Article Text

Abstract
Objective Multiple factors predispose patients with cirrhosis to sepsis and/or bacteraemia and this has a high mortality rate. Within different geographical regions there are marked differences in the prevalence of infection with multidrug-resistant organisms (MDR). This study examined risk factors for and outcomes of sepsis/bacteraemia in public hospital admissions with cirrhosis in the state of Queensland, Australia, over the last decade, along with the bacterial pathogens responsible and their antibiotic susceptibility profiles.
Design A population-based retrospective cohort study of public hospital admissions was conducted from 1 January 2008 to 31 December 2017. Hospital admissions for patients with a diagnosis of cirrhosis were categorised by the presence or absence of sepsis/bacteraemia. Clinical and sociodemographic information including cirrhosis aetiology, complications and comorbidities, and in-hospital mortality were examined using bivariate and multivariate analyses. In patients with bacteraemia, the type and prevalence of bacteria and antibiotic resistance was assessed.
Results Sepsis/bacteraemia was present in 3951 of 103 165 hospital admissions with a diagnosis of cirrhosis. Factors associated with sepsis/bacteraemia included disease aetiology, particularly primary sclerosing cholangitis (adj-OR 15.09, 95% CI 12.24 to 18.60), alcohol (adj-OR 2.90, 95% CI 2.71 to 3.09), Charlson Comorbidity Index ≥3 (adj-OR 3.54, 95% CI 3.19 to 3.93) and diabetes (adj-OR 1.87, 95% CI 1.74 to 2.01). Overall case-fatality rate among admissions with sepsis/bacteraemia was 27.7% (95% CI 26.3% to 29.1%) vs 3.7% (95% CI 3.6% to 3.8%) without sepsis/bacteraemia. In-hospital death was significantly associated with sepsis/bacteraemia (adj-OR 6.50, 95% CI 5.95 to 7.11). The most common organisms identified were Escherichia coli and Staphylococcus aureus, present in 22.9% and 18.1%, respectively, of the 2265 admissions with a positive blood culture. The prevalence of MDR bacteria was low (5.6%)
Conclusion Morbidity and mortality related to sepsis/bacteraemia in patients with cirrhosis remains a critical clinical problem.
- epidemiology
- liver
- bacterial infection
Data availability statement
Data are available on reasonable request. Ethics amendment would be required for data sharing.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known about this subject?
Sepsis and bacteraemia occur commonly in patients with cirrhosis, with marked differences in the prevalence of infection with multidrug-resistant (MDR) organisms and in patients’ clinical characteristics within different geographical regions. Large global cross-sectional studies have been completed on the epidemiology and outcomes of bacterial infections in hospitalised patients with cirrhosis, however, Australia was not included and there are no population-based data available from this geographical region.
What are the new findings?
In this study, factors associated with sepsis/bacteraemia included disease aetiology, particularly primary sclerosing cholangitis and alcohol, high comorbidity burden, and diabetes. The prevalence of MDR bacteria in cirrhotic patients in Australia was lower than that of reported data from Europe, Asia and the USA. Moreover, methicillin-resistant Staphylococcus aureus was the most common MDR organism in Australia cirrhotic patients while other bacteria (ie, ESBL, Escherichia coli) have been reported as the most common MDR organism in European patients with cirrhosis.
How might it impact on clinical practice in the foreseeable future?
Empirical antibiotic treatment protocols should be adapted to local epidemiology along with evidence-based sepsis management protocols such as timely initiation of antibiotic therapy, lower threshold for and access to intensive care services, and appropriate fluid resuscitation. There is also the need for vigilance about infection-prevention measures, particularly in older patients with type 2 diabetes mellitus and alcohol-related liver disease who have a high risk of sepsis.
Introduction
During hospitalisation, bacterial infections occur in 25%–35% of patients with cirrhosis1 and are responsible for much of the morbidity, mortality and resource utilisation in this population.2 The most common infections include spontaneous bacterial peritonitis (SBP), urinary tract infections (UTI), pneumonia and soft tissue infections.3 In addition, blood stream infections are common, occurring in 4%–21% of patients with cirrhosis,4 along with an increased risk of developing bacteraemia during other infections3 . Irrespective of liver disease aetiology, multiple factors predispose cirrhotic patients to bacteraemia; including increased translocation of gut-resident bacteria,5 cirrhosis-associated immune dysfunction6 and the requirement for invasive procedures or indwelling devices during hospitalisation. Bacterial infections may lead to sepsis (defined as suspected or confirmed infection in the presence of an organ failure)7 and may precipitate or worsen hepatic decompensation.
