Article Text

Abstract
Objective Serum albumin is used as a marker of acute inflammation. Several studies have addressed the association between serum albumin and clinical outcome in patients with ulcerative colitis (UC). While mucosal healing (MH) has been indicated as the therapeutic goal for UC, the association between serum albumin and MH remains unclear. We evaluated this issue in patients with UC overall and explored whether duration of UC affected this association.
Design This cross-sectional study recruited consecutive patients with UC. Study subjects consisted of 273 Japanese patients with UC. Serum albumin was divided into tertiles based on its distribution in all study subjects. One endoscopy specialist was responsible for measuring partial MH and MH, which were defined as a Mayo endoscopic subscore of 0–1 and 0, respectively. The association between serum albumin and clinical outcomes was assessed by multivariate logistic regression.
Results Rates of clinical remission, partial MH and MH were 57.9%, 63% and 26%, respectively. Only high serum albumin (>4.4 mg/dL) was significantly positively associated with MH (OR 2.29 (95% CI: 1.03 to 5.29), p for trend=0.043). In patients with short UC duration (<7 years) only, high serum albumin was significantly positively associated with MH and clinical remission. In patients with long UC duration (≥7 years), in contrast, no association between serum albumin and clinical outcomes was found.
Conclusion In Japanese patients with UC, serum albumin was significantly positively associated with MH. In patients with short UC duration, serum albumin might be a useful complementary marker for MH.
- ulcerative colitis
- inflammatory bowel disease
- endoscopy
Data availability statement
Data are available upon reasonable request. The data sets used and/or analysed during the current study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Serum albumin is associated with clinical outcomes, disease activity and relapse in patients with ulcerative colitis (UC). The association between albumin and mucosal healing (MH) and whether duration of UC affects this association remain unclear.
What are the new findings?
Serum albumin was positively associated with MH in patients with UC. In patients with short UC duration only, high serum albumin was significantly positively associated with MH and clinical remission. In patients with long UC duration, in contrast, there was no association between serum albumin and clinical outcomes.
How might it impact on clinical practice in the foreseeable future?
In patients with short UC duration, but not those with long UC duration, serum albumin might be a useful complementary marker for MH.
Introduction
Ulcerative colitis (UC) is a chronic inflammatory bowel disease (IBD) characterised by a disease course involving relapses and remissions.1 The association between anti-tumour necrosis factor (TNF)-α monoclonal antibody treatment and long-term colectomy rate among patients with UC is still unclear.2 Accumulating evidence suggests that mucosal healing (MH) is inversely associated with relapse, surgery, hospitalisation, and long-term complications in patients with UC.3 In clinical settings, MH has been indicated as a therapeutic goal for UC. Likewise, the Selecting Therapeutic Targets in Inflammatory Bowel Disease study recommended treat-to-target strategies for patients with IBD.4 5 To maintain MH, the normalisation of serum and faecal biomarkers have been determined as short-term targets. Faecal calprotectin (FC) is the most reliable marker for MH and is therefore widely used.6 7 It requires repeated stool examination, however, which is burdensome for all patients. The prevalence and incidence of UC are reportedly increasing around the world.6 Thus, the development of an easy, rapid, repeatable, and affordable serum marker for MH is one of the unmet needs related to maintaining MH in the clinical setting. Novel biomarkers for clinical outcomes have recently been reported including serum globulin, serum indirect bilirubin, neutrophil/lymphocyte ratio, C reactive protein/albumin ratio, albumin/platelet ratio, and platelet/lymphocyte ratio.7–11 Now, we may be able to add serum albumin to this list.
Serum albumin is known as a marker of acute inflammation.12 The serum albumin test is simple, rapid, relatively non-invasive, repeatable, and affordable, and can be measured at all medical institutions. There is abundant evidence regarding the association between serum albumin and clinical outcomes in patients with UC.3 13–18 In Japanese and Norwegian studies, serum albumin was associated with clinical disease activity.13 14 In Indian, Spanish, Iranian and UK studies of patients with UC, serum albumin was inversely associated with clinical outcomes including relapse.15–17 Nevertheless, there is no evidence regarding a possible association between serum albumin and MH, although two studies showed no association between serum albumin and MH.19 20 We aimed to resolve this discrepancy by evaluating the association between serum albumin and clinical outcomes including MH and exploring whether duration of disease affected that association in Japanese patients with UC.
