Article Text

Abstract
Objective The differential diagnosis and management of seronegative enteropathies is challenging due to the rarity of these conditions, the overlap of clinical and histopathological features and the current lack of an international consensus on their nomenclature.
Design This is a narrative review providing pragmatic guide on the investigation and clinical management of seronegative enteropathies in adults based on the available literature and our clinical experience.
Conclusions Seronegative coeliac disease is the most frequent cause among the heterogeneous group of seronegative enteropathies and its diagnosis is confirmed by the clinical and histological response to a gluten-free diet after the exclusion of other causes of villous atrophy. Correct identification and targeted management of seronegative enteropathies is mandatory because of the variation in terms of clinical outcomes and prognosis.
- celiac disease
- gluten free diet
- malabsorption
- small intestinal biopsy
Data availability statement
No data are available. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Villous atrophy (VA) is the histopathological hallmark of many chronic enteropathies, which, despite being aetiologically heterogeneous, can manifest clinically with a malabsorption syndrome. Conventional coeliac disease (CD) and its complications are the major cause of VA, particularly in the Western World.1–4 Diagnosis of CD in adults is based on positive specific serology (IgA tissue transglutaminase-TTA, endomysial antibodies-EmA, deamidated gliadin peptides-DGP) and a certain degree of VA responding to a gluten-free diet (GFD).1 2 When VA occurs in patients without IgA coeliac specific serology (negative IgA EmA/TTA/DGP) the term seronegative enteropathy (SNE) is usually adopted.3 4 This term refers to a group of rare and aetiologically heterogeneous clinical entities, whose common hallmark is duodenal VA (table 1).3–11 Differential diagnosis and clinical management of SNEs is still challenging, because of their rarity, the overlapping clinical and histopathological features and the lack of a standard consensus on the nomenclature and the diagnostic criteria for many of these conditions.3 4 We specify that patients with total IgA deficiency and positive IgG-based coeliac serology (IgG EmA/tTG/DGP) should be diagnosed with CD associated to IgA deficiency, rather than being considered as affected by SNEs.3 4
Aetiological classification of non-coeliac seronegative enteropathies with villous atrophy
In this narrative review, we summarise the current knowledge on SNEs and provide a practical guide on the differential diagnosis and clinical management of these enteropathies in adult patients based on the available literature and our clinical experience.
Epidemiology of SNEs
Non-coeliac enteropathies (NCEs) are rare conditions, although data on the epidemiology are scarce and figures vary according to the population under investigation.
When the denominator consists of all the patients affected by VA, up to 5.1% of patients with VA can have a form of NCE. An Italian referral centre study over 15 years revealed that the remaining 94.9% of patients with VA was due to conventional seropositive CD.8 Conversely, when the general population is considered, the true prevalence of NCEs is still unknown.
There is a limited data on the prevalence of the different aetiologies of NCEs. When the denominator consists of all the patients affected by a form of NCEs, it emerges that, in adults, seronegative coeliac disease (SNCD) is the most common cause of SNEs followed by iatrogenic and infectious causes. Remarkably, in up to 14% of adult patients, a definitive aetiology was not found and a final diagnosis of idiopathic VA/undefined sprue was made.6–10 While conversely, in children, SNCD and iatrogenic causes are virtually absent and the most common aetiologies are inflammatory, infectious and immune-mediated.12 13
When the setting is the general population, there are no data on the prevalence of these enteropathies and it is only possible to make an estimation of how common these conditions may be. For example, prevalence of olmesartan-associated enteropathy, which is certainly the most common form of drug-induced SNEs is estimated to vary in between 1/4000 and 1/5000 case of olmesartan users.3 14 Autoimmune enteropathy has an estimated incidence of 1/million person years.15–18 Gastrointestinal involvement in common variable immunodeficiency (CVID) is frequent, and persistent diarrhoea has been described in up to 20%–60% of cases.19–23 However, the true prevalence of VA in patients affected by CVID is still unknown.3 The prevalence of Whipple’s disease can be estimated around three cases per million people, according to a paper from Northern Italy.24
Finally, as far as SNCD is concerned, although it is the most common aetiology for SNEs,3–10 25 the true prevalence of SNCD among coeliac patients and in the general population still needs to be elucidated. While the first papers on SNCD reported a prevalence of SNCD of 10%–20% of all coeliac patients,26–30 more recent studies show a lower prevalence between 2%–6.5%.8 9 31 These last figures on the prevalence of SNCD among all the coeliac patients are in line with the sensitivity of coeliac specific antibody testing.32 It is still unclear, however, if the difference between the first and the latest figures may be due to a true change in the prevalence of SNCD over the years, the higher sensitivity of Ema and TTA, or to the different diagnostic criteria adopted for this condition.25 There are currently no data on the prevalence of SNCD in the general population.
