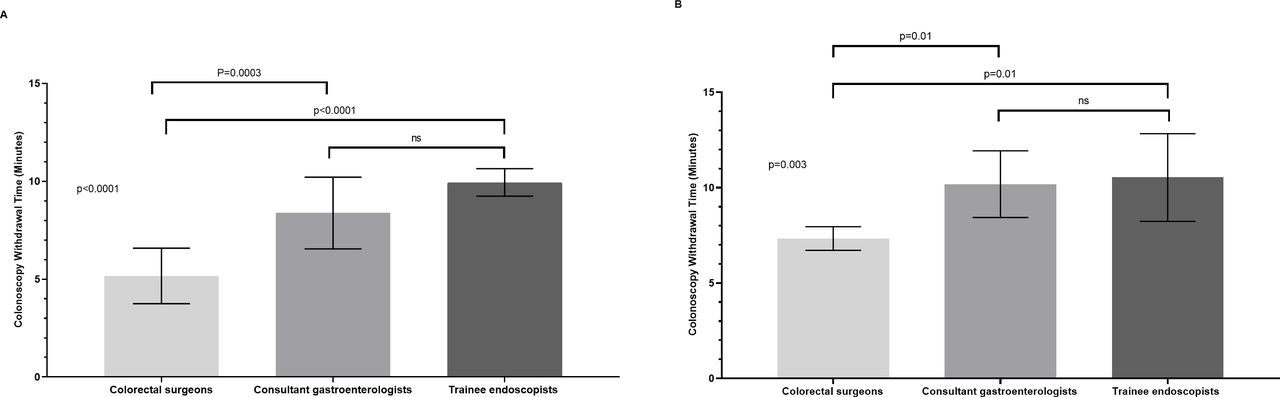
CWT ranged between 3 and 11.2 min (mean 7.66 SD 2.44) min) in 2016 compared with 6.18–12.4 min (mean 9.25 (SD 2.16) min) in 2019 (p=0.0001) as shown in figure 1. CWT was significantly longer in colonoscopies performed by group B and group C compared with group A in 2016 (p<0.0001) and 2019 (p=0.003) (figure 2).
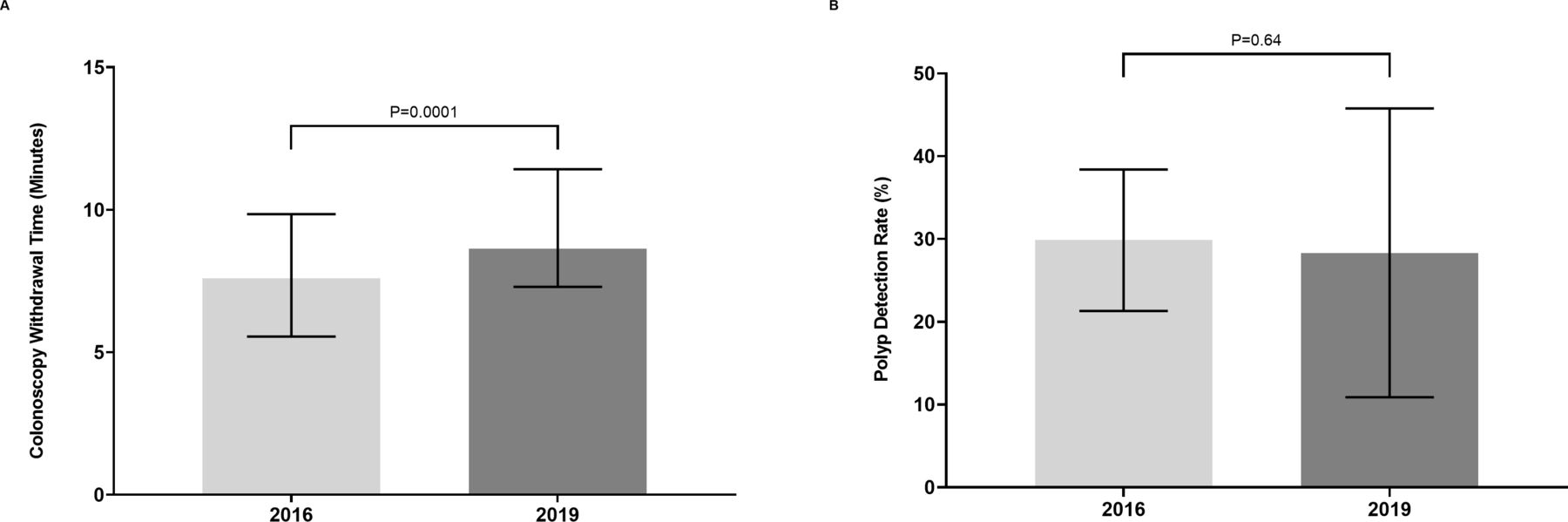
Differences between (A) colonoscopy withdrawal time in 2016 and 2019 and (B) polyp detection rate in 2016 and 2019.