Materials and methods
Study population
The study subjects consisted of patients with UC treated at the Department of Gastroenterology and Metabology at the Ehime University Graduate School of Medicine, and at several affiliated hospitals in Ehime Prefecture. All patients had been diagnosed with UC according to endoscopical, radiological, histological, and clinical criteria. Consecutive outpatients and inpatients with UC who were able to understand our study were candidates. After they were informed about the study, however, some subjects did not consent to participate in the colonoscopy, blood test, and questionnaire portions of the study, while other patients had missing data. The final analysis sample in this study consisted of patients with data on endoscopy findings, duration of UC, clinical remission, body mass index (BMI), medication, C reactive protein (CRP), and serum albumin. This study protocol conforms to the ethical guidelines of the Declaration of Helsinki. Well-trained staff obtained written informed consent from all patients enrolled. The group analysed in this study was registered during the period from 2015 to 2019.
Measurements
Information on duration of UC, endoscopic findings, clinical remission, medication, serum albumin, and CRP levels were collected from medical records. Serum albumin and CRP had been measured during routine blood tests and were obtained from patient files at the time of each patient’s enrolment in in the study. Blood samples were taken in the morning after overnight fasting. Each patient’s BMI was calculated as their weight (kg) divided by the square of their height (m2). Blood examination was performed when a colonoscopy was scheduled or performed, and up to 2 months may have passed between the blood test and the colonoscopy.
Assessment of clinical remission, endoscopic activity, and MH
A charge-certified gastrointestinal endoscopist assessed all patients’ clinical symptoms. Clinical remission was defined as no rectal bleeding and no abnormally high stool frequency (<3 times per day). A certified endoscopist evaluated mucosal status by total colonoscopy. All endoscopic findings used in our analysis had been obtained within the last 6 months. In patients without endoscopic findings in the last 6 months, a new endoscopy was performed to assess mucosal status. Certified gastrointestinal endoscopists provided most of the medical reports regarding endoscopic activity. The Mayo endoscopic score (MES) classifies patients into the following four categories21: 0, normal or inactive disease; 1, mild disease with erythema, decreased vascular patterns, and mild friability; 2, moderate disease with marked erythema, absent vascular patterns, friability, and erosions; and 3, severe disease with spontaneous bleeding and ulceration. Partial MH and MH were defined as category 0–1 and 0, respectively, in this study. One endoscopy specialist who was blinded to CRP and serum albumin was responsible for evaluating MES, partial MH and MH in all patients.
Statistical analysis
Serum albumin was divided into tertiles based on its distribution among all study subjects. Serum albumin level was classified into three categories: (1) low serum albumin, <4.1 g/dL (reference); (2) moderate serum albumin, 4.1–4.4 g/dL; and (3) high serum albumin, >4.4 g/dL. Estimations of crude ORs and their 95%CIs for clinical remission, partial MH and MH in relation to serum albumin were performed using logistic regression analysis. Multiple logistic regression analyses were used to adjust for potential confounding factors. Age, sex, BMI, prednisolone use, anti-TNF-α monoclonal antibody preparation, CRP, disease extent (proctitis/non-protitis), and disease duration (<7 years/≥7 years) were selected a priori as potential confounding factors. All statistical analyses were performed using SAS software package V.9.4 (SAS Institute). A receiver operating characteristic (ROC) curve was generated, and the area under the curve was calculated to show the utility of serum albumin in indicating MH. We used Youden’s index to calculate the cut-off value of albumin. The ROC curve, cut-off value of serum albumin, sensitivity, and specificity were analysed using JMP V.14.2 software (SAS Institute). All probability values for statistical tests were two-tailed, and p<0.05 was considered statistically significant.