Long-term outcomes and mortality
Only two papers7 8 have evaluated long-term outcomes in SNEs showing that these enteropathies are characterised by poor prognosis. In the UK paper by Aziz et al7 patients affected by non-coeliac SNEs and those affected by SNCD had a higher mortality than conventional seropositive CD. In the Italian paper by Schiepatti et al, data about development of complications and mortality were provided. 4/260 patients with CD developed complications (type 1 refractory CD, abdominal B-cell lymphoma, small bowel carcinoma and enteropathy-associated T-cell lymphoma), compared with 4/14 SNEs patients, with a complication rate of 0.2 (95% CI 0.1 to 0.6) and 6.3 per 100 person years (95% CI 2.4 to 17.0), respectively.8
4/260 patients died in the CD group (three of unrelated causes and one of enteropathy-associated T-cell lymphoma) and 4/14 in the SNEs group, therefore corresponding to a mortality rate of 0.2 (95% CI 0.1 to 0.6) and 6.0 deaths per 100 person years (95% CI 2.2 to 16), respectively (HR=25.37, 95% CI 6.15 to 104.63, p<0.001).8
However, both the Italian and UK study did not compare risk of complications and mortality in SNCD and in each subtype of NCE to CD.7 8
This is a relevant point, as in our clinical experience it is likely that long-term outcomes are slightly different within the heterogeneous group of NCEs. In fact, while prognosis of SNEs due to an identifiable cause, such as drugs and infections, is usually excellent on removal of the trigger agent, patients affected by CVID, AE, idiopathic VA can develop severe complications worsening their prognosis.3 4 7 8 33–41
Patients affected by CVID enteropathy are burdened by a high mortality,33 39 mainly due to development of infectious and malignant complications. Also patients with AE can develop lymphoproliferative complications,35 40 and an American study showed an increased mortality in patients with AE, comparable to those affected by refractory CD.41
A recent dual-centre Italian-UK study, on forms VA of undetermined origin, also known as idiopathic villous atrophy (IVA), showed that these enteropathies can be subclassified into three main groups, with distinct clinical phenotypes and prognosis.37 IVA group 1 is characterised by forms of transient self-limiting partial VA, likely due to an infectious agent and good prognosis (5-year survival 96%). IVA group 2 is characterised by persistent non-clonal IVA with peculiar association with HLA DQB1*0301 and DQB1*06 and long-term survival (5-year survival was 100%). Finally, IVA group 3 is characterised by a cluster of enteropathies with lymphoproliferative features and poor outcome (5-year survival 27%). Hypoalbuminaemia and age at diagnosis were major predictors of mortality in IVA.
Finally, although a recent UK paper suggested that a more extensive small-bowel disease on capsule endoscopy correlated with a higher mortality (p=0.019) in SNEs,42 a thorough study of clinical predictors of poor long-term outcomes and mortality may be helpful to address the clinical follow-up of these patients.
Seronegative coeliac disease
A minority of coeliac patients present with VA and negative serology at diagnosis. These patients are affected by SNCD. Diagnosis of SNCD is based on the clinical and histological response to a GFD, after the exclusion of other NCEs.3 4 25 In the last years, our understanding of SNCD has been growing and it is likely that different forms of SNCD may exist. According to the literature, forms of true SNCD may be found in an early phase of the disease with a lesser degree of VA, as well as in the late stage of disease (with possible refractory CD or lymphoma) and in dermatitis herpetiformis.25 Remarkably, up to 30% of patients with biopsy proven dermatitis herpetiformis can have a negative serology at diagnosis.43 Forms of SNCD may also rarely occur in the first degree relatives of coeliac patients.44 45 Patients who had already been started on a GFD or steroids/immunosuppressive therapies prior to serological testing may also present with IgA negative TTA/EmA at diagnosis.25 However, when immunosuppressants are withdrawn or a GFD re-started a positive coeliac serology is found in these patients. Therefore, they should be considered as affected by conventional seropositive CD and not by SNCD.25
Debates still exist on whether patients affected by total IgA deficiency who show positive class IgG TTA or IgG EmA and VA should be considered as affected by SNCD. Taking into consideration that these patients generate an IgG-based serological response, this point may be in favour of a diagnosis of conventional seropositive CD instead of that of true SNCD.25 However, comparative data on the clinical phenotypes and long-term outcomes of patients with CD associated with IgA deficiency and SNCD are still lacking.