In patients with cirrhosis, bacteraemia has a mortality rate between 23% and 58%,8 significantly higher than other bacterial infections8, or bloodstream infections in patients without cirrhosis.9 The increase in mortality is due to haemodynamic and immune system-related alterations that occur in cirrhosis, and prompt empirical antibiotic therapy is key to optimising patient outcomes.7 Appropriate antibiotic selection is guided by the local epidemiology of bloodstream infections and the prevalence of antibiotic-resistant bacteria. Recent studies from Europe,10 Asia11 and the USA12 demonstrate that a substantial proportion (23%–44%) of cirrhotic patients with bacterial infections have multidrug-resistant organisms (MDRO), which may lead to inappropriate empiric antibiotic therapy and higher mortality. Increasing prevalence of antibiotic resistance in patients with cirrhosis is likely driven by recurrent hospital admissions, invasive procedures and frequent exposure to prophylactic or therapeutic antibiotics, however, the prevalence may also be influenced by local or regional measures13 to prevent the spread of antibiotic resistance.
Although the epidemiology and outcomes of bacterial infections in hospitalised patients with cirrhosis have recently been examined in a global cross-sectional study,14 Australia was not included in this study, and there are no population-based data available from this geographic region. This is important due to marked differences in the prevalence of infection with MDRO and in the demographic and clinical characteristics of patients with cirrhosis from different countries.14 While in many parts of the Asia-Pacific region antimicrobial use is largely unregulated, Australia has a national antimicrobial resistance strategy to promote a coordinated response to this problem.15 Conducting this study in Queensland which is the third most populous Australian state and with a large proportion of its population in regional areas, allowed the inclusion of large numbers of patients from a mix of regional and metropolitan area health services. As Australia has a universal health system, results from this Queensland study are likely to be generalisable to patients with cirrhosis in other Australian states.
In Australia, excessive alcohol consumption remains the most important factor contributing to cirrhosis, while the burden of metabolic comorbidity increased during 2008–2016.16 In particular, the prevalence of coding for type 2 diabetes mellitus (T2DM) among patients with cirrhosis doubled from 13.7% in 2008–2010 to 25.4% in 2014–2016.16 However, it remains unclear whether this changing prevalence of aetiological factors and comorbidities has an impact on the risk of sepsis and bacteraemia in people hospitalised for cirrhosis or the clinical outcomes of these infections. Therefore, the aim of this study was to describe the epidemiology of bacterial infection and sepsis in a population-based study of Queensland public hospital admissions with cirrhosis over the last decade and identify risk factors across the spectrum of clinical severity, namely: sepsis regardless of bacteraemia, bacteraemia without sepsis, and uncomplicated infection without sepsis or documented bacteraemia. We will also assess mortality in these patients and identify the most common bacterial pathogens and their antibiotic susceptibility profiles.
Methods
Study design
A population-based retrospective cohort study of all adults treated in hospital with cirrhosis in Queensland during 1 January 2008 and 31 December 2017 was conducted. The primary data sources were the Queensland Hospital Admitted Patient Data Collection (QHAPDC) that contains information on all hospital episodes of care for patients admitted to Queensland public and private hospitals, and the AUSLAB database that contains all pathology data including information on infections of patients admitted to Queensland public hospitals.
Setting and participants
All adult patients discharged from a Queensland public or private hospital during 2008–2017 with a ‘principal diagnosis’ or ‘other diagnosis’ of cirrhosis, or related complications or procedures, and/or died during 2008–2017 with a principal or other cause of death of cirrhosis or related complications were ascertained. The study cohort (referred to as ‘parent cohort’) was identified via a comprehensive list of ICD-10-AM diagnosis and procedure codes provided to the Statistical Analysis Linkage Unit. We obtained pathology data from AUSLAB pertaining to infections in Queensland public hospitals, namely microbiological culture from blood and ascitic fluid, causative pathogens, and their antibiotic susceptibility profiles for the parent cohort. Blood culture data was used in the analysis, while ascitic fluid culture and neutrophil count were used to define SBP. Patient clinical and demographic data were linked to microbiology data for each admission.
