Article Text

Abstract
Introduction Exercise is emerging as a therapy in oncology for its physical and psychosocial benefits and potential effects on chemotherapy tolerability and efficacy. However, evidence from randomised controlled trials (RCTs) supporting exercise in patients with borderline resectable or locally advanced pancreatic cancer (PanCa) undergoing neoadjuvant therapy (NAT) are lacking.
Methods and analysis The EXPAN trial is a dual-centre, two-armed, phase I RCT. Forty patients with borderline resectable or locally advanced PanCa undergoing NAT will be randomised equally to an exercise intervention group (individualised exercise+standard NAT) or a usual care control group (standard NAT). The exercise intervention will be supervised and consist of moderate to vigorous intensity resistance and aerobic-based training undertaken two times a week for 45–60 min per session for a maximum period of 6 months. The primary outcome is feasibility. Secondary outcomes are patient-related and treatment-related endpoints, objectively measured physical function, body composition, psychological health and quality of life. Assessments will be conducted at baseline, prior to potential alteration of treatment (~4 months postbaseline), at completion of the intervention (maximum 6 months postbaseline) and 3-month and 6-month postintervention (maximum 9 and 12 months postbaseline).
Ethics and dissemination The EXPAN trial has been approved by Edith Cowan University (reference no.: 2020-02011-LUO), Sir Charles Gairdner Hospital (reference no.: RGS 03956) and St John of God Subiaco Hospital (reference no.: 1726). The study results will be presented at national/international conferences and submitted for publications in peer-reviewed journals.
Trial registration number ACTRN12620001081909.
- pancreatic cancer
- alternative medicine
- chemotherapy
- surgical resection
- quality of life
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
INTRODUCTION
Advances in neoadjuvant therapy (NAT) and surgical techniques for pancreatic cancer (PanCa) have improved the likelihood of patients with borderline resectable or locally advanced disease undergoing curative-intent surgery.1 2 However, rates of operability and margin-negative (R0) resection remain low for patients with borderline resectable (operability: 69%, R0: 54%) or locally advanced (operability: 26%, R0: 23%) PanCa after NAT (based on various pre-NAT resectability criteria)3 due to poor response to current regimens. This may be due to the complex microenvironment of PanCa characterised by a high percentage of tumour stroma that leads to dysfunction in nearby blood vessels and impedes drug delivery to tumour cells.4 In addition, dose reductions, dose delays and reduced relative dose intensity (RDI) are common in these patients during NAT due to dose-limiting toxicities (such as fatigue, neutropenia, vomiting and diarrhoea),5 6 which can also contribute to reduced therapeutic response.7
Patient physical condition is an important consideration before proceeding to PanCa surgery.2 8 However, patients with PanCa are relatively older (median age 71 years)2 and are at high risk of developing debilitating syndromes including sarcopaenia and cachexia.9 These factors along with cumulative toxicities of NAT can worsen patients’ preoperative condition and, in turn, increase risk of complications and prolonged recovery after surgical resection, ultimately impairing their long-term survival.10 11 Further, side effects relating to PanCa and its treatments have a negative impact on patients’ psychological health and quality of life (QoL).12 13 Given the suboptimal responses to current NAT and the extensive treatment-related side effects in patients with borderline resectable or locally advanced PanCa, research into interventions to address these unmet needs is of clinical importance.
Exercise has been recommended as an effective therapy for persons following a cancer diagnosis in managing fatigue, psychological distress, muscle loss and declines in physical function and QoL.14 15 Of importance, there is early evidence suggesting that exercise may serve as a potential strategy to improve chemotherapy tolerability.16 17 Further, preclinical and clinical trials (including a trial in patients with PanCa) suggest that exercise normalises tumour vasculature, which in turn may lead to augmented efficacy of chemotherapy via increasing drug delivery.18–21 Despite the benefits associated with exercise in cancer management, only seven exercise trials have been undertaken in patients with PanCa with over half being case reports or a case series.22–24 Although a recent systematic review by our team found that exercise may be safe and feasible in patients with PanCa,24 most of the patients enrolled in the studies were highly selected having already successfully completed NAT and surgical resection. Additionally, a case series25 and a case report26 of patients with borderline resectable or locally advanced PanCa during NAT performing supervised exercise training showed promising results that warrant further investigation with a more rigorous study design. Therefore, we propose to undertake a pilot randomised controlled trial (RCT) to examine the feasibility and efficacy of a supervised, multicomponent exercise programme in patients with borderline resectable or locally advanced PanCa undergoing NAT.