Finally, some authors suggest that SNCD can be found in association with CVID.46–49 Although this point is highly debated, the histological recovery of VA after gluten withdrawal is the mainstay for confirming CD in this specific setting. Moreover, a negative HLA-DQ2 and DQ8 typing is very useful to rule out CD.48 49 On the contrary, coeliac antibodies have no role in this diagnostic work-up. In fact, class IgG EmA has been found in CVID patients who had previously received intravenous immunoglobulin replacement therapy and in whom CD was excluded, due to the absence of HLA-DQ2 and DQ8 molecules.22 48 49 Finally, certain histopathological features such as absence of plasma cells and the presence of a polymorphonuclear infiltrate and graft-versus-host disease like lesions48–50 were described in patients affected by CVID and duodenal VA but not in untreated CD. However, their role is only supportive for diagnosis of CVID.
Although the main literature findings suggest that patients with SNCD are older at diagnosis and can more frequently present with severe malabsorption,7–9 25 29 there is a lack of clinical data about the long-term follow-up of SNCD.
Clinical features of patients with seronegative enteropathies
In the vast majority of cases, the clinical picture of SNEs is dominated by a severe malabsorption syndrome requiring upper GI endoscopy despite the negative coeliac serology.3 4 According to the literature, adult patients with SNEs (both SNCD and non-CD enteropathies) are older than patients with conventional seropositive CD.3 4 7–9 Therefore, the overlap in presenting symptoms between NCEs, SNCD and complications of CD is certainly a major challenge in the differential diagnosis of these conditions.
Some clinical clues can be useful to guide the differential diagnosis between seronegative CD and non-coeliac SNEs. For example, a thorough pharmacological and travel history can guide towards a diagnosis of iatrogenic forms of SNEs or tropical sprue, respectively. A personal history of primary (such as CVID or IgA deficiency) or secondary immunodeficiency can represent a predisposing factor to giardiasis.3–11 A history of recurrent upper and lower airways infections in early childhood can support the diagnosis of CVID. Finally, for other conditions such as Whipple’s disease, tuberculosis and HIV, VA and a malabsorption syndrome are usually not the typical primary manifestations prompting the diagnosis, especially if other more relevant findings unrelated to malabsorption are not present. For example, Whipple’s disease should be suspected predominantly in middle-aged Caucasians men with a long-lasting history of seronegative arthritis, lymphadenopathy and fever, which anticipates the onset of a severe malabsorption syndrome.24 51 A potentially life-threatening neurological involvement can complete the clinical picture.
Histological features of seronegative enteropathies
Although VA is the key histological feature for NCEs and it is mandatory for the diagnosis, there are currently no specific histological markers allowing the differential diagnosis between SNCD and other non-coeliac SNEs. Some of these histological findings may be supportive for a specific aetiology (see table 1), but need always to be considered in the whole clinical and biochemical scenario. The only two conditions that can be directly diagnosed through histology are giardiasis and Whipple’s disease. However, these two conditions usually do not pose a problem of differential diagnosis with SNCD and other seronegative enteropathies, as VA is not always present and the diagnostic tests are very specific. PCR on duodenal biopsies aspirate or direct identification of Giardia lamblia by the pathologist on formalin-fixed paraffin embedded H&E stained small-bowel specimens are reliable diagnostic methods for making the diagnosis of giardiasis.3 4 Duodenal biopsy showing a periodic acid Shiff staining+diastase resistant macrophagic infiltration of the lamina propria is key to the diagnosis of Whipple’s disease. PCR for Tropheryma whipplei is highly specific but should be reserved for certain sterile sites, such as the central nervous system.51
Traditional histology, immunohistochemistry, flow cytometry and molecular diagnostics (PCR on duodenal specimens for detecting monoclonal rearrangements of gamma/beta-TCR genes) remain the key diagnostic tests for some kind of rare primary lymphoproliferative disorders of the small bowel that can manifest with VA in the uninvolved non-neoplastic mucosa.52 These conditions can pose a problem of differential diagnosis with SNCD and include enteropathy associated T-cell lymphoma- type 1 and type 2, indolent T-cell lymphoproliferative disease of gastrointestinal tract, and immune-proliferative small intestinal disease. Abdomen CT, positron emission tomography (PET)-CT and bone marrow aspiration can complete the diagnostic work-up for these disorders.3 4
Some interest was initially dedicated to intestinal deposits of IgA tTG2 antibodies that were found in the small bowel mucosa of seronegative coeliac patients, but not in other NCEs.29 However, their specificity has recently been questioned,53 so their relevance for differentiating SNCD from other NCEs in everyday clinical practice is still limited.