Data analysed here included all hospital admissions of adult patients with cirrhosis who were identified from ICD‐10‐AM codes. We excluded admissions where the patient’s age was <20 years, residential location was unknown, interstate or overseas, and admissions to private hospitals. The latter were excluded because the AUSLAB database did not include pathology data from private hospitals. Adult patients younger than 20 years of age were excluded because the Statistical Analysis Linkage Unit only provided age groups (5-year age group, capped at 75+ years) and we could not identify adult patients within the 15–20 years age group. Details regarding the selection of hospital admissions of patients with cirrhosis have been described previously.17 Briefly, a patient with cirrhosis was defined by hospitalisation that included at least one ICD‐10‐AM code for cirrhosis (K70.3, K74.4, K74.5, K74.6), hepatocellular carcinoma (HCC) (C22.0), alcoholic hepatic failure (K70.4), hepatic failure unspecified (K72.9), ascites (R18), varices with or without bleeding (I85.0, I85.9, I98.3, I98.2, I86.4), hepatorenal syndrome (K76.7) and portal hypertension (K76.6) as primary diagnosis or other diagnosis. Patients with portal hypertension related to primary thrombophilia (D68.5, D68.6) and schistosomiasis (K77.0, B65.1, B65.9) were classified as non-cirrhotic. The accuracy of this algorithm for identification of patients with cirrhosis has been reported to have a 76% negative predictive value (95% CI 0.67 to 0.84) and 88% positive predictive value (95% CI 0.84 to 0.90).17
The AUSLAB database included 208 220 results linked to this time period and patient cohort; 27 580 were excluded because they were not linked to an admission in the parent cohort; 21 672 were excluded based on age, residence outside Queensland, or private hospital admission. There were a total of 158 968 eligible AUSLAB results: 93 923 were from patients with cirrhosis as defined by the abovementioned algorithm, and 65 045 were from admissions that preceded the cirrhosis diagnosis.
Variables
Clinical and sociodemographic information as well as information about hospital discharge (eg, in-hospital mortality) for all hospital episodes of care were obtained from QHAPDC. Patients’ residential postcodes were used to determine area-based index of relative socioeconomic disadvantage score18 and remoteness of residence.19 Aetiology of liver disease and comorbidity at each admission was determined based on recorded ICD code for primary or other diagnosis. Comorbidity burden at the index admission was measured using the Charlson Comorbidity Index (Charlson index)20 using validated coding algorithms.21 Length of hospital stay was calculated by adding all days the patient was an admitted patient during one hospital stay, including when patients were transferred within the same or to another hospital. Patients were categorised as ‘in-hospital death’ if status at separation of patient was ‘death’, and as ‘live discharge’ if status at separation of patient was ‘discharge’ or ‘transfer’. The primary outcomes of interest were the presence of sepsis and in-hospital mortality.
Patient selection
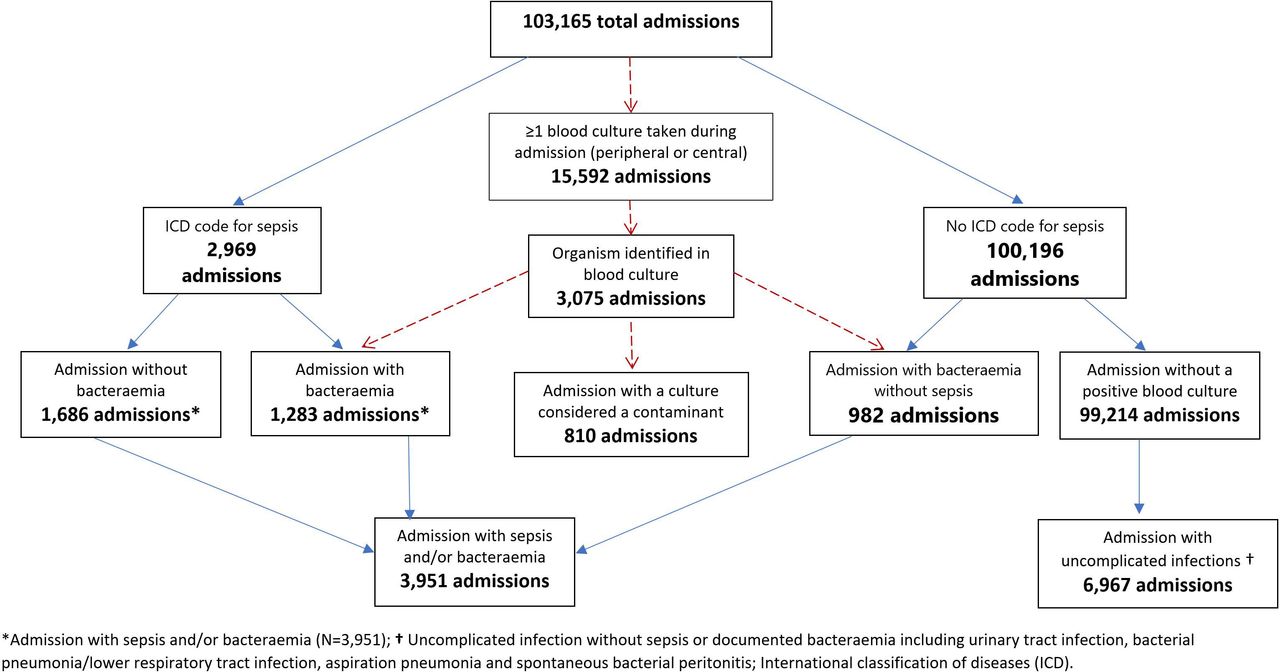
All hospital admissions were categorised by the presence vs absence of sepsis/bacteraemia (figure 1). Hospital admissions were considered positive for sepsis if they had an ICD code for sepsis (A40 or A41, (online supplemental table 1) with or without bacteraemia (a blood culture that has grown a bacteria that is not considered a contaminant)(figure 1). As medical records were not reviewed, admissions in which the patient had a single culture with a bacteria that could have been a contaminant were categorised as ‘no bacteraemia’, and admissions with at least one positive blood culture that was not thought to be a contaminant were classed as ‘bacteraemia’. We were unable to determine if a patient had >1 episode of sepsis or bacteraemia during an admission. Common possible contaminants included Coagulase negative Staphylococci, Bacillus spp, Micrococcus spp, Actinomyces spp, Rhodococcus spp, Kocuria spp, Corynebacterium spp, Propionibacterium spp and mixed flora. Other infections examined included UTI, bacterial pneumonia/lower respiratory tract infection, aspiration pneumonia and SBP. Presence of infection was determined based on recorded ICD code for primary or other diagnosis. Ascites was defined by the ICD-10-AM code R18, and/or the presence of an ascitic fluid sample linked to that hospital admission. For SBP the presence of infection was also confirmed by ascitic fluid polymorphonuclear count >250 cells/mm3 following interrogation of AUSLAB data.
