Article Text

Abstract
Objectives Transjugular intrahepatic portosystemic stent shunt (TIPSS) is clinically effective in variceal bleeding and refractory ascites; however, the cost-effectiveness of TIPSS has yet to be evaluated in the UK. This study aimed to establish the cost-effectiveness of (i) pre-emptive TIPSS versus endoscopic band ligation (EBL) in populations with variceal bleeding and (ii) TIPSS versus large volume paracentesis (LVP) in refractory ascites.
Methods A cost-utility analysis was conducted with the perspective including healthcare costs and quality-adjusted life years (QALYs). A Markov model was constructed with a 2-year time horizon, health states for mortality and survival and probabilities for the development of variceal bleeding, ascites and hepatic encephalopathy. A survival analysis was conducted to extrapolate 12-month to 24-month mortality for the refractory ascites indication. Uncertainty was analysed in deterministic and probabilistic sensitivity analyses.
Results TIPSS was cost-effective (dominant) and cost saving for both indications. For variceal bleeding, pre-emptive TIPSS resulted in 0.209 additional QALYs, and saved £600 per patient compared with EBL. TIPSS had a very high probability of being cost-effective (95%) but was not cost saving in scenario analyses driven by rates of variceal rebleeding. For refractory ascites, TIPSS resulted in 0.526 additional QALYs and saved £17 983 per patient and had a 100% probability of being cost-effective and cost saving when compared with LVP.
Conclusions TIPSS is a cost-effective intervention for variceal bleeding and refractory ascites. TIPSS is highly cost-saving for refractory ascites. Robust randomised trial data are required to confirm whether pre-emptive TIPSS is cost saving for variceal bleeding.
- cost-effectiveness
- economic evaluation
- bleeding
- ascites
- liver cirrhosis
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known about this subject?
Pre-emptive transjugular intrahepatic portosystemic stent shunt (TIPSS) is considered to be clinically effective versus endoscopic band ligation (EBL) plus drug therapy in patients with cirrhosis and variceal bleeding who are haemodynamically stable. TIPSS is also clinically effective versus large volume paracentesis (LVP) plus human albumin in the management of patients with cirrhosis and refractory ascites.
Robust economic analysis with regard to use of TIPSS for these clinical indications is lacking.
What are the new findings?
Economic modelling, using methodology endorsed by National Institute for Health and Care Excellence (NICE), found that pre-emptive TIPSS was likely to be cost-effective in patients with cirrhosis and variceal bleeding versus treatment with EBL and beta blockers. However, there are high levels of uncertainty as to whether TIPSS is cost-saving in the context of the National Health Service (NHS).
TIPSS was cost-effective as well as cost saving when compared with LVP plus albumin in patients with cirrhosis and refractory ascites. Substantial cost savings to the NHS are forecast from a reduced need for continued LVP sessions to drain ascitic fluid.
How might it impact on clinical practice in the foreseeable future?
The evidence from this study supports the continued use of TIPSS in patients with cirrhosis and refractory ascites. Further well-conducted multicentre trials are required to confirm the cost saving potential of TIPSS for the variceal bleeding indication.
These results could be used to revise recommendations made by commissioners and inform regulators, such as NICE and NHS England.
Background
Cirrhosis of the liver imposes a substantial and increasing health burden being responsible for 2.4% of all deaths in the UK.1 The NHS cost of liver disease were forecast to exceed £1 billion in 2015–2016.2 The majority of the clinical and economic burden in cirrhosis occurs in patients with decompensated cirrhotic disease, the most common clinical manifestations of which are recurrent variceal bleeding and recurrent and refractory ascites (RA).3 Both variceal bleeding and RA are associated with significant impairment in length and quality of life.4–6
Treatment options for variceal bleeding and ascites include endoscopic band ligation (EBL) and large-volume paracentesis (LVP), respectively. Both indications can also be managed by transjugular intrahepatic portosystemic stent shunt (TIPSS). TIPSS procedures were originally conducted using bare metal stents, but these had relatively poor patency, requiring re-interventions and are associated with an increase in the incidence of hepatic encephalopathy (HE).7 Clinical outcomes have improved since the early 2000s following the introduction of expanded polytetrafluoroethylene (ePTFE) covered stents.7–9
When compared with EBL, randomised controlled trial (RCT) evidence indicates TIPSS with an ePTFE covered stent is likely to be clinically effective if delivered as a pre-emptive procedure in populations with haemodynamically stable variceal bleeding. Conclusive RCT evidence has identified increased survival and reduced cirrhosis related adverse event rates for TIPSS vs LVP in RA populations.10 11 Such findings informed UK clinical guidelines which recommend TIPSS with covered stents for the management of variceal bleeding and RA in these patient populations.12 13
While TIPSS improves health morbidity and mortality, the procedure incurs substantial healthcare costs and is delivered to populations with relatively severe disease and poor long-term prognosis.10 11 It is questionable whether TIPSS offers value for money when compared with other interventions that could be funded within the budget constrained UK health sector. There is a paucity of evidence establishing the cost-effectiveness of TIPSS with ePTFE covered stents for variceal bleeding and RA in the UK.14 Uncertainty regarding the cost-effectiveness of TIPSS may be reflected in National Institute for Health and Care Excellence (NICE) guidelines which include ‘consider’ rather than ‘offer’ recommendation for TIPSS for RA.14–16
The aim of this study was to examine the cost-effectiveness of TIPSS using ePTFE covered stents in the UK, for the following indications:
Indication 1: Patients with cirrhosis, haemodynamically stable variceal bleeding and moderate to severe hepatic dysfunction. Pre-emptive TIPSS is delivered within the first 72 hours of the index bleed following first-line EBL and drug therapy. The comparator is continued EBL and drug therapy.