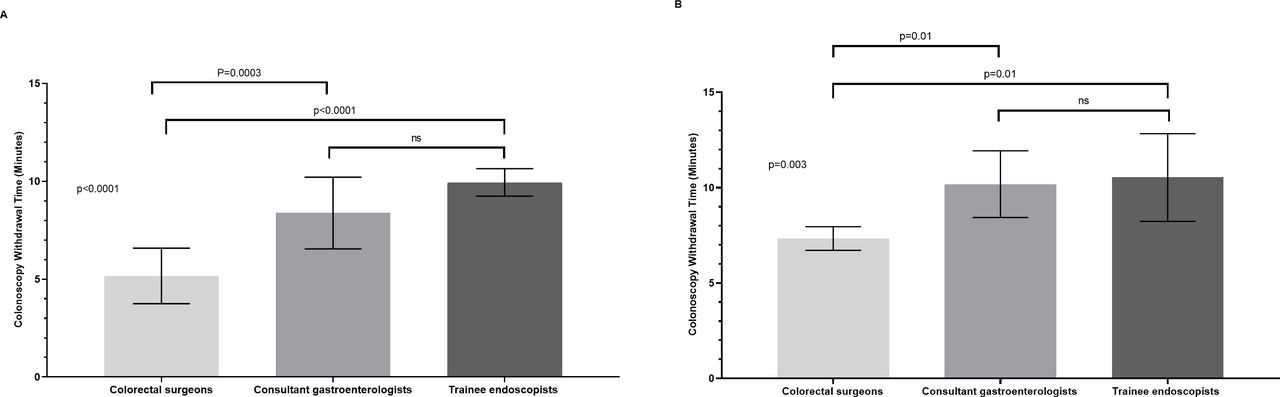
Comparison of colonoscopy withdrawal time between the three groups of endoscopists in (A) 2016 and (B) 2019.
Seventy-two per cent of endoscopists (n=18/25) had CWT >6 min in 2016 compared with 100% (n=25/25) in 2019; differences in CWT between 2016 and 2019 were significant in group A (mean CWT 5.16 vs 7.33 min, p=0.0004) and group B (mean CWT 8.37 vs 10.18 min, p=0.02) but not in group C (mean CWT 9.94 vs 10.5 min, p=0.37) (figure 3).

Comparison of colonoscopy withdrawal time in 2016 and 2019 between individual groups.