Supplemental material

{kind=link}
Pathway for categorising hospital admissions with sepsis/bacteraemia and uncomplicated infection.
Statistical methods
Analyses were conducted using Stata/SE (V.15; Stata) and JMP Pro V.14.1.0 (SAS Institute). Categorical variables were presented as numbers and percentages and the χ2 test was used to compare categorical variables (Fisher’s exact test was used when one of the expected values in a table was less than 5). All p values were two sided.
Case-fatality rates (in-hospital deaths divided by hospital admissions) were calculated per calendar year and per calendar period (2008–2010 and 2015–2017).
Multivariable logistic regression was used to examine factors that were independent predictors of presence of sepsis. The decision as to which independent variables were included was first determined based on the results of bivariable analyses. We then performed multivariable analysis to appreciate the extent of confounding and applied stepwise model selection (p=0.20 as the significance level at which variables were entered or removed from to the model). We also accounted for our previous analysis of this patient cohort that examined relationships and dependencies among variables and their association with in-hospital mortality and/or sepsis, as well as the clinical relevance of variables.22 The final multivariable model for sepsis included sex, age group, remoteness of residence, socioeconomic status, diabetes and alcohol aetiology. Alcohol and diabetes were included in both models due to previously reported associations with susceptibility to infection and in-hospital mortality.23–25 Sensitivity analyses were conducted by repeating the analysis excluding 1-day admissions,. Multivariable logistic regression was also used to examine factors that were independent predictors of in-hospital mortality. The final multivariable model included age group, alcohol aetiology, Charlson Comorbidity Index, sepsis/bacteraemia and complications of cirrhosis (ascites, hepatic encephalopathy, gastrointestinal bleeding, hepatorenal syndrome and HCC). The management and prognosis of various diseases included in the Carlson Comorbidity Index20 has changed substantially since the index was developed, altering the relevance of variables contained in the score. We have, therefore, created a second model with diabetes as an indicator of comorbidity risk, as it is a common comorbid condition in patients with cirrhosis and is associated with adverse patient outcomes including morbidity and mortality.23 Results are presented as ORs with 95% CIs.
Results
Patient population and presence of sepsis/bacteraemia
During 2008–2017, 12 423 people aged ≥20 years had 103 165 Queensland public hospital admissions with a diagnosis of cirrhosis, with 54.1% (55,825 admissions) longer than 1 day. Data were also analysed excluding 1-day admissions, as their clinical significance is likely different from that of longer admissions (eg, planned diagnostic or therapeutic procedures vs management of disease complications).
There was a predominance of male gender (69.2%), age 50–69 years (55.0%), 54.3% were classified in the lowest two quintiles of socioeconomic disadvantage and in 57.7% of admissions patients resided in a major city area. A liver disease aetiology was coded in 56.5% of all admissions (80.2% of admissions >1 day), including alcohol-related in 32.3%, chronic hepatitis C in 17.3%, chronic hepatitis B in 3% and non-alcoholic fatty liver disease/non-alcoholic steatohepatitis in 2.4%.