Indication 2: Patients with cirrhosis and RA. The comparator is LVP plus albumin.
Methodology
A cost-utility analysis was conducted for a UK population adopting methods specified by NICE16 including costs incurred by the NHS and personal social services and health benefits measured as quality-adjusted life years (QALYs). The incremental cost-effectiveness ratio (ICER) of TIPSS versus standard care was estimated using a cost-effectiveness threshold of £20 000/QALY. A discount rate of 3.5% was applied to costs and QALYs.16 The impact of TIPSS on healthcare resources, primarily hospital bed-days, was also reported.
Authors DT, GA and DP provided expert clinical advice as key opinion leaders (KOLs) to:
Validate the model structure, treatment pathways, clinical data and model parameters for TIPSS and standard care.
Provide costs where no published data were available.
Economic model
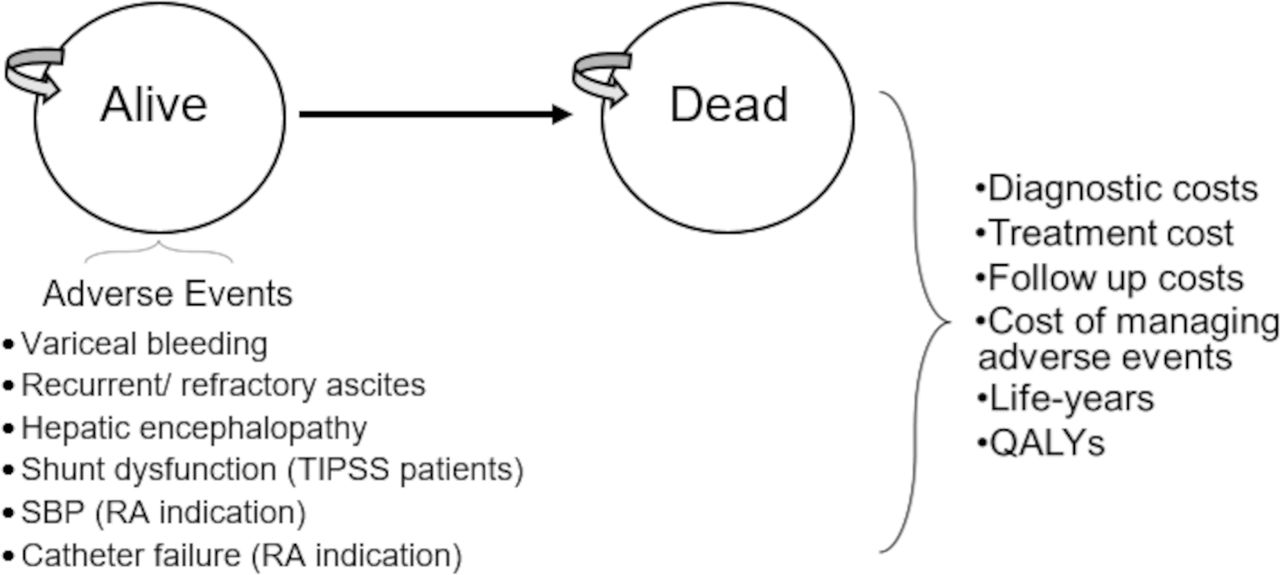
A Markov model was developed with health states of ‘alive’ and ‘dead’, over a 2-year time horizon, with cycle lengths equal to 1 month with a half-cycle correction (figure 1). Monthly all-cause mortality rates were estimated based on survival curves sourced from RCT evidence. Key adverse events associated with liver cirrhosis were assigned per cycle to the ‘alive’ population based on monthly probabilities. Three adverse events were assigned to all populations: variceal bleeding, recurrent and RA and HE, classified as mild (grade I or II) or severe (grade III or IV).17 Shunt dysfunction was included as a procedure-related adverse event for TIPSS. Spontaneous bacterial peritonitis (SBP) and catheter failure were included as adverse events for RA populations receiving standard care. To avoid double counting, we did not include specific mortality risk per adverse event as these were captured within the all-cause rates.