Methods and analysis
In this manuscript, we describe the rationale and design considerations of the EXPAN trial. The protocol was developed and reported according to the SPIRIT (Standard Protocol Items: Recommendations for Interventional Trials) guidelines.27
Study design
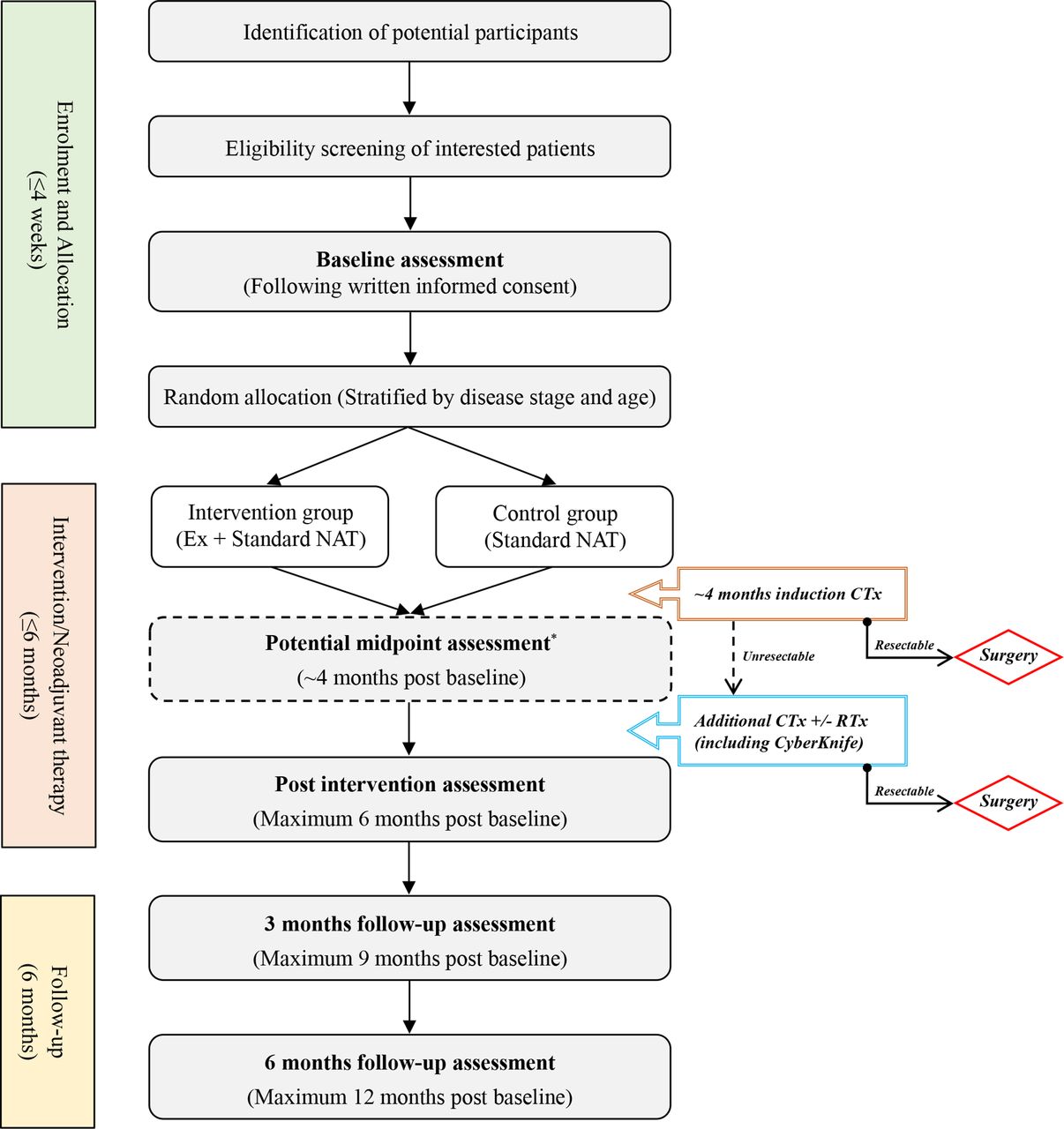
The study design and a schematic schedule for enrolment, intervention and assessments of the EXPAN trial is outlined in figures 1 and 2, respectively. The EXPAN trial is a dual-centre, two-armed, phase I RCT to examine the feasibility and efficacy of a supervised, multicomponent exercise medicine programme in patients with borderline resectable or locally advanced PanCa undergoing NAT. Following completion of eligibility screening, informed consent and baseline assessment, recruited patients will be randomised equally to an intervention group (individualised exercise training concomitant with standard NAT) or a usual care control group (standard NAT). Participants will undergo additional assessments at completion of the intervention (maximum 6 months postbaseline), 3-month and 6-month postintervention (maximum 9 and 12 months postbaseline). For participants who will undergo additional chemotherapy with or without radiation (including CyberKnife) after induction chemotherapy, a midpoint assessment will be performed before the alteration of treatment (~4 months postbaseline).