Results
Characteristics of patients with UC in this study
After 114 patients were excluded due to incomplete data, the final analysis sample in this study consisted of 273 patients. Table 1 shows the characteristics of the study participants. The mean age was 51 years, and the percentage of men was 59%. Mean BMI was 22.72 kg/m2. Use of 5-aminosalicylates, prednisolone, anti-TNF-α monoclonal antibody preparations and azathioprine was reported for 91.2%, 21.6%, 6.2%, and 15.5% of patients, respectively. Rates of clinical remission, partial MH (including MES 0 and 1), and MH (MES 0) were 57.9%, 63% and 26%, respectively, and the mean serum albumin level was 4.21±0.43 mg/dL.
Clinical characteristics of 273 study participants
The association between serum albumin level and clinical outcomes
Crude and adjusted ORs and 95% CIs for clinical remission and MH in relation to serum albumin level are shown in table 2. In all patients, after adjustment for age, sex, BMI, use of prednisolone, use of TNF-α monoclonal antibody preparations, CRP, disease extent, and disease duration, high serum albumin was significantly positively associated with MH (OR 2.29 (95% CI: 1.03 to 5.29), p for trend=0.043). Serum albumin level was not associated with clinical remission or partial MH. In a sensitivity analysis, only use of steroids was inversely associated with MH in all patients. CRP was not associated with MH or albumin.
Crude and adjusted ORs and 95% CIs for association between clinical outcomes and serum albumin level
Influence of disease duration on the association between albumin level and clinical outcomes
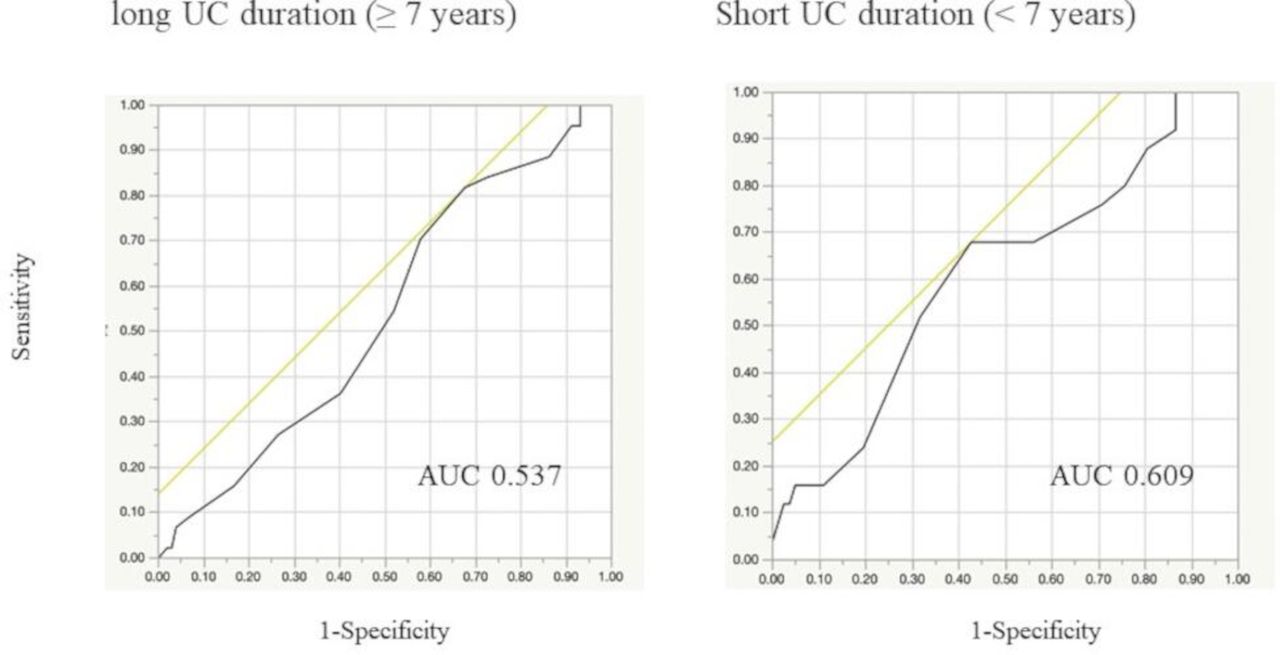
The association between serum albumin and MH in patient groups classified according to disease duration is shown in table 3. In the short-duration group (<7 years), high serum albumin was independently inversely associated with clinical remission and MH (clinical remission: adjusted OR 3.65 (95% CI: 1.05 to 13.66), p for trend=0.03, and MH: adjusted OR 6.85 (95% CI: 1.54 to 36.45), p for trend=0.005). In the long-duration group (≥7 years), these associations between serum albumin and clinical outcomes disappeared. In the short-duration group, the area under the ROC curve for serum albumin level (cut-off 4.40 g/dL) was 0.609 (figure 1).