At least one blood culture was taken in 15 592 (15.1%) of the 103 165 admissions and in 2265 admissions (2.2%), ≥1 blood culture grew an organism that was not considered a contaminant. In 810 (0.8%) admissions, a bacteria that was considered a contaminant (5.2% of patients that had a culture taken) was identified. Blood cultures were negative in 12 517 (12.1%) admissions (80.3% of patients that had a blood culture taken) (figure 1). No blood sample was taken in 87 573 admissions (84.9%). An ICD code for sepsis was recorded in 2969 admissions and a positive blood culture (bacteraemia) was seen in 1283 of these (43.2%) (figure 1). Of the 2265 admissions with bacteraemia displayed in figure 1 and 1283 (57.6%) had an ICD code for sepsis. In a further 982 admissions without an ICD code for sepsis, the bacteria grown were considered likely to have caused a significant infection. In total, 3951 admissions comprised the sepsis/bacteraemia group (3.8% of total admissions; 7.4% of admissions >1 day); an ICD code for sepsis was present in 75.1% (figure 1) and bacteraemia was present in 57.2%. Among the patients with sepsis/bacteraemia, ICD codes for UTI or bacterial pneumonia were present in 22% and 19.8% of admissions, respectively.
A 2.3-fold increase in the number of admissions with a diagnosis of sepsis/bacteraemia was observed during the 10-year study period (from 762 in 2008–2010 to 1742 in 2015–2017). When considered as a proportion of all hospital admissions for patients with cirrhosis, the proportion of admissions with sepsis/bacteraemia decreased from 4.6% in 2008–2010 to 3.8% in 2015–2017 (p<0.001). The corresponding proportions among hospital admissions>1 day were 7.5% and 7.1% (p=0.260), respectively. Over the 10-year study period admissions with a diagnosis of sepsis/bacteraemia had a median length of stay of 13 days (IQR 7–26) compared with 2 days (IQR 1–5) for admissions without (p<0.001).
Risk factors across the spectrum of clinical severity of infections
Although there were significant differences in sociodemographic factors (gender, remoteness of residence and socioeconomic status) according to presence or absence of sepsis/bacteraemia, the differences were small. One-quarter of the admissions with sepsis/bacteraemia had a Charlson Comorbidity Index of ≥3 (reflecting a greater number and severity of comorbidities) compared with 11% of admissions without sepsis/bacteraemia, with a difference in the prevalence of diabetes also significant (p<0.001). With respect to liver disease aetiology, there was a 10-fold higher prevalence of primary sclerosing cholangitis (PSC) in the admissions with sepsis/bacteraemia, compared with their counterparts, although the overall numbers were small. Complications of cirrhosis were also more prevalent in admissions with sepsis/bacteraemia, particularly hepatorenal syndrome, hepatic encephalopathy, ascites and SBP. In addition, the length of hospital stay was markedly different between admissions with and without sepsis/bacteraemia, with 61.5% of patients with sepsis/bacteraemia having an admission ≥10 days (online supplemental table 2).
Supplemental material
In multivariate analysis, we examined the associations between sociodemographic and clinical factors across the spectrum of clinical severity, namely: sepsis and/or bacteraemia (overall), and sepsis regardless of bacteraemia, bacteraemia without sepsis, and uncomplicated infection without sepsis or documented bacteraemia. Overall, 19 factors were associated with sepsis/bacteraemia (table 1). Of the factors included in the final multivariable model, alcohol as liver disease aetiology (adj-OR 2.90, 95% CI 2.71 to 3.09) and diabetes (adj-OR 1.87, 95% CI 1.74 to 2.01) were the strongest risk factors for sepsis/bacteraemia. As other studies reported a greater risk of infection with increasing severity of liver disease,25 we repeated the multivariable analysis adjusting for complications of cirrhosis (hepatorenal syndrome, hepatic encephalopathy, ascites, jaundice, HCC and variceal bleeding) as a ‘surrogate’ of liver disease severity; alcohol-related admissions remained associated with sepsis/bacteraemia (adj-OR 2.12, 95% CI 1.98 to 2.28).