Flowchart of study design. *Only for participants who are unresectable and will undergo additional chemotherapy with or without radiation (including CyberKnife) after induction chemotherapy. CTx, chemotherapy; Ex, exercise intervention; NAT, neoadjuvant therapy; RTx, radiotherapy.

{kind=link}
{kind=link}
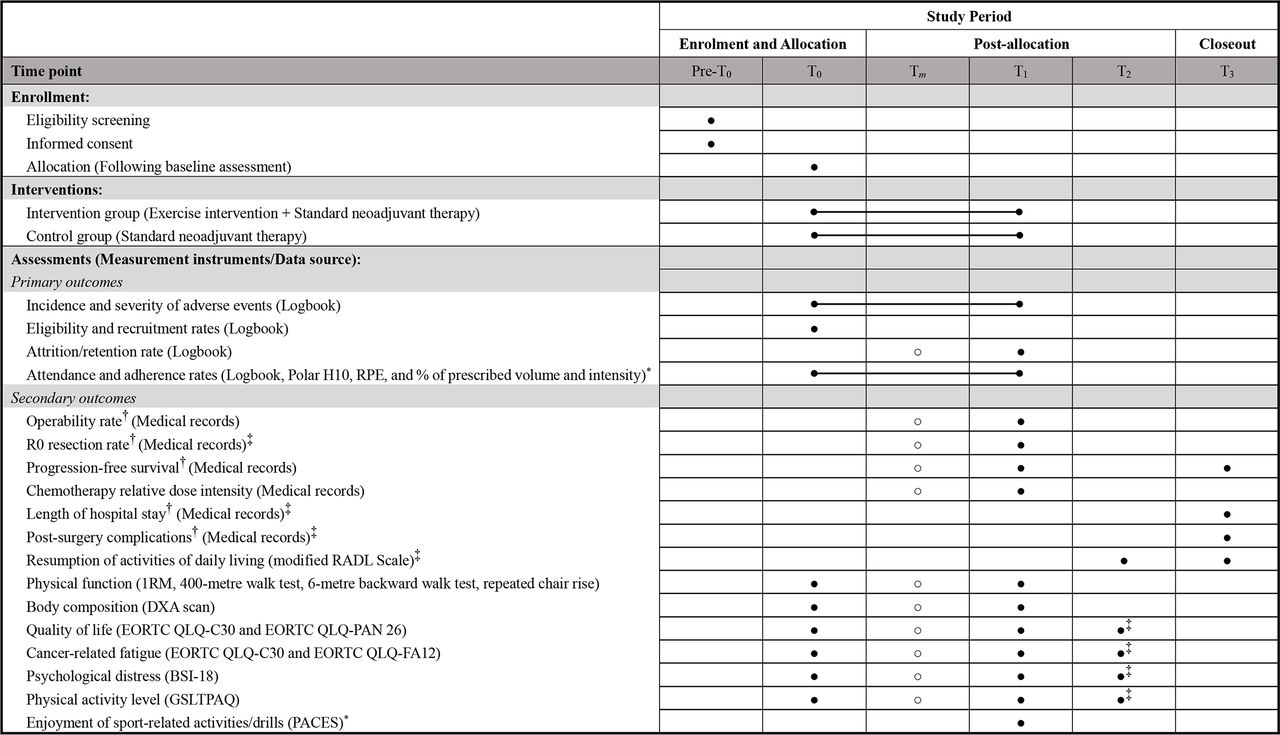
SPIRIT schematic schedule of enrolment, interventions and assessments for the EXPAN trial. ●: fixed assessment time points; ○: potential assessment time point. *Only for the intervention group. †Measured in line with routine clinical examination of the hospitals with the data collected closest to the predefined assessment time points (ie, Tm, T1 and T3) used for the EXPAN trial. ‡Only for participants receiving pancreatic cancer surgery. BSI-18, Brief Symptom Inventory-18; DXA, dual X-ray absorptiometry; EORTC QLQ, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire; GSLTPAQ, The Godin-Shephard leisure-time physical activity questionnaire; 1 RM, 1-repetition maximum; PACES, physical activity enjoyment scale; RADL, resumption of activities of daily living; RPE, the rating of perceived exertion (the 10-point Borg Scale); T0, baseline; Tm, potential midpoint (~4 months postbaseline); T1, at completion of the exercise intervention (maximum 6 months postbaseline); T2, 3 months after T1 (maximum 9 months postbaseline); T3, 6 months after T1 (maximum 12 months postbaseline).