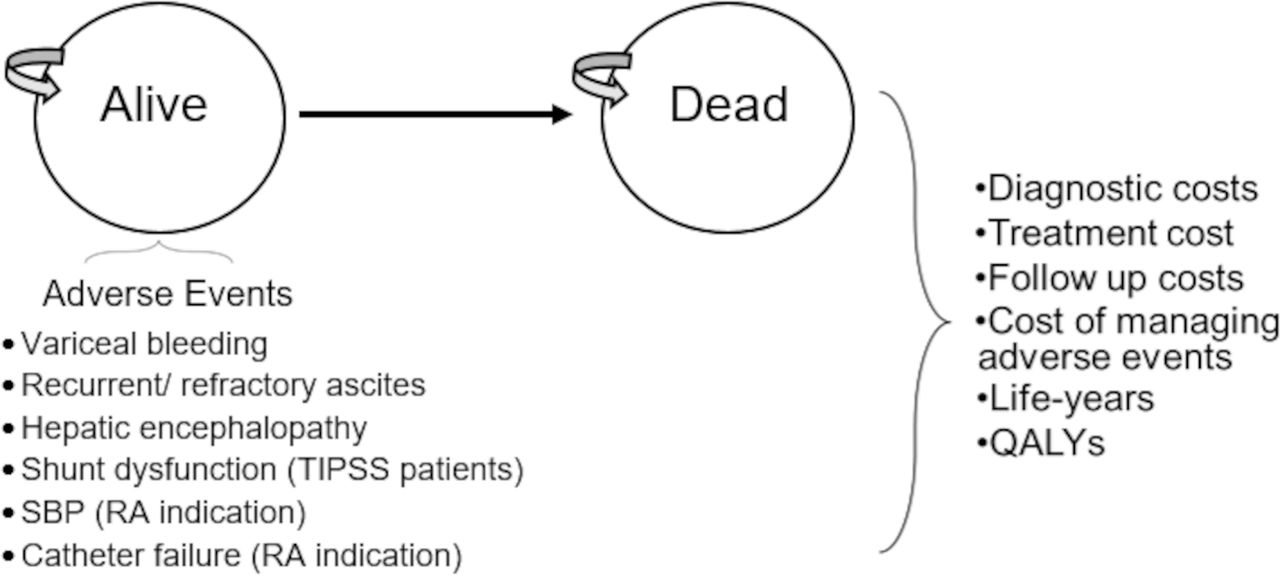
Structure of the Markov model. QALY, quality-adjusted life year; RA, refractory ascites; SBP, spontaneous bacterial peritonitis; TIPSS, transjugular intrahepatic stent shunt.
Prior to entering the model, TIPSS populations were assigned to a treatment pathway based on procedural technical success rates. Where TIPSS resulted in a technical failure, patients entered the standard care arm.
In both arms, the following are summed:
Total costs of: relevant diagnostics, treatments, follow-up and management of complications/adverse events.
Total QALYs.
Population and clinical pathways
The analysis was conducted for two indications recommended by UK clinical guidelines for TIPSS.12–15
Indication 1
Patients with cirrhosis and variceal bleeding who were haemodynamically stable. Populations received a pre-emptive TIPSS procedure within 72 hours of the index bleed, following first-line treatment with EBL and pharmaceuticals. The population were age 18 or over including both Child’s C and B disease with a maximum score of 13. Patients in whom acute variceal bleeding was refractory to endoscopic and pharmacological measures who received salvage TIPSS were excluded. The comparator, standard care, comprised of:
Four outpatient EBL sessions, during the first 2 months
Three follow-up outpatient EBL sessions at 6, 12 and 24 months.
A beta-blocker (either carvedilol, propranolol or nadolol).
Indication 2
Patients with cirrhosis and RA. Refractory status was defined as per UK guidelines, that is, ascites that cannot be mobilised or early recurrence of which (after therapeutic paracentesis) cannot be prevented by medical therapy.13 TIPSS was performed as an elective inpatient procedure following initial treatment with LVP. The comparator, standard care, comprised of further LVP and albumin. KOLs advised that patients in standard care with RA would require LVP sessions every 14 days.