More recently, it has been suggested that analysis of intraepithelial lymphocytes by means of flow cytometry allows the distinction of SNCD from non-coeliac SNEs on the basis of the so called ‘coeliac lymphogram’.10 54 These methods, however, need to be validated on larger sample sizes.
Serological markers and faecal tests
Enterocyte antibodies (AEA) and dosage of serum immunoglobulins are the most relevant blood test in the differential diagnosis of SNEs.3 4 AEA detected by means of indirect immunofluorescence on monkey jejunum slides are the mainstay for serological diagnosis of AE in adults.16 18 55 In children, also cases of AE with negative AEA have been described, particularly in association with rare and complex immunodeficiency syndromes.56 Although standard diagnostic criteria for the detection of AEA in indirect immunofluorescence are still lacking, on the basis of our clinical experience, we and others suggest that in adult patients with VA unresponsive to a GFD, positive AEA confirm the diagnosis of AE.3 4 16 26 34 35 55 Anti-goblet cell antibodies were also proposed as a further marker for AE.18 However, they are totally non-specific and their use should definitely be discouraged for the diagnosis of AE.3 4 57
A marked decrease of IgG (at least 2 SD below the mean for age) and at least one of either IgM or IgA is required to make a diagnosis of CVID. The following diagnostic criteria must also be fulfilled: onset of immunodeficiency after the age of 2 years; absent isohaemagglutinins and/or poor response to vaccines; exclusion of secondary causes of hypogammaglobulinaemia such as malignancies, drugs, infections and genetic disorders.19
Finally, for giardiasis, identification of cysts or trophozoites in the stool, stool specific Giardia antigens, PCR on duodenal biopsies aspirate or direct identification of the parasite by the pathologist on formalin-fixed paraffin embedded H&E stained small-bowel specimens are reliable diagnostic methods.3 4
Conditions that should not be considered in the differential diagnosis
It has been reported that also small intestinal bacteria overgrowth (SIBO) and Helicobacter pylori may be associated with non-coeliac VA.6–8 However, the strength of evidence is poor for these two conditions. In patients affected by SIBO a wide variety of histological lesions have been reported,58–60 but VA is not a key diagnostic element. Whereas mild VA seems to occur only in the most severe cases of SIBO,6 7 9 in most patients a normal villous architecture has been described.58 59 Moreover, in patients with VA and absence of any predisposing conditions to SIBO a positive glucose H2 breath test is quite likely to be a consequence of the histological lesions themselves rather than their cause.60 Few reports suggest peptic duodenitis with or without H. pylori infection5 7 61 as the cause of SNVA, but there is scarce evidence in favour of its causative role in SNVA.
Methodological approach to differential diagnosis of seronegative enteropathies
Currently, there is no standardised international consensus about the nomenclature and the clinical management of SNEs. However, based on our experience and the recommendations by the American Gastroenterology Association, and other centres with international expertise on SNEs,3–11 we have developed an investigational work-up for the differential diagnosis of SNEs (figure 1).

Algorithm for the differential diagnosis of duodenal villous atrophy. CVID, common variable immunodeficiency; DGP, deamidated gliadin antibodies; EmA, endomysial antibodies; TTA, tissue transglutaminase antibodies.
The first step is the assessment of VA on correctly duodenal specimens taken from the second duodenal portion. It is mandatory to ascertain that investigations leading to the diagnosis of VA were conducted while on a gluten-containing diet, and if not, additional or repeat testing should be performed after gluten-challenge (box 1). For patients with a history of VA, a careful review of duodenal biopsy slides by an expert gastrointestinal pathologist informed about the pharmacological history and clinical features of the patient is mandatory. This means that patients presenting with increased intraepithelial lymphocyte count only, without VA, cannot be considered in this algorithm. Unfortunately, the poor orientation of duodenal specimens still account for a substantial proportion of the diagnostic errors in SNEs, leading to overestimation of seronegative CD and unnecessary treatment.62
Diagnostic panel for differential diagnosis of seronegative enteropathies
Laboratory tests
HLA typing.