Eligibility criteria
Men and women diagnosed with borderline resectable or locally advanced pancreatic ductal adenocarcinoma as per the Australasian Gastro-Intestinal Trials Group definition (AGITG)28 will be invited to participate in the study. Major inclusion and exclusion criteria are as follows:
Inclusion criteria
Age ≥18 years.
Waiting to start or within 4 weeks after starting their prescribed neoadjuvant chemotherapy with or without locoregional radiotherapy.
Approved by their treating oncologist to participate in the trial.
Exclusion criteria
Recurrent PanCa with or without exposure to previous chemotherapy.
Having undergone treatments for another primary cancer within the last 12 months, or another ongoing active primary malignancy.
Anticipating undergoing major surgery for non-cancer diseases within the next 6 months.
Any musculoskeletal, cardiovascular or neurological disorder that could put them at risk during exercise testing and training.
Having participated in planned, individualised and supervised exercise training for ≥2 days/week in the previous month.
Unable to travel to any designated training and/or testing site.
Sample size
Given the pilot nature of the EXPAN trial investigating primarily the safety and feasibility of the exercise intervention in patients with PanCa during NAT, no formal sample size calculation was performed a priori. However, according to the study clinicians, the number of participants that is viable over a 12-month recruitment period in the participating hospitals would be approximately 40 (ie, 20 per group). This has been reported to be an acceptable sample size for a pilot RCT (ie, 12–35 persons per group).29–31
Recruitment
The EXPAN trial will receive support for recruitment from the Multidisciplinary Team in Upper Gastrointestinal Cancers at Sir Charles Gairdner Hospital (SCGH) and St John of God Subiaco Hospital (SJOGSH). Participants will be recruited using the following methods: (1) The study investigator reviews electronic clinical notes at SJOGSH every 2 weeks to initially identify potential participants. Subsequently, the attending oncologist or clinical nurse is asked for confirmation of their clinical eligibility and permission to contact. (2) The attending oncologists or clinical nurses at both hospitals identify clinically eligible patients and inform them about the study. Should patients express an interest in the study and provide permission, their contact details will be passed to the study investigator. On obtaining permission to contact potential participants in either way, the investigator will approach them by telephone to discuss all aspects involved with the study and perform eligibility screening. Patients who meet the eligibility criteria and are interested in the study will then be invited to participate and will be provided with a set of recruitment documents and questionnaires via post, email, fax or Microsoft Forms (for questionnaires) as appropriate. They will be advised to provide written informed consent before the baseline assessment.
In addition, participants will be recruited through advertisement posting on the website of the Exercise Medicine Research Institute (EMRI) at Edith Cowan University (ECU). Interested patients can contact the study investigator via phone or email for further information regarding the EXPAN trial.
Randomisation and blinding
After completion of the baseline assessment, participants will be randomly allocated on a 1:1 basis to an exercise intervention group or a usual care control group using a random allocation sequence generated by a secure website, Sealed Envelope (London, UK).32 The randomisation will be stratified by participants’ disease stage (borderline resectable vs locally advanced) and age (<65 years vs ≥65 years) to account for variations in historical operability rate following standard NAT in the hospitals. Random permuted blocks (block size 2 and 4) will be employed to ensure balanced allocation of participants into both groups. Assessors of the efficacy outcomes and participants’ treating oncologists will be blinded to group allocation. Due to the nature of the exercise intervention, participants will not be blinded to intervention assignment following randomisation. However, they will be required not to reveal their group allocation to the assessors and their treating oncologists.