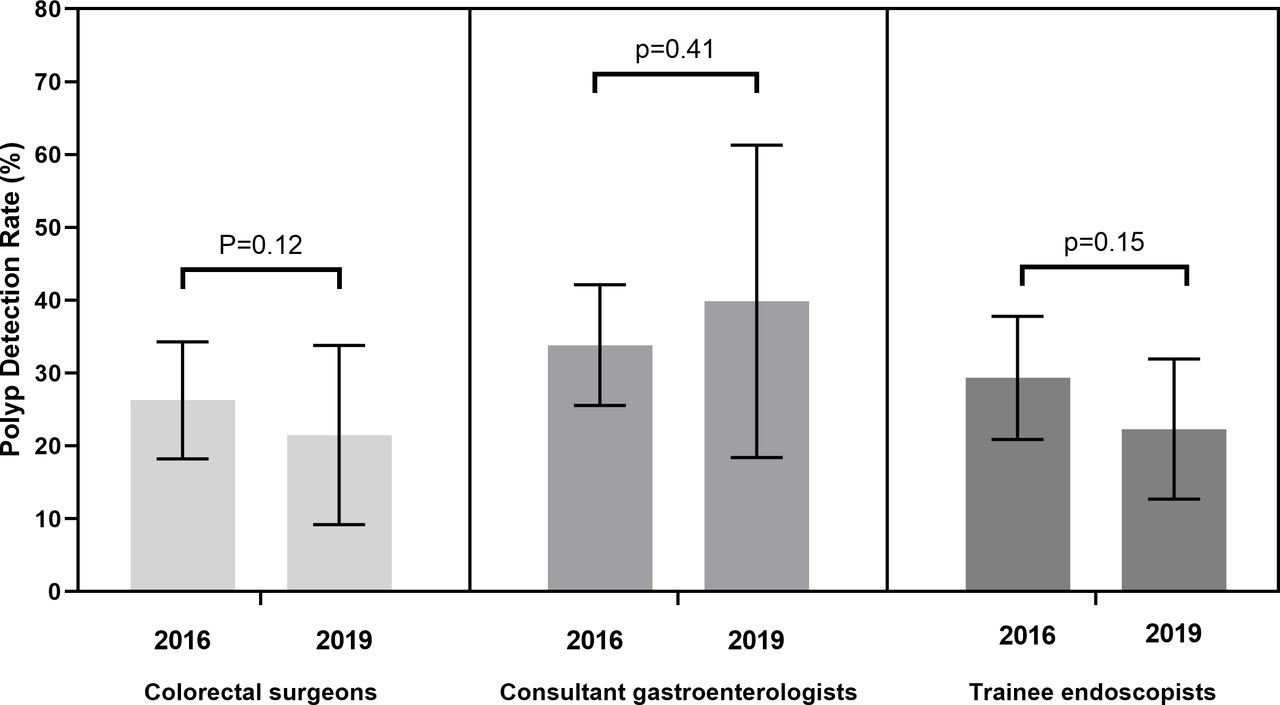
We found no significant differences in ADR between 2016 and 2019 (p=0.64); ADR ranged from 17.2% to 47.1% in 2016 (mean 29.9%) compared with 4% to 67.2% (mean 28.3%) in 2019 (figure 4). All endoscopists met the national minimum ADR of >15% in 2016 while only four endoscopists had ADR <15% in 2019. No statistical differences in ADR were found between the different groups (figure 4).