Factors associated with sepsis and/or bacteraemia (overall), and sepsis regardless of bacteraemia, uncomplicated infection without sepsis or documented bacteraemia and bacteraemia without sepsis
Other socioeconomic and clinical factors examined were strongly associated with sepsis/bacteraemia including Charlson Comorbidity Index of ≥3 (adj-OR 3.54, 95% CI 3.19 to 3.93), complications of cirrhosis (the highest ORs were for hepatorenal syndrome (adj-OR 4.53, 95% CI 3.85 to 5.34) and hepatic encephalopathy (adj-OR 4.26, 95% CI 3.77 to 4.81) and liver disease aetiology, particularly PSC (adj-OR=15.09, 95% CI 12.24 to 18.60). Of infections, aspiration pneumonia (adj-OR=8.77, 95% CI 7.58 to 10.15) and SBP (adj-OR 8.55, 95% CI 7.27 to 10.06) were strongly associated with sepsis/bacteraemia. Longer length of stay was significantly associated with sepsis/bacteraemia, with the odds of admissions longer than 30 days including sepsis/bacteraemia being 19 times as large as the odds for admissions lasting 2–4 days. When the analyses were repeated following exclusion of 1-day admissions, the results were similar (table 1), although the effect sizes were in general smaller (online supplemental table 3).
Supplemental material
In multivariate analysis examining factors associated with presence or absence of sepsis regardless of bacteraemia, the same 19 factors were associated with sepsis regardless of bacteraemia, and the adjusted ORs were in general similar or larger than that of the overall group (sepsis and/or bacteraemia). Regarding factors associated with bacteraemia without sepsis and uncomplicated infection without sepsis or documented bacteraemia, associations were similar to the overall group, but the effect sizes were in general smaller (table 1).
In-hospital mortality/case-fatality rate
The overall case-fatality rate among admissions with sepsis/bacteraemia during the study period was 27.7% (95% CI 26.3% to 29.1%) vs 3.7% (95% CI 3.6% to 3.8%) without sepsis/bacteraemia. The case fatality rate decreased progressively over the decade for patients with sepsis/bacteraemia from 32.2% in 2008–2010, to 25.9% in 2015–2017 (p=0.001). A decline was also seen among patients with sepsis regardless of bacteraemia (37.7% vs 28.1%, respectively; p<0.001), and patients with uncomplicated infection without sepsis or documented bacteraemia (16.8% vs 10.2%, p<0.001), with no significant difference in the case fatality rate among patients with bacteraemia without sepsis (19.7% vs 16.8%, p=0.38). For patients without sepsis/bacteraemia, the case fatality rate decreased from 4.9% in 2008–2010, to 2.8% in 2015–2017 (p<0.001). As a proportion of all deaths, the rate of in-hospital mortality associated with sepsis/bacteraemia remained relatively stable at 24.0% in 2008–2010 and 26.3% in 2015–2017 (p=0.19).
Following multivariate analysis adjusting for complications of cirrhosis, age, Charlson Comorbidity Index and alcohol as liver disease aetiology, in all admissions, in-hospital death was significantly associated with sepsis/bacteraemia (adj-OR 6.50, 95% CI 5.95 to 7.11). Other factors independently associated with mortality included age ≥50 years (adj-OR 1.64, 95% CI 1.49 to 1.79), alcohol aetiology (adj-OR 1.86, 95% CI 1.73 to 2.00), Charlson Comorbidity Index ≥3 (adj-OR 5.19, 95% CI 4.78 to 5.63), ascites (adj-OR 1.99, CI 1.85 to 2.15), hepatic encephalopathy (adj-OR 3.24, 95% CI 2.84 to 3.70), hepatorenal syndrome (adj-OR 10.50, 95% CI 9.03 to 12.21), variceal bleeding (adj-OR 2.01, 95% CI 1.85 to 2.18) and HCC (adj-OR 4.64, 95% CI 4.24 to 5.09). When the multivariate analysis was repeated including diabetes instead of Charlson Comorbidity Index in the model, diabetes was independently associated with mortality in all admissions (adj-OR 1.23, 95% CI 1.15 to 1.33), but was not significant in the sepsis/bacteraemia subgroup (adj-OR 0.85, 95% CI 0.72 to 1.01) (online supplemental table 4).
Supplemental material
MDR bacteria were identified in blood cultures in 132 admissions (one admission had two different MDRs grown). Following multivariate analysis adjusting for complications of cirrhosis, age, Charlson Comorbidity Index and alcohol as liver disease aetiology, presence of MDR bacteria in the blood was not associated with in-hospital mortality (adj-OR 0.92, 95% CI 0.59 to 1.45; p=0.727).
Type and prevalence of bacteria and antibiotic resistance in patients with bacteraemia
The most common organism identified was Escherichia coli, present in 22.9% of the 2265 admissions with a positive blood culture. Staphylococcus aureus was the second most common bacteria, present in 18.1% of admissions with a positive blood culture (table 2).