{kind=link}
Receiver operating characteristic curve of serum albumin as a marker for mucosal healing defined as Mayo endoscopic subscore 0. The receiver operating characteristic curve of serum albumin as a marker for mucosal healing had an AUC of 0.609 in patients with short UC duration. When the cut-off serum albumin level was set to 4.40 g/dL, the sensitivity and specificity of this marker were 68% and 57.3%, respectively. In patients with long UC duration, the sensitivity and specificity were 81.8% and 32.4%, respectively (cut-off value, 4.10 g/dL), and the AUC was 0.537. We used the Youden’s Index to calculate the cut-off serum albumin values. AUC, area under the curve; UC, ulcerative colitis.
Crude and adjusted ORs and 95% CIs for the association between clinical outcomes and serum albumin level according to duration of UC
Discussion
This is the first study to show a significant positive association between serum albumin and MH in patients with UC. While serum albumin is independently positively associated with clinical remission and MH in the short-duration UC group, there was no association between serum albumin and any clinical outcome in the long-duration UC group.
Previous studies have suggested associations between serum albumin and disease activity, relapse, and colectomy in patients with UC.3 In a Japanese retrospective study of patients with UC, the prevalence of low serum albumin (<3.5 g/dL) was 35.3% in the moderately active UC group; in the mildly active UC group, on the other hand, there were no patients with low serum albumin.14 Similarly, in a Norwegian study of IBD, serum albumin was inversely related with the median Simple Clinical Colitis Activity Index, which is also used as an indicator of clinical activity of UC.15 In an Indian prospective study of 55 patients with UC, serum albumin was inversely associated with the failure of medical treatment.16 Similarly, in a Spanish cohort study of patients with UC treated with steroids, the Ho index, which includes serum albumin, was inversely associated with response to cyclosporine.17 In a UK cohort study, serum albumin was significantly lower in patients with UC who required surgery than in patients who did not.18 The findings in the present study are partially consistent with these findings in patients with UC.
There is increasing interest in the concept of ‘treat-to-target’ in IBD as a means of standardising management and preventing complications. To date, MH has been regarded as the therapeutic goal for UC.4 5 Surveillance colonoscopy is essential as a means of assessing MH regardless of clinical symptoms, but strict control based on the close monitoring of biomarkers allows patients to maintain MH.4 FC is the most reliable marker for MH and is therefore widely used. Yet it requires stool examination and repeated colonoscopy, which is burdensome for all patients, but especially for the elderly, women, adolescents, and asymptomatic patients with UC. As FC has been significantly correlated with serum albumin in Japanese, Korean, Swiss, and Canadian studies of patients with UC,22–25 serum albumin might be useful as a complementary marker for FC, especially in patients with short duration of UC. Additionally, pretreatment serum albumin level predicted response to anti-TNF treatment in 728 patients with UC.26 Monitoring serum albumin might therefore be a useful tool in UC management including acute severe UC. As serological markers might be less sensitive and less specific for intestinal inflammation compared with FC,27 however, serum albumin should be used as a complementary marker rather than as a substitute for calprotectin. We have previously found associations between platelet,28 globulin,7 and bilirubin8 values and clinical outcomes including MH, though the sensitivity and specificity of these serum markers for clinical outcomes was not sufficiently high to justify using any of them alone. To assess MH using serum markers only, combinations of these markers should be studied in the future.