Serum IgA, IgG, IgM.
IgA and IgG Ema, TTA and DGP.
Anti-enterocyte antibodies.
HIV testing.
Quantiferon.
Stool tests
Giardia lamblia and other parasites.
Viruses.
Helicobacter pylori antigens.
Faecal calprotectin.
Duodenal biopsies
H&E and PAS staining.
PCR for Giardia, tuberculosis and Whipple’s disease.
Small bowel aspirate.
PCR for beta and gamma-TCR clonality assessment.
Flow cytometry for aberrant IELs.
Other examinations
Capsule endoscopy.
Abdomen CT/PET.
Colonoscopy+biopsies.
The second key requirement is the synchronous presence of negative IgA EmA/ttG/DGP.4
Once VA and negative coeliac antibodies are confirmed, all the possible aetiologies must be excluded before considering the possibility of SNCD or IVA.3 4 25 37 In this regard, a pertinent pharmacological and clinical history, together with specific laboratory and molecular tests can guide clinicians to the appropriate diagnosis in a substantial number of cases (table 1). HLA typing for DQ2.5 (DQA1*05, DQB1*0201), DQ2.2 (DQA1*02, DQB1*0202), DQ8 (DQA1*03, DQB1*0302) and DQ7.5 (DQA1*05, DQB1*0301) should be carefully considered, particularly when negative in order to exclude SNCD.3 4 25
Clinical management and follow-up of seronegative enteropathies
The optimal management of SNEs is still unknown. Data from major referral centres have tried to address the issue of the differential diagnosis of SNVA, but there is still a complete lack of data on the best treatment options and timing for clinical and endoscopic follow-up of these patients.
Based on our clinical experience, we propose the following options for the treatment and follow-up of these patients.
Treatment
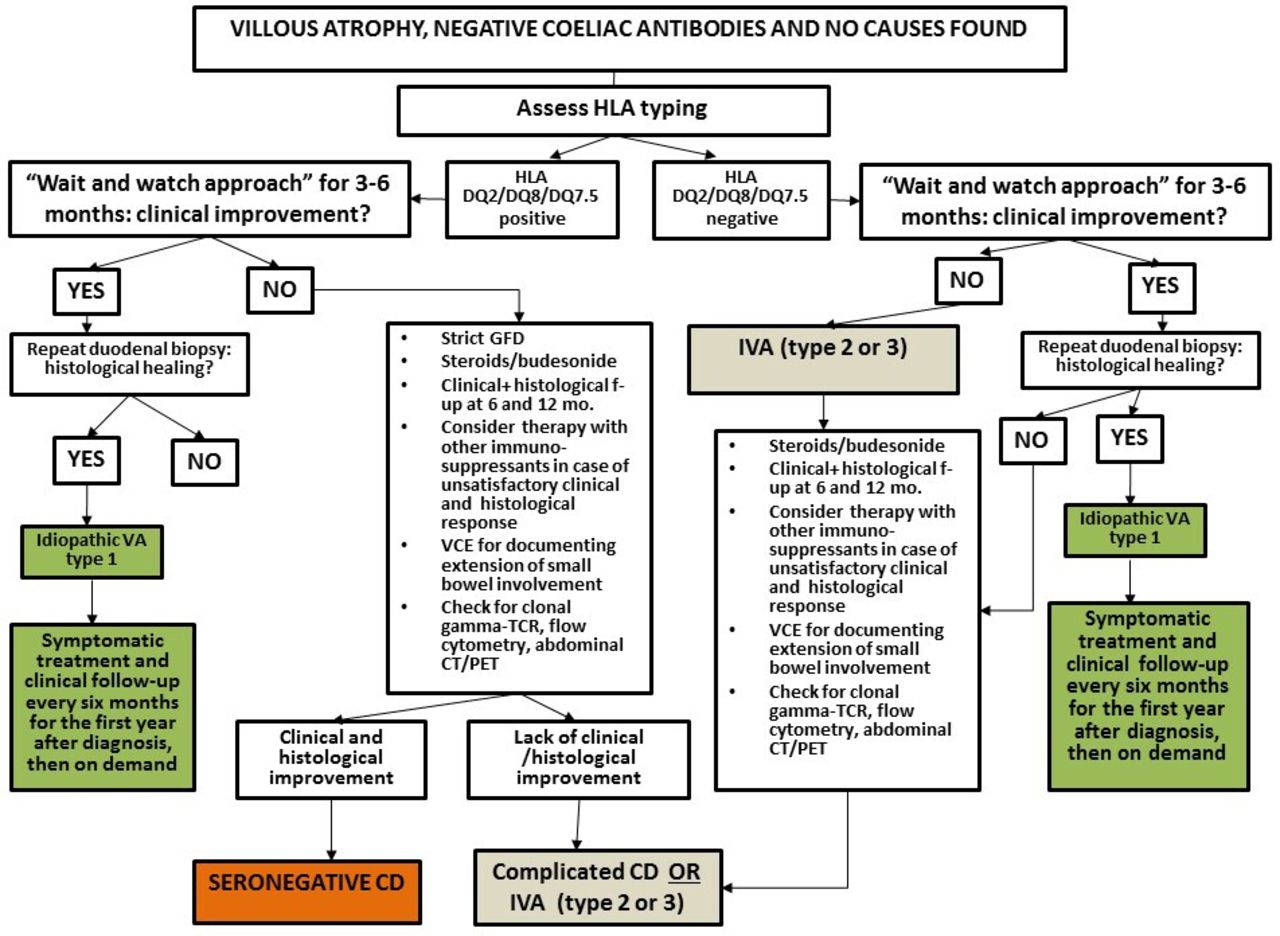
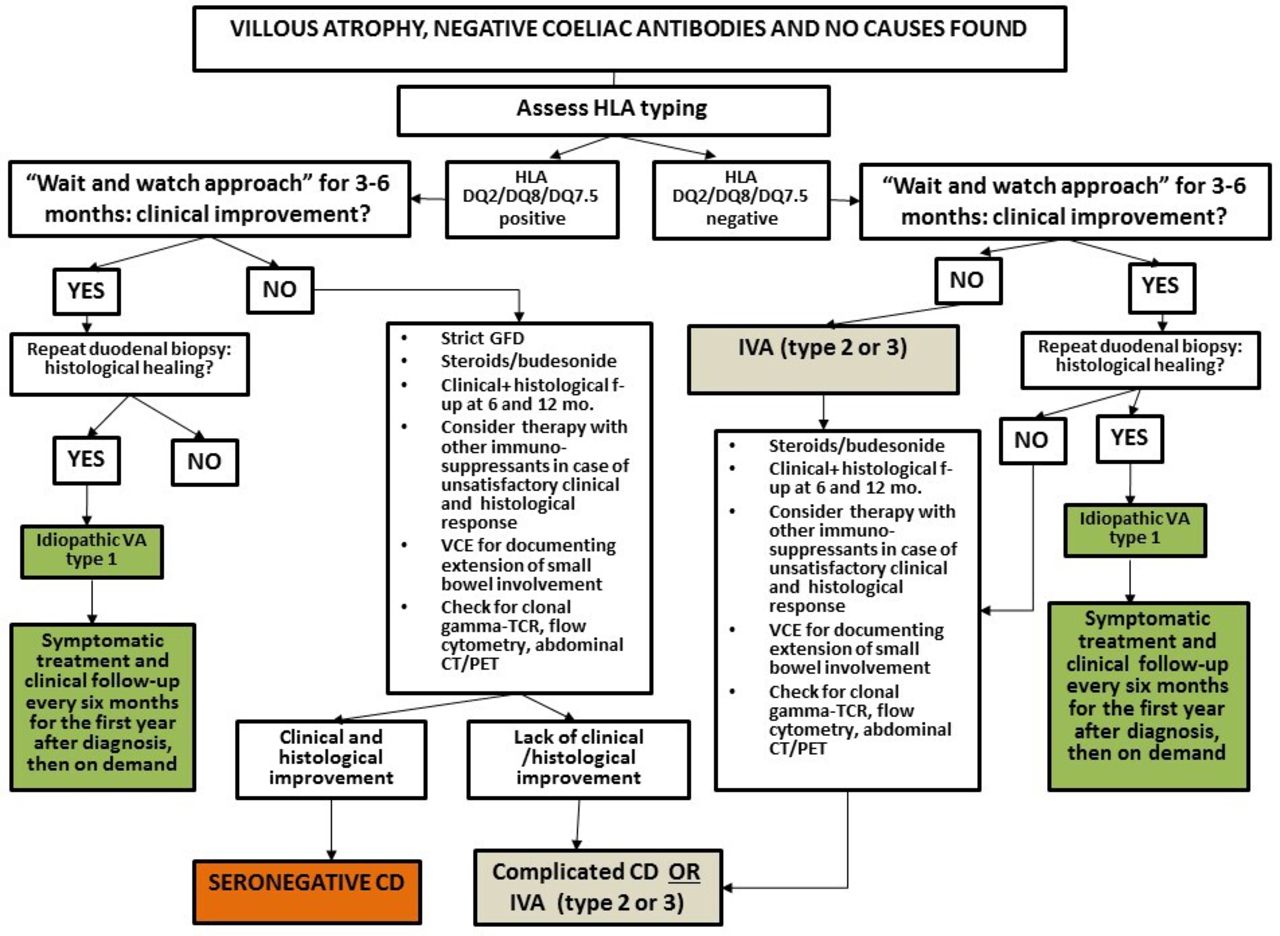