Intervention
An overview of the exercise intervention is provided in table 1. The exercise program is scheduled for a maximum period of 6 months, which will be terminated prior to potential surgical resection. Participants in the intervention group will undertake individually tailored exercise training in any of the three ECU affiliated exercise clinics/facilities that covers different areas of the city. They will be required to exercise at a frequency of two sessions per week with 45–60 min/session (including a 5 min warm-up and cool-down). In each session, participants will perform 20–30 min of resistance training and a maximum 20 min of aerobic-based exercise (continuous cycling or intermittent sport-related activities). All the prescribed exercise components in a session will be performed in a one-to-one fashion or in a small group depending on participants' training schedule or availability and closely supervised by the investigator. The exercise programme will follow the principle of progressive overload and autoregulated based on a participant’s perceived readiness for training at the start of an exercise session. Given that participants will be exercising during NAT, a flexible training schedule will be adopted to accommodate individual treatment schedule. In addition, participants who are absent from a session will be followed up via phone and encouraged to make up for a missed session anytime in the same week (ie, during daytime on weekdays and weekends).
Overview of the exercise programme
Resistance training
Resistance training will involve 4–6 exercises that cover the major muscle groups of the upper-body and lower-body using machines and dumbbells (such as overhead press, latissimus pull-down, chest press, seated row, leg press and leg curl). For each exercise, participants will perform 1–3 sets at 8–12 repetition maximum with 60 s recovery between sets. The weight will be increased by 5%–10% when a participant can successfully complete two additional repetitions on the last set of an exercise for two consecutive sessions.33 A similar resistance training regimen has been tested and shown to be acceptable in patients following PanCa surgery.34
Aerobic-based exercises
In addition to resistance training, each session includes a maximum of 20 min of either continuous cycle ergometer exercise or intermittent sport-related activities (such as repeated punches thrown and agility ladder drills), which will be alternated from session to session to provide greater variety and training stimulus. Exercise intensity will be manipulated from ~65% to 80% of estimated maximum heart rate (MHR) (MHR=220-age), corresponding to a rating of perceived exertion (RPE) of 4–6 (Moderate to Hard) on the 10-point Borg Category-ratio scale.35 For continuous cycling, participants will be required to pedal at a cadence of 50–80 rpm.36 The pedalling resistance and speed will be progressed to elicit the target heart rate zone or RPE. With regard to the intermittent component, 3–8 bouts of 30–60 s sport-related drills will be performed with 60 s rest intervals between adjacent bouts. A similar work-to-rest ratio has been administrated in patients with cancer undergoing chemotherapy.37
Controls
After completion of the baseline assessment and randomisation, the study investigator will advise the controls to maintain their usual activities. No exercise prescriptions or recommendations will be provided to them. To capture information concerning leisure-time exercise undertaken incidentally in the controls, a pre-established physical activity log will be provided to them. In addition, the study investigator will contact the controls via phone once per month to facilitate data collection relating to incidental exercise, potential adverse events (AEs) and any changes in cancer treatment.
Treatment of exocrine pancreatic insufficiency
All study participants will be prescribed Creon (pancrelipase delayed-release capsules) for the treatment of potential exocrine pancreatic insufficiency.
Data collection
Primary outcome
Feasibility metrics
Incidence and severity of AEs (defined as unfavourable responses to exercise and NAT undertaken as part of the EXPAN trial but may not necessarily be related to these treatments) will be tracked by the study investigator and participants, and identified through review of medical records. Specifically, the occurrence of AEs during and following an exercise session will be captured by the study investigator or participants using a pre-established tracking log. Any NAT-related AEs will be actively monitored by clinicians and obtained via medical records after completion of the intervention. The severity of AEs will be graded using the National Cancer Institute’s Common Terminology Criteria for Adverse Events (CTCAE, V.5.0).38
Eligibility rate will be calculated by dividing the number of eligible patients by the number of patients screened; recruitment rate will be calculated by the number of enrolled patients versus the number of eligible patients. We will assess eligibility and recruitment rate at baseline. The number of excluded and unenrolled patients will be documented along with the relevant reasons by the study investigator.
Attrition rate will be determined by the number of dropouts in each group versus the number originally allocated and assessed prior to the potential alteration of treatment and at completion of the exercise intervention. Reasons for dropping out will be documented by the study investigator.