Type and prevalence of bacteria identified in blood cultures during 2008–2017
The proportion of organisms with antibiotic resistance over the 10-year study period is summarised in table 3. More than 80% of S. aureus isolates were resistant to penicillin; while 9.1% and 10% of E. coli isolates were resistant to ceftriaxone and ciprofloxacin, respectively. The prevalence of E. coli resistance to ceftriaxone increased from 3.5% in 2008–2010 to 10.3% in 2015–17 (p=0.029), and the resistance to ciprofloxacin increased from 3.4% in 2008–2010 to 13.8% in 2015–17 (p=0.003) (table 4).
The proportion of organisms with antibiotic resistance during 2008–2017
Number and proportion of admissions with Escherichia coli antibiotic resistance and number and proportion of admissions with a multidrug-resistant organism
Overall, a MDR bacterium was identified in 5.6% of admissions (table 2), with an increase from 2.3% in 2008–2010 to 4.6% in 2015–2017 (p=0.015) (table 4). However, at the level of individual bacteria, only E. coli (ESBL) showed a significant increase in prevalence over the decade (p=0.01).
Discussion
This large population-based study from Australia has shown that sepsis and/or bacteraemia occur commonly in hospitalised patients with cirrhosis (7.4% of admissions longer than 1 day) and are associated with high in-hospital mortality (27.7%). The most common bacteria identified was E. coli, present in 22.9% of admissions with a positive blood culture. Although the prevalence of E. coli resistance to ceftriaxone increased from 3.5% in 2008–2010 to 10.3% in 2015–2017, and the resistance to ciprofloxacin increased from 3.4% in 2008–2010 to 13.8% in 2015–2017, overall, the prevalence of MDR bacteria was low (5.6% of admissions in which an organism was identified).
Our data concur with studies demonstrating that bloodstream infections are a common complication in patients with cirrhosis,7 8 with a 10-fold higher incidence rate than the general population.26 In our cohort, the factor most notably associated with sepsis/bacteraemia was the presence of PSC (OR 15.09, 95% CI 12.24 to 18.60), although overall, this liver disease was recorded in only 0.5% of admissions, and the low overall proportion of patients with a coded liver disease aetiology introduces a bias in the study design. Cholangitis occurs commonly in patients with PSC as a consequence of biliary strictures, alteration in gut microbiota composition and endoscopic or surgical manipulation.27 Patients with alcohol-related liver disease (ALD) had a 2.9-fold higher risk of sepsis/bacteraemia than those with other causes of cirrhosis. This relationship persisted following adjustment for cirrhosis complications, as a surrogate marker for liver disease severity. Alcohol modifies the composition of gut microbiota and leads to increased intestinal permeability, facilitating bacterial translocation,25 however, its contribution to promoting sepsis, independent of the extent of liver dysfunction, remains unresolved.
A higher number of comorbidities was also a greater risk for development of sepsis/bacteraemia as well as for bacteraemia without sepsis and uncomplicated infection without sepsis or documented bacteraemia, in agreement with findings in patients without cirrhosis.28 29 In particular, patients with T2DM have higher susceptibility to infections and development of sepsis,30 although few studies are available about the impact in the cirrhotic population. In our study, patients with T2DM were 83% more likely to have sepsis/bacteraemia than those without T2DM. A similar finding was reported in a retrospective cohort study of hospitalised cirrhotic patients with skin infections (n=122; 23% with T2DM).31 Following multivariate analysis, T2DM was a key factor contributing to bacteraemia in these patients (p<0.001; OR 1.98, 95% CI 1.59 to 4.15).31 T2DM is associated with chronic inflammation and immune dysregulation32 that may have a synergistic effect in the setting of cirrhosis associated immune dysfunction, leading to increased risk of bacterial infection and related complications.