The mechanism underlying the link between serum albumin and MH remains unclear, but there are several biologically plausible options. Inflammation in the intestine might injure the vascular endothelium, permit leakage from the mucosa, and suppress the synthesis of albumin in the liver.29 In 43 patients with UC, CRP was significantly inversely associated with serum albumin.30 Associations have likewise been reported between plasma TNF-α levels and serum albumin levels in community-dwelling Japanese elderly women.31 Intestinal tract inflammation might lower serum albumin in patients with active UC.
Only a few studies have explored the influence of disease duration on biomarker accuracy in patients with IBD. In patients with Crohn’s disease, disease duration did not affect the utility of FC as a biomarker.32 In patients with UC, the immunochemical faecal occult blood test is a more accurate biomarker for MH when disease duration is <4 years.33 In this study, likewise, there was a positive association between serum albumin and MH only in patients with short duration of disease. A higher frequency of bleeding is also observed in patients with shorter disease duration,33 while long disease duration with chronic inflammation is associated with higher frequencies of intestinal fibrosis33 and malnutrition. Differences in rates of bleeding, fibrosis, and malnutrition between patients with short-duration and long-duration UC might affect the association between serum albumin and clinical outcomes. However, it remains uncertain why UC duration affects the association between serum albumin and MH.
Our study has several limitations. First, as this was a cross-sectional study, we cannot confirm that there is a causal relationship between serum albumin levels and MH. Future longitudinal studies and intervention studies are needed to confirm the association between changes in albumin levels and endoscopic findings. Second, the extended interval between some participants’ colonoscopies and their blood tests may have resulted in misclassification. Third, it is likely that most of the patients in this cohort had been receiving anti-inflammatory treatment for a considerable time. Long-term treatment with medications such as prednisolone might promote MH and change serum albumin levels. Long-term treatment might also obscure the association between serum albumin and MH. Fourth, patients with other diseases that can lower serum albumin levels, such as liver cirrhosis, and renal dysfunction, were not excluded from this study. Fifth, although FC is a reliable marker of MH, we could not measure FC in this cohort. Sixth, we did not perform an independent, completely blinded, central evaluation of the endoscopic findings. Finally, the patients in the present study are likely not representative of all patients with UC in Japan. Nevertheless, their median age, male:female ratio, and rates of biological, prednisolone, 5-aminosalicylate, and thiopurine use (51 years, 59%, 6.2%, 21.6%, 91.2%, and 15.5%, respectively) were similar to those in a Japanese national study based on 2016 UC claims data (44 years, 63.9%, 9%, 15.5%, 96.2%, and 13.8%, respectively).34 Further research is warranted to evaluate the association between serum albumin and clinical outcomes in other cohorts of patients with UC. In particular, more investigation into the relationship between biomarker accuracy and disease duration is warranted.
In conclusion, serum albumin may be independently positively associated with MH in Japanese patients with UC. In short-duration patients with UC, serum albumin might be useful as a complementary marker for MH.
Supplemental material
Data availability statement
Data are available upon reasonable request. The data sets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics statements
Ethics approval
This research was approved by the institutional review board of the Ehime University Graduate School of Medicine (#1505011). All patients provided written informed consent before enrolment.
Acknowledgments
The authors would like to acknowledge Keiko Kikuchi, Masumi Hino, Keitarou Kawasaki, Yuji Mizukami, Masayoshi Uraoka, Satoshi Imamine, Sanae Nakamura, Harumi Yano, Makoto Yano, Masato Murakami, Masamoto Torisu, Kanako Konishi and Tomoe Kawamura for their support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
SY and SF are joint first authors.
SY and SF contributed equally.
Contributors SF, ET, YI and YHi contributed to the study conception and design. Material preparation and data collection were performed by SY, SF, KS, YHa, KT, KM, TN, SS, NS, HM, KO, AH, HT, YY, ET and YI. Data analysis was performed by SF. The first draft of the manuscript was written by SY and SF and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.