Comparison of polyp detection rate in 2016 and 2019 between individual groups.
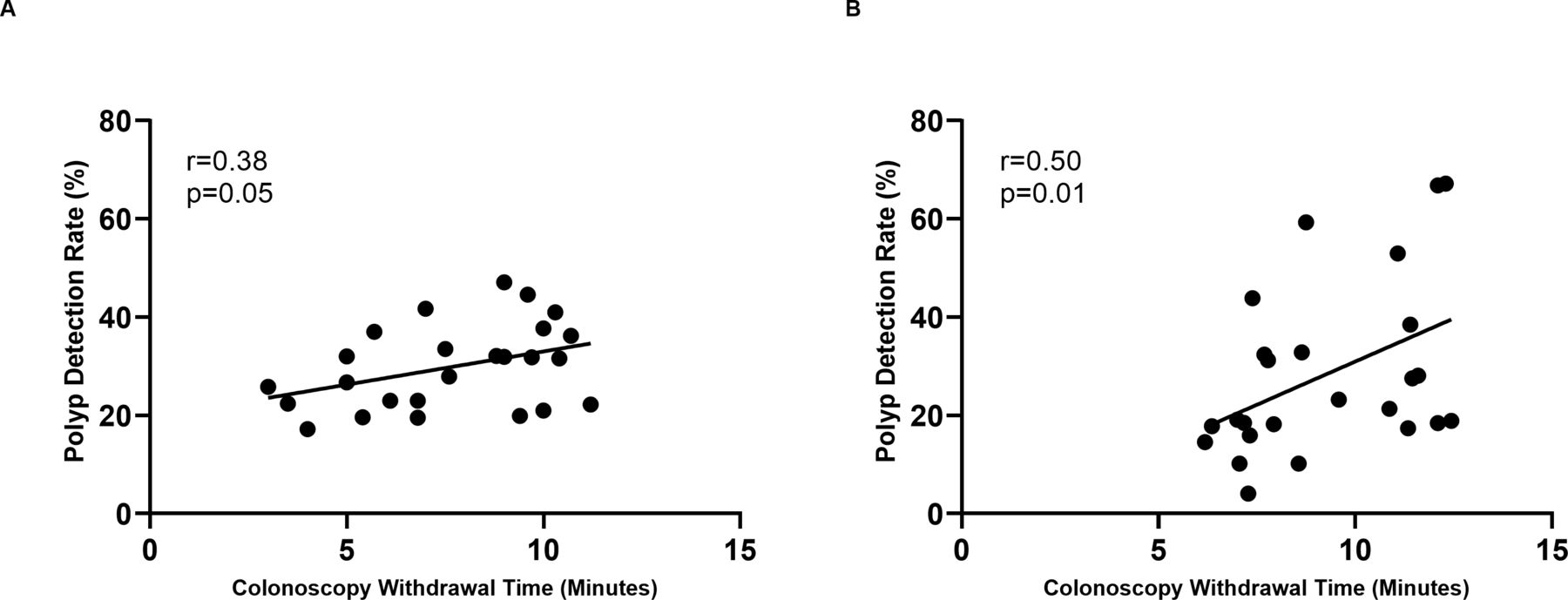
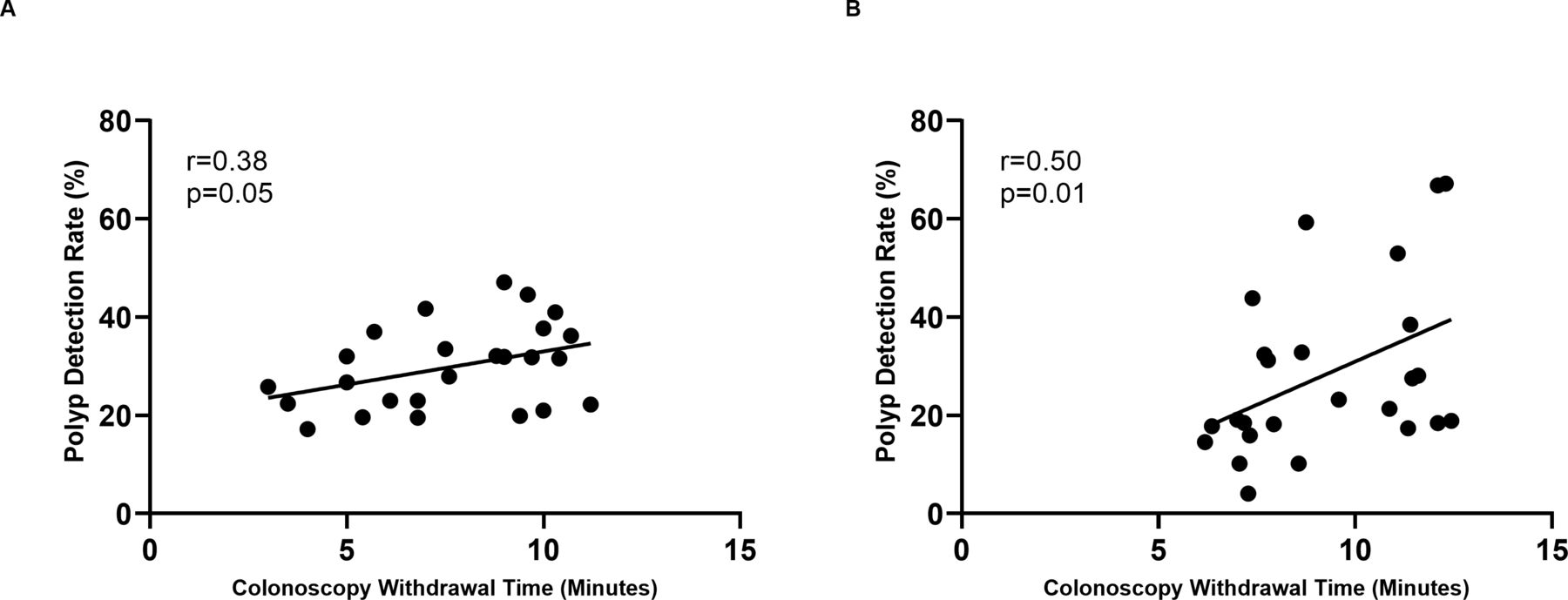
As shown in figure 5, we found positive correlation between CWT and ADR in 2016 (r=0.38, p=0.05) and 2019 (r=0.50, p=0.01).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation between colonoscopy withdrawal time and polyp detection rate in (A) 2016 and (B) 2019.