While for patients affected by SNEs due to a known cause, the treatment depends on the underlying aetiology (see table 1), it is still unclear what the best approach for patients with SNEs and no identifiable cause should be. Although histological response to a GFD is the mainstay for diagnosing SNCD, uncertainties still exist about the correct timing for a patient affected by SNVA, positive HLA-DQ2/DQ8/DQ7.5 and negative investigations to be started on a GFD. We think that it can be reasonable to take into account factors such as ethnicity, HLA typing and severity of the clinical picture and length of involved small-bowel on capsule endoscopy3 4 7 37 42 to guide the decision on whether or not to start a GFD. We suggest that in Caucasian patients carrying HLA-DQ2/DQ8 and in whom no alternative aetiology has been found, a GFD could be started. In patients with these characteristics and presenting with severe features of malabsorption and age >50 years corticosteroids followed by oral budesonide may be considered to promote mucosal recovery. Parenteral nutrition should be considered for patients with severe malabsorption and malnutrition. In patients with no cause found for VA, mild symptoms and absence of laboratory abnormalities at diagnosis (IVA 1), it may be reasonable to adopt a ‘watch and wait’ approach and a histological follow-up, as this resulted in histological recovery of VA within 12 months from diagnosis.3 7 37 Figure 2 shows a flow chart for the diagnosis and management of SNCD and idiopathic forms of VA.
{kind=link}
{kind=link}
Flow-chart for the diagnosis and management of seronegative coeliac disease and IVA. CD, coeliac disease; GFD, gluten-free diet; IVA, idiopathic villous atrophy; PET, positron emission tomography; VCE, video capsule endoscopy; TCR, T-cell receptor.
Follow-up