As expected, our data confirm the striking impact of sepsis/bacteraemia on clinical outcomes in patients with cirrhosis, with a sixfold increase in length of hospital admission and a 6.5-fold increase in in-hospital mortality compared with patients without sepsis/bacteraemia. Severe complications of cirrhosis, particularly hepatorenal syndrome and hepatic encephalopathy, were also more common in patients with the spectrum of clinical severity of infection from sepsis/bacteraemia to bacteraemia without sepsis, likely precipitated by the infection. At a population level, hospital mortality for sepsis was estimated to be 17% in high-income countries for the years 2003–2015,26 substantially lower than the mortality rate for our cirrhotic patients with sepsis (27.7%). Despite a reduction in sepsis-related mortality from 2008 to 2013, the rate has remained constant over the last 5 years. Indeed, as a proportion of total mortality, there has been a small but non-significant increase in sepsis-related mortality over the last decade. These findings suggest a need to be vigilant about infection-prevention measures, particularly in older patients with T2DM and ALD who have a high risk of sepsis, since in these multimorbid patients with cirrhosis, sepsis-related deaths may not be preventable.33
In our cohort with bacteraemia, the most commonly isolated organisms (E. coli 22.9%, S. aureus 19.1%, S. viridans 9% and K. pneumonia 7.9%) were broadly similar to those reported in patients with decompensated cirrhosis in other centres.8 10 12 14 34 Intestinal bacterial translocation is a key route for development of bacteraemia in cirrhotic patients, as evidenced by the prominent role for Enterobacterales. Staphylococcal bloodstream infections were also common, likely due to the frequent requirement for invasive or therapeutic procedures. In contrast to studies in Europe, Asia and the USA, however, a striking finding in our population-based study, was the low prevalence of MDR bacteria, with a significant increase over the decade only for E. coli ESBL (4.6% in 2015–2017).35 There were differences between geographical areas. A multicentre prospective study (2015–2016) found a global prevalence of MDR bacteria of 34% (95% CI 31% to 37%) among 1302 hospitalised patients with cirrhosis, with a rate of 28% in Europe and 27% in North America.14 The most common MDRO found in cirrhotic patients in Europe is ESBL E. coli10 as compared with our finding in Australia where MRSA was most prevalent. The low rate of MDR bacteria in Australian patients with cirrhosis is likely multifactorial, due to our relative geographical isolation, strong antimicrobial stewardship and policies to restrict antimicrobial use in production animals and agriculture,13 15 and strengthens the concept that empirical antibiotic treatment protocols should be adapted to local epidemiology. For example, the empirical use of carbapenems suggested by Piano et al in nosocomial SBP36 and by Merli et al in healthcare associated infections37 does not seem justified in Australia, while it is more effective than the standard of care in Italy.
Our study has a number of strengths, including the near complete population-based data for public hospital admissions for cirrhosis and linked microbiological data over the last decade, curation of data by a multidisciplinary team including epidemiology, hepatology, infectious diseases, microbiology and the statistical services branch of Queensland Health, and the use of widely accepted and validated coding algorithms for cirrhosis17 and comorbidities.20 Although the study was restricted to public hospital admissions, we have previously shown that more than three-quarters of admissions for cirrhosis occur in the public sector, and we believe this is unlikely to impact the epidemiology of the study.22 An important limitation with hospital admissions data is the inability to assess cirrhosis severity using the Child-Pugh or MELD scores, which are strong predictors of a patient’s risk of mortality, or the presence of acute-on-chronic liver failure.38 Other important limitations are the lack of data about antibiotic use in the previous 3 months, including the use of norfloxacin or rifaximin prophylaxis, and the lack of information about hospital admission area (eg, intensive care unit).39 In addition, due to the limited accuracy of ICD code classification, there is the potential for misclassification of sepsis, liver disease aetiology, cirrhosis and related complications as well as comorbidities. Data were dependent on the quality of coding of hospital admissions, which may vary from site to site (eg, small hospitals in regional areas) and over time. For example, if the primary reason for admission was not related to cirrhosis, medical staff may be less likely to document aetiology of cirrhosis.
The definition of sepsis changed in 2016,40 and while clinically the difference in the definition was not very marked, there is the potential for inaccurate diagnosis of sepsis in 2017 .41 As medical records were not reviewed and hospital admissions data does not provide sufficient detail to distinguish community-acquired and hospital-acquired infection, we could not examine this. Nevertheless, our findings demonstrate that morbidity and mortality related to sepsis/bacteraemia in patients with cirrhosis remains a critical clinical problem. Awareness of factors that increase susceptibility to and mortality with bacterial infection (particularly the role of age, liver disease aetiology and comorbidity burden) may identify ‘high-risk’ patients requiring greater preventative strategies and reinforce the need for ongoing vigilance to avoid infections with MDR bacteria and inappropriate antibiotic use. Empirical antibiotic treatment protocols adapted to local epidemiology along with evidence-based sepsis management protocols that include timely initiation of antibiotic therapy after sepsis recognition, lower threshold for and access to intensive care services, and early and aggressive fluid resuscitation can significantly decrease in-hospital mortality in this patient group.36
Data availability statement
Data are available on reasonable request. Ethics amendment would be required for data sharing.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Human Research Ethics Committees of Queensland Health (HREC/17/QPAH/23; HREC/2018/QMS/43571) and QIMR Berghofer Medical Research Institute (P3506).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
EEP and PCV are joint senior authors.
EEP and PCV contributed equally.
Contributors Study conceptualisation: KMI, EP and PCV; data curation and analysis: ALJ, IUR, KMI, AH, EP and PCV; investigation: ALJ, IUR, AH, KMI, EP and PCV; supervision: EP and PCV; manuscript writing: ALJ, EP and PCV. PCV is responsible for the overall content as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.