In both indications, common exclusion criteria for TIPSS included: significant pulmonary hypertension, heart failure, rapidly progressing liver failure, severe or uncontrolled HE, sepsis, unrelieved biliary obstruction, primary or metastatic hepatic malignancy and polycystic liver disease.12
Model parameters
Clinical parameters
Clinical parameters were identified through a systematic literature review (online supplemental appendix 1).18 In summary, an electronic literature search was conducted for clinical, safety and economic studies of TIPSS in portal hypertension, oesophageal and gastric varices and ascites. After deduplication, 5502 remained for screening, 5209 were excluded at title and abstract review, with 293 included for full text review. In total, 10 RCTs and 10 economic studies were identified.
Supplemental material
Indication 1—variceal bleeding
Base case parameter values were informed predominantly by the Garcia-Pagán et al RCT.10 The study reported actuarial probabilities of survival at 12 months equal to 86% (TIPSS) and 61% (EBL), with no additional mortality reported between months 12 and 24. Probabilities for adverse events were obtained at 12-month and/or 24-month endpoints as reported by Garcia-Pagán et al.10
Indication 2—refractory ascites
Bureau et al was considered to be the most relevant RCT, reporting 12-month actuarial survival curves for TIPSS versus LVP in RA.11 We calculated survival probabilities at 24 months by constructing parametric survival curves with a log normal survival function based on the 12-month patient data in Bureau et al (online supplemental appendix 2).11
Clinical parameter values are reported in table 1. All values were converted to rates per month to align with the model’s cycle duration. Where published data were only available across a 12-month time horizon, monthly event rates for months 1–12 were applied across the full 24 months. All data were obtained from RCTs or meta-analyses excluding two observational studies which informed the technical success rate for TIPSS, equal to 98%,19 and the rate of catheter failure for patients with LVP equal to 3.8%.20 In addition, we followed methods by Shen et al21 and applied a conservative assumption for the rate of recurrent bleeding for TIPSS patients in the RA indication, set equal to 4.4% as opposed to 0% in Bureau et al.11
Clinical parameters
Healthcare resource usage and unit costs
TIPSS and standard care
We conducted pragmatic literature searches of UK and European clinical guidelines and economic studies to identify resource use and unit costs. Resources required for the preoperative, intraoperative and postoperative phases of TIPSS were extracted from UK clinical guidelines.12 13 The KOLs estimated an average length of stay equal to 2 days per elective and 5 days per non-elective TIPSS. Costs per excess bed day were calculated from NHS reference costs as weighted average across TIPSS tariffs YR16A and YR16B.22 Resources for standard care were identified from published literature, with KOLs advising on consistency with UK clinical practice. Unit costs were from national databases,22–24 with gaps informed by the KOLs. The model used 2017/2018 prices. Dossiers reporting the resources and unit cost were reviewed by KOLs, in an iterative process, until a consensus was reached.
Resource and unit cost for TIPSS and standard care are summarised in table 2 and fully detailed in online supplemental appendix 3. TIPSS for variceal bleeds were non-elective, costing £5398; TIPSS for RA were elective, costing £4646 per procedure. All cases of technical failure had an additional procedure time of 2 hours and required an additional VIATORR stent. In comparison, standard care costs for variceal bleeding (EBL plus beta-blockers) were £3862, per patient assuming 24-month survival. Standard care costs for RA were £800 per LVP session, occurring every 14 days, summing to £41 618 per patient assuming 24-month survival.
Resource usage, unit and total costs (2017/2018 prices) and utilities
Complications and adverse events
Table 2 and online supplemental appendix 3 detail the treatment assumptions applied per adverse event. In brief, a TIPSS shunt dysfunction required reintervention with a balloon catheter costing £4095. Variceal bleeding episodes were treated with terlipressin and required an inpatient/emergency hospital stay and cost £3081. Fifty per cent of variceal bleeding episodes for patients with RA were treated with TIPSS, 14% received a further EBL session and 36% were managed by watchful waiting, giving an average cost of £6454 per episode.
Uncomplicated moderate ascites13 were treated with spironolactone (£5.90), while uncomplicated large ascites required 1.2 sessions with LVP and albumin (£960).
Lactulose (1 month) and rifaximin (6 months) to treat mild HE (grade I & II) cost £91 per month. Twenty-five per cent of severe HE (grade III and IV) cases received a TIPSS reduction procedure, with the remainder managed on rifaximin for 6 months, giving an average cost of £1377.