Attendance rate will be determined by the total and weekly number of exercise sessions attended versus the number of sessions prescribed (only for the intervention group). Reasons for non-attendance will be documented by the study investigator.
Adherence rate will be determined by the number of sessions where the prescribed resistance and aerobic-based exercises are successfully completed (including volume and intensity) versus the number of sessions attended (only for the intervention group). A combination of exercise heart rate (tracked by Polar H10), RPE (10-point Borg scale) and duration will be used to monitor activity profile for aerobic-based exercises. Adherence to resistance training will be assessed by calculating the amount of exercise actually completed (ie, the number of exercises, sets, repetitions and weights) and comparing to the individual prescribed exercise in each session.39 Reasons for non-adherence to an exercise prescription will be documented by the study investigator.
Secondary outcomes
Patient-related and treatment-related endpoints
Rates of operability and R0 resection will be evaluated in line with routine clinical examinations at the hospitals with the latest data collected prior to potential alteration of treatment and at completion of the exercise intervention used for the EXPAN trial. Operability rate refers to the proportion of participants who achieve anatomical resectability status as defined by the AGITG28 and proceed to PanCa surgery; R0 resection rate is defined as proportion of participants who undergo tumour resection with a clear margin (>1 mm). The data will be extracted from participants’ medical records.
Progression-free survival (PFS) will be assessed in line with routine clinical examinations at the hospitals with the latest data collected prior to potential alteration of treatment, at completion of the exercise intervention and 6 months post the exercise intervention used for the EXPAN trial. In this study, PFS is defined as the length of time elapsed from the start of the exercise intervention/postrandomisation to an indication of disease progression or death from any cause. The data will be obtained via participants’ medical records.
Chemotherapy RDI will be examined prior to potential alteration of treatment and at completion of the exercise intervention. RDI is determined by the ratio of actually delivered dose (mg/m2/week) against the planned dose (mg/m2/week) of a regimen. For participants receiving a multiple-drug regimen, the RDI for each drug and average RDI across all drugs included in the regimen will be calculated. The data will be extracted from participants’ medical records along with any documented reasons for regimen delay, change and discontinuation.
Length of hospital stay (LOS) will be assessed in line with routine clinical examinations at the hospitals in participants who receive PanCa surgery. In this study, LOS is defined as the duration of a single episode of hospitalisation between the day completing surgical resection and the day being discharged from the hospital. The data will be obtained through participants’ medical records at 6 months post the exercise intervention.
The incidence and severity of postsurgery complications will be assessed in line with routine clinical examinations at the hospitals in participants who undertake PanCa surgery. We will use the Clavien-Dindo classification to define and grade the severity of surgical complications.40 The data will be obtained via participants’ medical records at 6 months post the exercise intervention.
Resumption of activities of daily living in participants following surgical resection will be assessed at 3-month and 6-month postexercise intervention using a self-administrated questionnaire. The questionnaire is a 12-item Likert-scale used to rate the degree to which the participants have resumed their usual activities of daily living.41
Physical function
Physical function will be measured at baseline, prior to potential alteration of treatment, and at completion of the exercise intervention using a battery of standard tests that are as follows:
One-repetition maximum (1RM) chest press and leg press test is performed to assess muscle strength of major muscle groups in the upper-body and lower-body, respectively.42 The chest press test is conducted on a Cybex chest press machine (Cybex International, Medway, Massachusetts, USA) and leg press on a Cybex leg press machine. Following a general warm-up, participants undertake two specific warm-up sets of eight and three repetitions at approximately 50% and 70% of an estimated 1 RM, respectively. Subsequently, single repetitions are performed with progressively heavier weights until failure. The final weight lifted successfully is recorded for analysis. To avoid unnecessary fatigue, three to five trials are attempted and a rest interval of 1–2 min is given between trials.
Repeated chair rise test is used to evaluate lower-limb muscle function.43 To perform the test, participants sit on a hard-backed chair (seat height 43 cm from the floor) with their arms folded across their chest. They are instructed to rise as fast as possible to a full standing position and then return to a full sitting position five times. Three trials are performed with a 1 min recovery between trials. The fastest time recorded will be used in the analysis.
Four hundred metre walk test is administrated to measure cardiorespiratory fitness and walking endurance.43 The test requires participants to walk 400 m in a hallway back and forth on a 20 m course as fast as possible. The time taken to complete the 400 m walk will be used in the analysis.