Given the risk of poor long-term outcomes in SNEs,3 4 7 8 we strongly recommend a strict clinical and endoscopic follow-up in these patients, regardless of the underlying cause. While it could be debatable whether to perform a follow-up duodenal biopsy in patients with SNEs due to an identifiable and reversible cause (such as iatrogenic) and in whom a complete and satisfactory clinical response to treatment has occurred, we believe it is mandatory to document both histological recovery and extension of the involved small-bowel by means of VCE in patients with SNCD, CVID, autoimmune enteropathy, IVA, iatrogenic causes and lymphomas.
Conclusions
Differential diagnosis and clinical management of SNEs in adults are still challenging, and in the absence of specific international guidelines, pitfalls are still common. In our review, we have suggested investigation and management strategies based on expert opinion, which we hope can nevertheless be helpful and largely pragmatic, despite the lack of a true evidence base.
A systematic and algorithmic approach may be useful to appropriately categorise these patients and treat them accordingly. Assessment of histological response to treatment is the mainstay to make the diagnosis of SNCD, but also to guide clinical management and follow-up of the other forms of SNEs.
Future research perspectives may include the development of standard consensus guidelines for the diagnosis and a better definition of natural history of different forms of SNEs. Identification of molecular mechanisms beyond SNVA will also be precious to develop biomarkers and target therapies, particularly for patients at higher risk of poor outcomes.
Data availability statement
No data are available. Not applicable.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors AS and DSS conceived the study. AS drafted the manuscript with MC, FB and DSS. DSS revised the study for important intellectual content. All the authors approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.