Antibiotics, albumin and hospital bed-days per SBP episode were estimated to cost £1308, while catheter failure was estimated to cost £552.
Utilities
Utility values were identified through a pragmatic literature search, including handsearching of the 10 retrieved economic studies. Baseline utilities for the bleeding indication were 0.67 for Child-Pugh B and 0.56 for Child-Pugh C.25 We applied population weightings by Child-Pugh B/C in line with the Garcia-Pagan (2010) RCT population,10 resulting in a baseline utility for variceal bleeding of 0.62.
A baseline utility of 0.65 for people with liver cirrhosis without ascites was obtained from Moscucci et al.26
Disutilities were applied to each adverse event. Disutilities of 0.15 for TIPSS procedures, including shunt dysfunction were applied during the hospital stay.27 All other disutilities were applied to the full month cycle and are reported in table 2.
Sensitivity and scenario analyses
Extensive deterministic sensitivity analysis (DSA) was conducted across ranges equal to the 95% CI or ±15% of the mean if CIs were unavailable. Results were plotted on Tornado diagrams to identify key drivers of cost-effectiveness. Threshold analyses for several influential parameters determined the lower/upper bounds for TIPSS to be cost-effective and cost saving vs standard care.
Probabilistic sensitivity analysis (PSA) was conducted using 10 000 iterations to establish the uncertainty in the cost-effectiveness results given the combined uncertainty of the parameter values. All probabilistic parameter distributions followed recommendations by Briggs et al (online supplemental appendix 4).28
Scenario analyses were conducted for the variceal bleeding indication using clinical parameters from a random effects meta-analysis (online supplemental appendix 1), which pooled values from Garcia-Pagán et al10 and a recent UK RCT by Dunne et al.29 The meta-analysis was not used as the base case due to a high risk of bias in Dunne et al where only 13 of 29 participants received ‘early’ TIPSS within 72 hours. As outlined in the Cochrane risk-of-bias tool for RCTs, deviations from the intended interventions can lead to heterogeneity in meta-analyses of intention-to-treat studies.30 Consequently, two scenario analyses were conducted where the meta-analyses included (i) intention-to-treat and (ii) per-protocol data from Dunne et al.29 The clinical parameters for each scenario are presented in table 3; all other parameters retain the values reported in table 1.
Clinical outcomes used in scenario analyses for variceal bleeding
In the RA indication, a scenario analysis was conducted reducing the frequency of LVP sessions from 2.17 per month to 0.71 per month, this value being informed by findings from a UK observational study by Parker et al.31 In addition, two scenario analyses were conducted which applied the Weibull and exponential distributions as the parametric function used to estimate 24-month survival as opposed to the log normal distribution used in the base case analysis (online supplemental appendix 2).
Results
Results from the base-case and scenario analyses are reported in table 4, with Tornado diagrams presented in online supplemental appendix 5.
Deterministic results: TIPSS vs standard care, mean outcomes per person
TIPSS for variceal bleeding
In the base case analysis, TIPSS had 0.209 additional QALYs and NHS savings of £600 per person when compared with EBL and pharmaceuticals. Hence, TIPSS dominated standard care. Savings were predominantly related to treatment (£4059) and hospital stay (£1949) for recurrent bleeding episodes. NHS savings due to reductions in adverse events outweighed the average cost of £5613 per patient for a TIPSS procedure and subsequent hospital stay. The major resource saving (per 1000 population) was 400 fewer bed-days for TIPSS compared with standard care (23 vs 424). There were also fewer HE events (44 vs 52), ascites events (25 vs 55) and angiographies (4 vs 53).
TIPSS remained cost-effective for both scenario analyses, but was no longer cost saving. The incremental costs of TIPSS was equal to £445 (scenario 1) and £372 (scenario 2) while incremental QALYs were equal to 0.21 (scenario 1) and 0.22 (scenario 2). The resultant ICERs for scenarios 1 and 2 were well below the £20 000/QALY threshold and equal to £4128 and £3267, respectively.
The base case results were also sensitive to changes in EBL survival rates, TIPSS procedural costs and the cost and frequency of EBL procedures. TIPSS was cost incurring for these DSAs but cost saving for all others. In all DSAs, ICERs remained below £20 000/QALY. Threshold analyses established that TIPSS would remain cost-saving if the frequency of outpatient EBL procedures for the initial bleed reduced from 4.00 to 2.82, the technical success rate for TIPSS reduced from 98% to 88%, and if the cost per non-elective bed day for TIPSS patients increased from £442 to £995.