Mean caecal intubation rate was 91.4% (SD 4.06) in 2016 and 90.6% (SD 5.80) in 2019.
Discussion
By using data from the NED, we found that CWT was significantly longer after using NED with all endoscopists having CWT longer than the recommended minimum withdrawal time of 6 min. Despite the longer withdrawal times, we did not observe a higher PDR. This is likely because the PDR in our centre was already exceeding the national aspirational benchmark of 20% before using NED. Gastroenterology consultants and trainee endoscopists had longer CWT compared with colorectal surgeons both before and after the introduction of NED. Interestingly, we did not observe any differences in PDR between the three groups despite a positive correlation between CWT and PDR.
No previous studies have investigated the effect of NED on CWT. However, previous interventions have been utilised to improve CWT, and thus improving PDR/ADR. Vavricka et al28 demonstrated that endoscopists had significantly longer withdrawal times and ADR when they were aware that their withdrawal times are being monitored. Similarly, Barclay et al29 showed that using a timer with intermittent audible signals to pace examination during colonoscopy withdrawal across different colonic segments lengthened withdrawal times and increased neoplastic lesion detection. Sinn et al 30 and Sawhney et al31 reporte d that formal documentation of withdrawal times at the end of the procedure led to longer withdrawal times. However, similar to our findings, the longer withdrawal times did not lead to higher ADR. Conversely, multiple studies have shown that quality improvement programmes and feedback to endoscopists can lead to higher ADR but have little or no impact on withdrawal times.32–38 The impact of automated feedback of NED KPIs on endoscopists and endoscopy leads is the current study area in a multicentre randomised controlled trial.39
The differences in PDR between surgeons and gastroenterologists have been conflicting.5 40 41 In a recent study of non-screening colonoscopies,9 we found significant CWT and PDR variations among different groups of endoscopists according to their specialties. The current study shows similar CWT variations, with colorectal surgeons having shorter withdrawal times than gastroenterology consultants and trainee endoscopists. However, colorectal surgeons showed the most marked improvement in CWT after using NED (p=0.0004) and the shorter withdrawal times did not seem to affect their PDR.
Although slowing down during colonoscopy withdrawal, to give time for more meticulous examination of colonic folds, is an important modifiable factor influencing PDR,16 it is not equivalent to withdrawal technique (ie, caecal retroflexion, 360 rotation of the lumen, focal narrow band imaging (NBI), position change), which remains key in detecting colonic lesions.22 42 Also, PDR is influenced by other factors such as adequate bowel preparation,43 44 patients’ characteristics,45 the timing of colonoscopies46 and even delays in colonoscopy starting time.47 This may explain why colorectal surgeons had similar PDR to both gastroenterology consultants and trainee endoscopists despite having shorter withdrawal times.
Our study had limitations. First, the retrospective nature of the database search is subject to multiple confounders, which may account for some of the differences observed in CWT and PDR. Second, three endoscopists performed screening colonoscopies in 2019 that were included in our analysis, which may have led to longer mean CWT in this group. However, we do not anticipate that endoscopists’ practice changes according to the colonoscopy indication. Third, this study was conducted at a single tertiary referral centre with experienced endoscopists, which is a plausible explanation for having longer CWT and higher PDR than the national average. Moreover, colorectal surgeons perform a significantly high number of colonoscopies in our centre. Therefore, the results may not be generalised to other endoscopy units. Conducting a similar study in a multicentre setting may yield more generalisable results. Finally, as the ratio between PDR and ADR has not been identified and validated in this study, we were unable to use PDR as a surrogate for ADR.
In conclusion, NED offers endoscopists the chance to monitor and audit their own KPIs, which seems to be the most effective way of improving colonoscopy practice. Using NED led to longer CWTs. However, variations in practice still exist between endoscopists. A national colonoscopy audit using data from NED is required to evaluate whether wide variations in practice across endoscopy units in the UK still exist and to ensure minimum colonoscopy quality standards are achieved.
Data availability statement
Data are available upon reasonable request. Data are available upon reasonable request.
Ethics statements
References
Footnotes
Twitter @Mo_Shiha
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.