Six-metre backwards tandem walk is undertaken to examine dynamic balance.44 Participants are required to walk backwards in tandem stance (ie, placing one foot directly behind the heel of the other with the shoes touching) for a distance of 6 m. The time taken to complete the distance is recorded for analysis.
Body composition and anthropometry
Whole body lean mass, fat mass and percentage body fat will be assessed at baseline, prior to potential alteration of treatment and at completion of the exercise intervention using dual-energy X-ray absorptiometry (DXA; Horizon A, Hologic, Waltham, Massachusetts, USA).45 In addition, body height and weight will be obtained using a digital measuring station (SECA 763; seca gmbh & co. kg., Hamburg, Germany) and waist and hip circumference using a constant tension tape measure.
Quality of life and psychological health
The European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire Core module (QLQ-C30)46 and the pancreatic cancer specific module (QLQ-PAN26)47 will be used to assess QoL. To assess cancer-related fatigue, the EORTC QLQ-C30 with the addition of a validated 12-item fatigue module (QLQ-FA12) by the EORTC48 will be administered. Psychological distress will be measured using the Brief Symptom Inventory-18.49 These questionnaires will be completed by participants at baseline, prior to potential alteration of treatment and at completion of the exercise intervention. For participants who undergo PanCa surgery, they will also complete these questionnaires at 3 months post the exercise intervention.
Physical activity level
Self-reported physical activity level will be assessed using the Godin-Shephard Leisure-Time Physical Activity Questionnaire50 at baseline, prior to potential alteration of treatment and at completion of the exercise intervention. For participants who receive PanCa surgery, they will also complete the questionnaire at 3 months post the exercise intervention.
Enjoyment of sport-related activities
To explore participants’ views on intermittent sport-related activities provided in the intervention, the intervention group will be asked to complete a modified Physical Activity Enjoyment Scale (PACES)51 at completion of the exercise intervention.
Statistical analysis plans
Statistical analyses will be performed using SPSS 26.0 (IBM, Chicago, Illinois, USA) and R V.4.0.2 (https://www.r-project.org/). Descriptive statistics will be used for baseline demographic and clinical characteristics of each group. Categorical variables will be presented as frequencies and proportions, and continuous variables will be presented as means and SDs (or medians and IQR). Between-group differences in baseline characteristics will be assessed using independent t-tests or the Mann-Whitney U test, as appropriate, for continuous data and the χ² test for categorical data.
The feasibility endpoints will be analysed descriptively and reported as frequencies and/or proportions. The differences between the intervention and control group in changes over time for efficacy outcomes (excluding LOS and PFS) will be assessed using linear mixed models or generalised linear mixed models with a random-effect factor for patients. Fixed-effect factors associated with secondary outcomes of interest include intervention assignment, time and an intervention by time interaction as well as actually completed dosage of the exercise intervention and NAT. Analysis of LOS will be conducted using zero-truncated negative binomial regression. With regard to the analysis of PFS, the Kaplan-Meier method with log-rank test will be used. The number of participants with disease progression within the study period (ie, maximum 12 months) and the number of censored patients will be presented. In addition, the Cox proportional hazards regression model will be used to estimate the hazard ratio between the study arms. The intention-to-treat principle will be applied to the efficacy outcomes analysis. The use of radiotherapy and choice of chemotherapy drugs in participants will be adjusted as potential confounding factors for the exercise intervention effects. All between-group differences will be reported using the 95% CI. Further analysis of the association between body composition and chemotherapy RDI at different time points will be performed using linear regression or generalised linear regression. Tests will be two-tailed and p≤0.05 will be considered statistically significant.
Monitoring
Monitoring of the EXPAN trial will be performed through regular study progress reports review (6-month to 12-month intervals) by the ECU Research Ethics Team (RET) and the respective RET or Research Governance Office (RGO) for SCGH and SJOGSH. This is in line with the current Australian Code for the Responsible Conduct of Research.52 The research team of the EXPAN trial is also responsible for monitoring. A summary of exercise-related AEs (if any) will be provided to the participants’ treating oncologists every 4 weeks. If there is any indication that the exercise intervention is causing harm, a case-by-case analysis will be conducted by the research team before stopping or modifying the intervention for a participant. In addition, the research team will report to the RETs and RGOs immediately in the event of a serious AE (≥Grade 3 in the CTCAE).