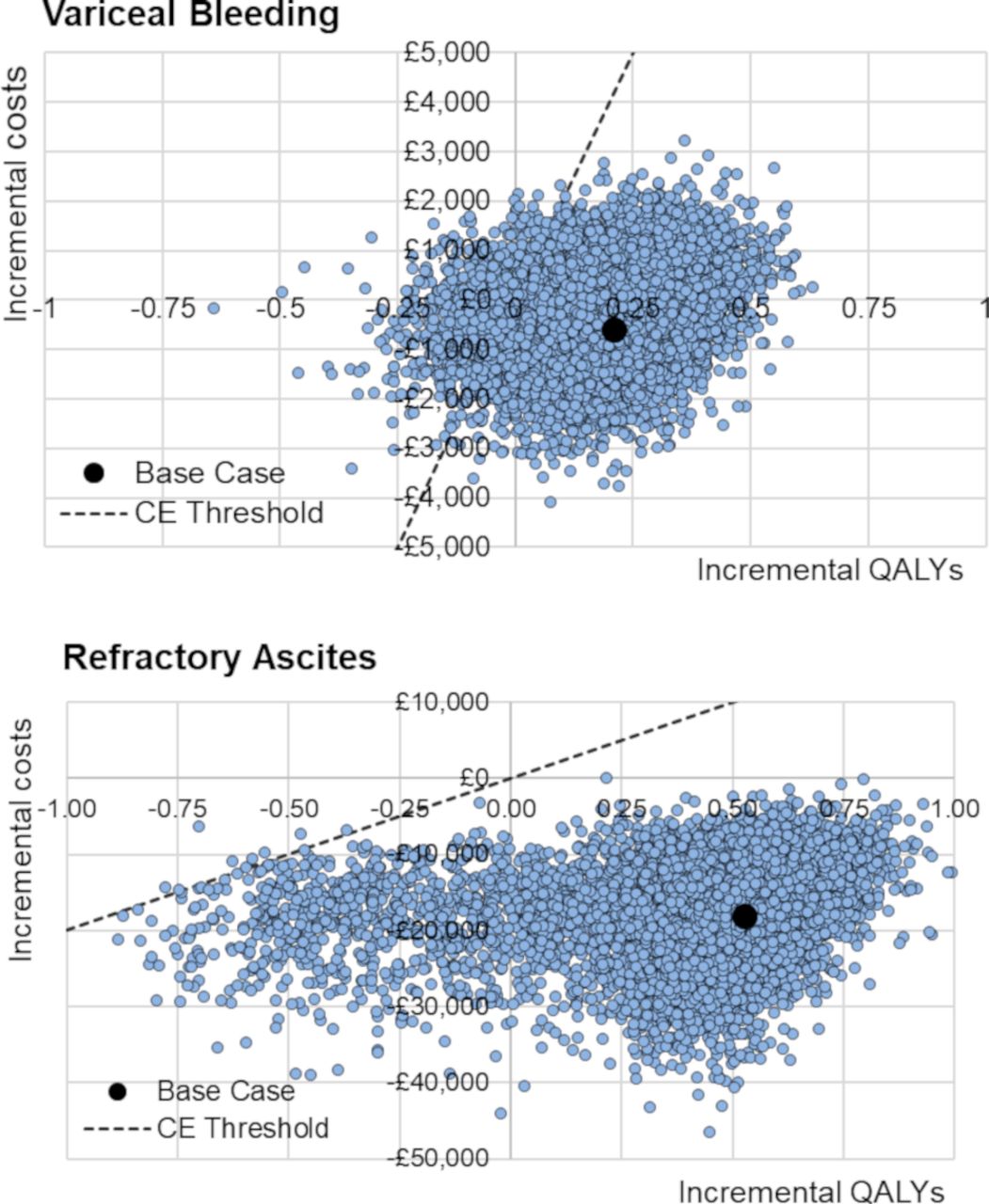
PSA results are displayed in figure 2. TIPSS was cost-effective in 95% and cost-saving in 75% of 10 000 iterations.

{kind=link}
{kind=link}
PSA results. PSA, probabilistic sensitivity analysis; QALY, quality-adjusted life year; CE, cost-effectiveness.
TIPSS for refractory ascites
In the base-case analysis, TIPSS resulted in 0.526 additional QALYs and NHS savings of £17 983 per patient versus LVP. Hence, TIPSS dominated standard care. TIPSS substantially increased survival resulting in 0.630 incremental life-years gained per patient. The major savings were from avoided LVP sessions. Each person treated with LVP incurred £22 322 additional costs to manage ascites over 24 months. These exceeded the average cost of £4877 per patient for a TIPSS procedure. TIPSS also saved £452 from fewer variceal bleeds, £116 from reduced cases of SBP and £116 from fewer catheter failures; however, there was an increase of £31 for HE (table 3). The major resource saving for TIPSS versus LVP (per 1000 population) was 4550 fewer bed-days (446 vs 4996). There were also fewer recurrent bleeds (9 vs 15) but more episodes of mild HE (49 vs 17). SBP and catheter failure had event rates of 7 and 5, respectively, in standard care.1
Results were robust across all DSA scenarios with TIPSS remaining cost saving. This included scenarios which reduced the frequency of LVP sessions from 2.17 per month to 0.71 per month, consistent with findings from an observational study by Parker et al31 and applied different functions to estimate 24-month survival (online supplemental appendix 2).
PSA results are displayed in figure 2. TIPSS was cost-saving in all 10 000 iterations. There was, however, uncertainty in the value of cost savings associated with TIPSS which ranged substantially from a minimum of £29 to a maximum of £46 608.
Discussion
Key findings
Our analysis suggests that TIPSS with an ePTFE covered stent is cost-saving and cost-effective in the UK, for patients with cirrhosis and variceal bleeding or RA. The results are driven by reductions in reinterventions for bleeding and RA. In particular, TIPSS was highly cost-saving for the RA indication, including across all sensitivity analyses.
While TIPSS was dominant (QALY gains and cost savings) in the base case for the bleeding indication, TIPSS was not cost saving in either of the scenario analyses. The uncertainty was due to large differences in recurrent bleeding rates (base case: 3% TIPSS, 50% standard care; scenario 1: 7% TIPSS, 36.7% standard care; scenario 2: 2.9% TIPSS, 36.7% standard care) which accounted for 86% of the total difference in NHS costs between scenarios. We suggest that further research is required to support robust economic modelling results for this indication.
Consistency with other studies
Our economic searches did not identify any UK-based cost-utility analyses indicating this is the first UK economic evaluation of ePTFE covered stents for either indication. Our results are in line with two cost-utility analyses conducted in the USA, by Shen et al21 and Kwan et al,32 where TIPSS was highly cost-effective, although neither found TIPSS to be cost-saving. Differences may have occurred due to the shorter time horizon (1 year) adopted by Shen et al,21 and the use of bare metal stents studies to inform clinical parameters by Kwan et al.32
Our results in RA are consistent with a real-world retrospective cost analysis by Parker et al of 24 TIPSS patients with RA managed at an NHS hospital.31 Mean savings using TIPSS as opposed to LVP with albumin were £2759 per person (2012/2013 prices) which increased to £4570 per person when removing an outlier.31 Cost savings were higher for TIPSS in our analysis (£17 983) due to larger number of LVP sessions, equal to 2.17 per month. When reducing the number of LVP sessions to 0.71 per month, as observed by Parker et al,31 we identified similar levels of cost savings for TIPSS, equal to £2053.
Limitations
There was considerable uncertainty in the cost-effectiveness of pre-emptive TIPSS compared with EBL for the bleeding indication due to limitations in the clinical evidence. It was not considered appropriate to use the meta-analysis for the base case analysis due to the high risk of bias associated with the Dunne et al29 study; thus, the clinical parameters were informed predominantly from a single RCT.10
A major concern regarding the study by Garcia-Pagán et al10 is the small sample (n=63) and imprecise parameter values. In particular, the rate of variceal bleeding for TIPSS versus EBL had a 95% CI ranging from 25% to 69%. Imprecision in the clinical parameters did not translate to high levels of uncertainty in the PSA, where TIPSS had a 95% and 75% probability of being cost-effective and cost-saving, respectively. However, in our most pessimistic scenario, application of the lower 95% CI changed the result of the cost analysis where TIPSS became cost incurring to the NHS.
A second concern relates to improvements in standard care, including survival, since the Garcia-Pagán et al10 RCT.33 Propranolol was used in the standard care arm10 while Dunne et al29 adopted more recent practice with 62% of patients treated with carvedilol. The latter may have a greater effect on portal pressure although there are no data to confirm this in secondary prophylaxis. This and other improvements in cirrhosis care may account for some of the increased survival observed between the two studies, rising from 61%10 to 76%.29 Increased survival for standard care may not impact the cost-effectiveness results materially as survival for TIPSS patients is likely to substantially exceed current standard care.