Ethics and dissemination
Ethics approval
The research ethics of the EXPAN trial was reviewed and approved by the respective Human Research Ethics Committee at ECU (reference no.: 2020–02011-LUO) and the participating hospitals in Perth, Australia, including SCGH (reference no.: RGS 03956) and SJOGSH (reference no.: 1726). The trial was registered with the Australian New Zealand Clinical Trials Registry (ANZCTR) on 20 October 2020 (ID: ACTRN12620001081909).
Protocol amendments
Any changes to the research protocol that may affect the conduct of the EXPAN trial, and the safety and potential benefits of participants (such as study design, eligibility criteria, outcome measures and analysis methods) require a substantive protocol amendment. Such amendment will be agreed on within the research team and communicated timely to the involved RET/RGO through their required review procedure, and approval will be obtained before implementation. In addition, protocol modifications will be tracked in the ANZCTR.
Confidentiality
On recruitment, each participant is assigned a unique identification number. During the trial, individually identifiable data/information will be deidentified with the number immediately after collection. As required by the ECU Data Management Plan, hard-copy records (eg, paper-based questionnaires) will be kept in a separate lockable filing cabinet; digital data will be stored on a password-protected computer and uploaded to a SharePoint site that is exclusive to the EXPAN trial. All the study data/information will only be accessible to the study personnel. In accordance with the current Australian Code for the Responsible Conduct of Research,52 the data/information collected for the EXPAN trial will be stored for at least 15 years following completion of the study. After the minimum storage duration, all study data/information will be permanently destroyed in an appropriate way.
Dissemination plan
Research outcomes of the EXPAN trial will be presented at national and international academic conferences and submitted for publication in peer-reviewed journals. In addition, to facilitate participant retention in the trial, a summary of individual results will be provided (on request) to those who complete the study. The report will outline individual results on body composition, muscle strength, functional capacity, psychological health and QoL at each time point and changes across all assessment time points.
Discussion
The understanding of the role of exercise in patients with PanCa and in particular for those during NAT is limited due to their under representation in exercise oncology research. To date, there are only seven individual published studies focusing exclusively on patients with PanCa.22–24 Of them, only three studies (all without control) have been conducted in patients during NAT (including one single-arm study,53 one case series25 and one case report.26 In addition, among the ongoing exercise trials for patients with PanCa in ClinicalTrial.gov, ANZCTR and CENTRAL, with the exception of the EXPAN trial, there is only one RCT over the course of preoperative therapy.54 In this context, additional rigorous research is required to support the use of exercise in patients with PanCa undergoing NAT.
The EXPAN trial is designed to investigate primarily the feasibility of a supervised, multicomponent exercise medicine programme in patients with borderline resectable or locally advanced PanCa undergoing NAT. The study will also provide indications of efficacy of the intervention on a wide range of clinical, physical and psychosocial endpoints. This is the first randomised controlled exercise trial specifically for patients with PanCa in Australia and is a collaborative research project between EMRI-ECU and high-volume hospitals for PanCa in Western Australia (ie, SCGH and SJOGSH).
The EXPAN intervention takes into account common perceived barriers and facilitators to exercise in patients with PanCa. Qualitative and quantitative research in this patient group found that lack of motivation is among barriers to exercise, while a supportive environment and enjoyable activities may improve exercise uptake.55 56 To this end, an exercise intervention containing sport-related activities may be a potential strategy for the patients providing an interactive and enjoyable environment.57 As a result, a multicomponent programme consisting of clinical-based resistance and aerobic exercises and adapted sport activities will be adopted given the promising results in patients with PanCa undergoing NAT through a combined exercise programme.24 An exercise intervention of this format has recently been shown to be safe and effective in maintaining physical activity for patients with sedentary breast cancer during adjuvant chemotherapy.58
Given the feasibility nature of the EXPAN trial, its results will be used to determine whether a subsequent fully powered RCT is needed. In addition, it will be an important basis for research into whether exercise can be implemented as a safe and efficacious component in a multidisciplinary management strategy for patients with PanCa or peripancreatic malignancies treated with comparable procedures (such as ampullary and periampullary).
Data availability statement
No data are available.
Ethics statements
References
Footnotes
Contributors HL conceptualised and designed the study and developed the first draft of the manuscript. DAG, RUN, CT and DRT conceptualised and designed the study and critically revised the manuscript. AD, KJ, MJ, IY and NS critically reviewed and edited the manuscript. CT, AD, KJ, MJ and IY will assist in recruitment and provide consultation on clinical data collection. All authors read and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.