A third concern relates to patient selection. Our results are not specific by Child-Pugh classification as in Garcia-Pagan (2010) about half of patients were class B and half class C.10 A recent editorial noted several observational studies have shown survival benefit of TIPSS in Child‐C but not in Child‐B patients, regardless of active bleeding. It concluded that large multicentre RCTs are necessary to draw firm conclusions on survival benefit of TIPSS in all high‐risk groups.34
The RA indication was also limited by the use of the single study by Bureau et al11 to inform the majority of parameter values. Again, there were limitations with study size (n=62) and also generalisability of French data to the UK setting. Any biases in the RCT design will be applicable to the economic results, for example, alcohol cessation is identified as a potential confounder for improved liver function by Bureau et al.11 In addition, Bureau et al11 excluded patients requiring more than six LVPs within the previous 3 months. Our base-case analysis modelled patients who require six LVPs every 3 months and thus at the extreme range of disease severity included in the RCT, but this was supported by KOL opinion. Uncertainties in the clinical parameters did not, however, translate to decision uncertainty for the RA indication: TIPSS remained dominant across all sensitivity analyses and was cost-effective and cost-saving in 100% of the PSA iterations.
There was additional uncertainty in other parameter values. For the bleeding indication, TIPSS was cost-effective but not cost-saving when follow-up EBL sessions during the first 2 months for standard care were reduced below 2.82. Dunne (2020)29 report a median of 4 (range 0 to 8) elective EBL procedures over 12 months for 29 patients receiving standard care; however, this outcome was not well reported and may not be directly comparable to the number of EBL sessions in our model which are conditional on survival. Across both indications, no intervention specific utilities were applied and all included values came from low quality and somewhat dated studies that did not apply the EQ-5D measure preferred in the NICE reference case. However, the values are reasonably consistent with the recent NICE cirrhosis guideline which reported no difference in utilities between TIPSS and LVP.14
Finally, our analysis relied on tariff price for the estimation of in-hospital costs separately for elective (suitable for indication 1 including ICU bed occupancy) and non-elective TIPSS admissions. There may have been relevant costs that were not captured within the tariff such as patient transfer for TIPSS. The cost per bed day threshold analysis indicates tariff excluded costs need to be substantial to alter the findings as such costs are also applicable to recurrent bleeding episodes which have higher rates in standard care.
Future research
Management of the complications of decompensated cirrhosis remains an area of intense research and the treatment landscape is evolving for both indications. For variceal bleeding, the ongoing CALIBRE trial compares carvedilol with EBL in a multicentre UK setting,35 while the benefits of long-term albumin in RA has been reported in the ANSWER trial.36 The ePTFE covered stent has also evolved, with a controlled expansion feature. Early studies of the device suggest improved outcomes for survival and lower adverse events, particularly HE and cardiac complications, which may be due to the improved haemodynamic control of the ePTFE covered stent.37–39
Future economic models will require robust clinical evidence. Future studies should prioritise the inclusion of patients who are treated with contemporaneous standard of care and be powered sufficiently to detect differences on key clinical outcomes. It is critical that clinical trials capture aspects of the service delivery of TIPSS at national level, including optimal volume of procedures, in a multicentre format. Further cost-effectiveness evidence by Child-Pugh subgroup should be obtained when robust clinical evidence becomes available. Analyses would be enhanced by the availability of validated utility or mapped quality of life values.
Conclusion
Using the best available evidence, our study indicates that TIPSS with an ePTFE covered stent improves survival and is cost-effective for the two indications. There is a very high likelihood of TIPSS being cost saving for populations with RA. There is considerably less certainty that pre-emptive TIPSS is cost saving for populations with haemodynamically stable variceal bleeding. An adequately powered RCT capturing the current treatment landscape and quality of life is required to inform robust modelling, particularly for the bleeding indication.
Data availability statement
No data are available.
Ethics statements
Acknowledgments
We thank Thomas Weierma (W.L. Gore and Associates, Tilburg, Netherlands) who supported the study, providing input to the patient pathways, cost inputs and commented on drafts of the manuscript.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors RM: primary author of manuscript and involved in all stages of research including model design, build, review of clinical and economic evidence. FON: involved in design of the study, analysis and interpretation of data; reviewed and edited the manuscript and primary author of several paragraphs. JC: involved in design of the study, analysis and interpretation of data; reviewed and edited the manuscript and primary author of several paragraphs. JT: involved in review of the economic model design and clinical evidence; reviewed and edited the manuscript. DT, DP, GA: provided key clinical input for this research; acted as key opinion leaders (KOLs) and informed parameter values and provided validation for the model design; reviewed and edited the manuscript.
Funding This work was funded by W.L. Gore & Associates. W.L. Gore & Associates were involved in the design of the study, data collection, analysis and interpretation of data as well as the writing of the manuscript.
Competing interests RM is an employee of York Health Economics Consortium who were commissioned by W.L. Gore & Associates to provide consultancy, develop the economic model and write the manuscript.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.